การใช้ยาลดระดับน้ำตาลในเลือดอย่างสมเหตุผล ในกลุ่มผู้ป่วยเบาหวาน ภญ. สุพิชชา อยู่สุข เภสัชกรชำนาญการ โรงพยาบาลสุรินทร์
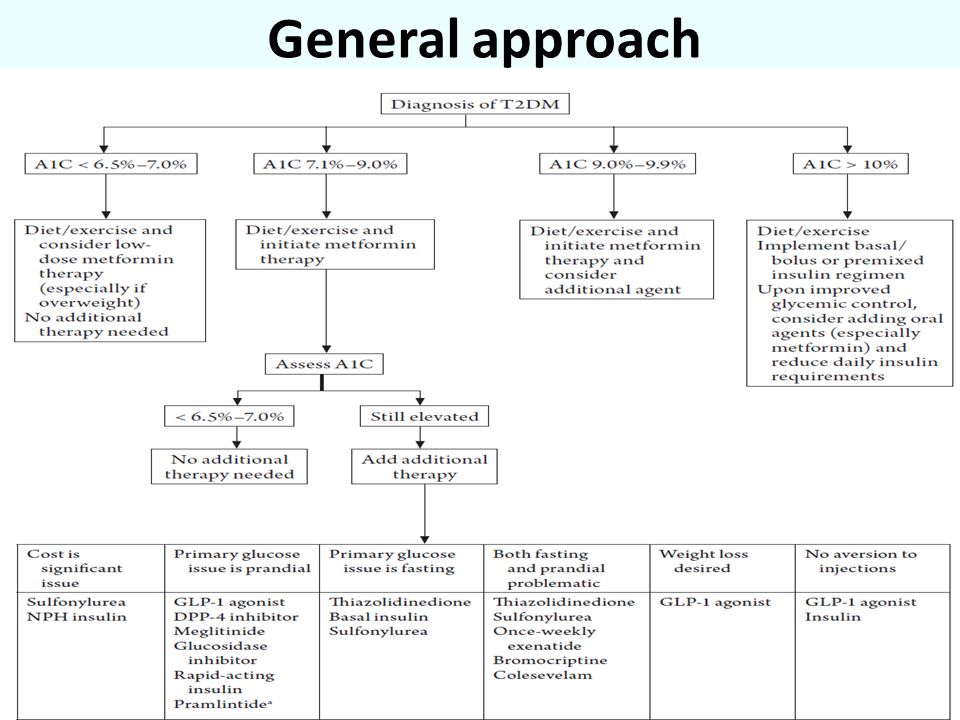
General approach
T2DM Drug Therapy Recommendations
ยาลดระดับน้ำตาลในเลือด (Antihyperglycemic Drug) Sulfonylurea ---glipizide, glibenclamide Rapid acting insulin secretagogue--repaglitanide Biguanides --metformin Thiazolidinediones----Pioglitazone (Actos) Alpha-glucosidase inhibitor---Acarbose DPP-4 inhibitors---sitagliptin (Januvia) SGLT2 inhibitors---Canagliptin Insulin
กลไกการออกฤทธิ์ของยาลดระดับน้ำตาลในเลือด
สูตรโครงสร้าง
Sulfonylurea Effects on the -cell Ca++ VDCC (+) Depolarization -Cell K+ATP Channel Free Ca++ [ATP] [ADP] K+ Slide 7: Nateglinide Effects in the -cell In Vitro The therapeutic effects of a number of oral antidiabetic drugs, including repaglinide, glyburide and nateglinide, derive from the ability of the agents to increase glucose-stimulated insulin secretion. These drugs, referred to as “insulin secretion agents,” bind to specific receptors on the insulin-secreting beta cells on or within the pancreas. This results in closure of KATP channels to which the receptors are coupled, leading to depolarization of the cell membrane and opening of voltage-dependent calcium channels. The subsequent influx of extracellular calcium ions triggers the release of insulin. The rate of onset of action of the different insulin secretion agents depends upon the speed of their interactions with their respective beta cell receptors, and whether or not they require internalization. The rate at which nateglinide binds to its beta cell receptor is significantly faster than that of repaglinide and comparable to that of glyburide. However, unlike nateglinide, glyburide requires internalization into beta-cells in order to exert its actions. Moreover, the prolonged presence of glyburide inside the cell may well contribute to the significantly shorter duration of action of glyburide at both the level of KATP channel closure and prolonged duration of insulin secretion. It is unclear whether internalization of repaglinide is required for stimulation of insulin secretion. These drugs may also be stimulating insulin secretion via other mechanisms than closing KATP channels. SUR Metabolism Sulfonylurea Insulin Release Glucose J Pharmacol Exp Ther 2000;293:444–52
Sulfonylureas Hemoglobin A1C lowering of 1%–2% Decreases FPG ~ 50 - 70 mg/dl (minimal decrease in postprandial) The higher the baseline HbA1C the greater the effect Fifty percent of maximal dose begets 80% of drug efficacy A 5%–10% primary failure rate; 5%–10%/year secondary failure rate
Elimination (M=hepatic metabolism Comparison Drugs Initial dose Dosage range(mg/day) Elimination (M=hepatic metabolism R=Renal) Glibenclamide, Glyburide (Daonil) 2.5–5.0 mg once or twice daily 2.5–20 50%M,R Gliclazide (Diamicron) 80 mg once or twice daily 40-320 (30-120 for MR) M, 80%R Glipizide (Minidiab) 5 mg once or twice daily 90% M, R Glimepiride (Amaryl) 1–2 mg once daily 1–8 40% M, 60%R Gliquidone (Glurinor) 15 mg once daily 15-120 95% M, 5%R
Sulfonylureas Adverse effects: Hypoglycemia Weight gain Contraindications: Hypersensitivity to sulfonamides Diabetic ketoacidosis Type 1 DM Severe liver or kidney disease Hypoglycemic unawareness (Beware for NPO) Adverse effects: Hypoglycemia Weight gain Less common: Rash, photosensitivity, dyspepsia, nausea/vomiting, headache
ADR Weight gain Hypoglycemia Headache ไม่ควรใช้ glibenclamide ในผู้ป่วยที่มีการทำงานของไตบกพร่อง (Scr > 1.5 mg/dl หรือมี GFR < 30 ml/min/1.73 m2) ระวังในผู้ป่วยที่มีประวัติแพ้ยา sulfa
Rapid acting non-sulfonylurea insulin secretagogue
Meglitinides Very similar to that of sulfonylureas in increasing insulin secretion from the pancreas but with a more rapid onset and shorter duration of activity Glucose-dependent activity A1C reduction: Repaglinide 1.6%, Nateglinide 0.8%, Mitiglinide 1.3% Most effective on postprandial glucose excursions Metabolize by CYP 2C8, 3A4
Meglitinides Mitiglinide(Glufast) Repaglinide(Novonorm) Initial: 5 mg 3 times daily with meals Maximum dose : 20 mg 3 times daily Repaglinide(Novonorm) Initial: 0.5–1 mg 15 minutes before meals Maximal daily dose: 16 mg Nateglinide(Starlix) 60-120 mg 15 minutes before meals 60 mg if A1C near goal Can be increased in weekly intervals if needed If skip a meal, skip medication
Meglitinides Adverse effects: Hypoglycemia (though less than with sulfonylureas), weight gain, upper respiratory infection Contraindications/precautions DM type 1, DKA Hypoglycemia unawareness Caution in concomitant use of repaglinide and gemfibrozil, can lead to greatly increased repaglinide levels
Biguanide
Metformin---ลดระดับน้ำตาลในเลือดได้โดย
The Biguanide Effect Inhibit oxidative metabolism Increases NADH Suppresses gluconeogenesis Decreases the GI absorption of glucose Intracellular redox potential shifts from aerobic to anaerobic metabolism Decrease in pyruvate carboxylase activity (rate limiting enzyme in the formation of glucose from lactate) results in decreased hepatic metabolism of lactate Symptoms: acidosis, nausea, vomiting, increased respiratory rate, abdominal pain, shock, and tachycardia
Metformin Primarily inhibits hepatic glucose production Secondarily some improvement of peripheral insulin resistance May decrease intestinal absorption of glucose (small intestine) Hemoglobin A1C lowering of 1%–2% Primarily reduces FBG(~ 50 - 70 mg/dl) 5%–10% per year secondary failure rate
Metformin Improved CV outcomes No hypoglycemia as monotherapy Positive lipid effects 500 mg once or twice daily with food to start (decrease GI adverse effects) May take 2-4 weeks to see maximum benefit Maximal dose: 2550 mg/day Common dose: 1 g 2 times/day
The Cardiovascular Effects of Metformin
metformin In meta-analysis, metformin in Type 1 DM ; reduce insulin requirements (6.6/day, P< 0.001), small reductions in weight Small totol and LDL cholesterol Not improved glycemic control (absolute A1C reduction 0.11%, P = 0.42)
Metformin Adverse effects: Contraindications: Serum creatinine of 1.5 mg/dL or greater in men; serum creatinine of 1.4 mg/dL or greater in women Creatinine clearance less than 30 mL/minute Severe hepatic, pulmonary, or cardiac disease Hold for 24 hours before procedures using contrast dye Excessive alcohol intake Hypoxemia, dehydration, or sepsis Adverse effects: Common: Nausea, vomiting, diarrhea, gas, upset stomach, metallic taste (especially early) Weight loss Uncommon: Macrocytic anemia (caused by vitamin B12 deficiency); lactic acidosis (uncommon but life threatening! Use only in appropriate patients)
อาการไม่พึงประสงค์ แก้ไขโดย กินหลังอาหารทันทีช่วยได้ คลื่นไส้อาเจียน ปวดท้อง ท้องเสีย ท้องผูก hypoglycemia แก้ไขโดย กินหลังอาหารทันทีช่วยได้ อมลูกอมหรือผสมน้ำหวานจิบบรรเทาอาการน้ำตาลในเลือดต่ำ
MALA (Metformin-associated Lactic Acidosis) เกิดน้อยแต่รุนแรง
MALA พบประมาณ 2-9 คน/100,000 คน/ปี มีโอกาสเสียชีวิต 30-50% ตรวจพบปริมาณ lactate ในเลือด > 5 mmol/L และค่า PH ในเลือด < 7.35 คลื่นไส้ /อาเจียน หายใจเร็ว ปวดท้อง ซึม,หมดสติ ความดันโลหิตต่ำ หัวใจเต้นเร็ว, หัวใจเต้นผิดจังหวะ ปัจจัยเสี่ยงที่ทำให้เกิด MALA เช่น การได้รับ metformin ในปริมาณต่อวันสูงกว่า 2,500 mg (เม็ดละ 500 mg) หรือขนาด 2,550 mg (เม็ดละ 850 mg), ผู้ป่วยสูงอายุ, การทำงานของไตบกพร่อง
Alpha-glucosidase Inhibitor
กลไกการออกฤทธิ์
α-Glucosidase inhibitors Inhibits the enzyme α-glucosidase, found along the brush border of the small intestine, which is responsible for the breakdown of complex carbohydrates into glucose, thus delaying and reducing post-meal carbohydrate absorption and postprandial blood glucose Hemoglobin A1C reduction of 0.5%–1% Reduces postprandial blood glucose Mealtime dosing
α-Glucosidase Inhibitors Efficacy: Lowers HgA1C ~ 0.7 - 1% Better post-prandial blood glucose control but fasting glucose levels are relatively unchanged Better with starchy, high fiber diets
α-Glucosidase inhibitors Acarbose(Glucobay) : 25 mg with first bite of meal; start every day and then increase weekly to 2 times/day; then 3 times/day with meals to decrease GI adverse effects (Maximal daily dose: 300 mg) Miglitol(Glyset) : 25 mg with first bite of meal Voglibose(Basen): 0.2-0.3 mg with first bite of meal (Maximal daily dose: 0.9 mg) Initiate at very low dose and increase gradually over months Skip if meal skipped
α-Glucosidase Inhibitors Possible side effects: Flatulence Abdominal pain Upset stomach Diarrhea May diminish after 4–8 weeks of therapy Increased liver enzymes observed with high doses of acarbose
α-Glucosidase Inhibitors Warnings and Precautions: Gastrointestinal disorders (Irritable Bowel Disease, bowel obstruction, colon ulcerations, malabsorption etc) Liver disease (potential hepatotoxicity) Creatinine clearance less than 25 mL/minute or serum creatinine greater than 2 mg/dL
Thiazodinedione
กลไกการออกฤทธิ์
Thiazolidinediones Often called TZDs or glitazones Peroxisome proliferator-activated receptor (PPAR) gamma agonist (found in adipose tissue, skeletal muscle, and the liver) Increase in insulin-dependent glucose disposal (insulin sensitivity) in skeletal muscle and adipocytes (primarily) and a decrease in hepatic glucose production (secondarily) Rosiglitazone and Pioglitazone
Thiazolidinediones Efficacy: Lowers HgA1C ~ 0.5 – 1.5% Decreases FPG ~ 50-80 mg/dl Only effective in the presence of insulin Both drugs increase HDL-C, but pioglitazone has a more favorable effect in reducing LDL-C Onset: 4 weeks and maximum benefit in 2-3 months
Thiazolidinediones Pioglitazone(Actos) Rosiglitazone(Avandia) Initial: 15 mg once daily Maximal daily dose: 45 mg Rosiglitazone(Avandia) Initial: 1–2 mg once daily Maximal daily dose: 8 mg Dose titration is slower with these agents, and the maximal effect of a dose change may not be observed for 8–12 weeks
Thiazolidinediones Possible side effects: Edema (particularly peripheral edema) Weight gain Headache, Weakness Nausea, vomiting, abdominal pain Bone fracture Increase the risk of heart failure Liver problems (RARE) Pioglitazone associated with small risk of bladder cancer Potential myocardial infarctions (rosiglitazone)
Thiazolidinediones Contraindications: Active liver disease; LFTs >2.5 times ULN Type 1 diabetes (ineffective without insulin) Diabetic ketoacidosis Heart Failure - NYHA class III or IV (causes plasma volume expansion)
ควรตรวจวัดการทำงานของตับก่อนเริ่มยา และในช่วงรักษา หากค่าการเอนไซม์ของตับขึ้นมากกว่า 2 เท่าของค่าปกติควรหยุดยา
DPP-4 inhibitor (Dipeptidyl Peptidase Inhibitor-4)
กลไกการออกฤทธิ์
Dipeptidyl peptidase-4 inhibitors Active GLP-1 Dipeptidyl peptidase-IV Inhibitors Dipeptidyl peptidase-IV Inactive GLP-1
Dipeptidyl peptidase-4 inhibitors Inhibits the enzyme dipeptidyl peptidase-4 from breaking down endogenous GLP-1 and GIP, resulting in increased endogenous incretin levels. This results in Glucose-dependent increase in insulin secretion Glucose-dependent inhibition of glucagon secretion
Dipeptidyl peptidase-4 inhibitors Hemoglobin A1c lowering of 0.5%–1.1% Reduces primarily postprandial glucose Weight neutral Sitagliptin(Januvia) Saxagliptin(Onglyza) Vildagliptin(Galvus) Alogliptin(Nesina): 25 mg/day(Reduced in renal impairment) Linagliptin(Trajenta): 5 mg/day(No dose adjustment in renal impairment)
Allow in mild to moderate Comparison Profile Sitagliptin Vildagliptin Saxagliptin Indication Mono or Combo with SU, MFM, TZD Insulin combination Yes No data Normal dose 100 mg OD 50 mg OD-BID 5mg OD GFR 30-50 50 mg OD Contraindicated 2.5 mg OD GFR<30 25 mg OD ESRD with dialysis Hepatic inpairment Allow in mild to moderate Not recommend
Dipeptidyl peptidase-4 inhibitors Contraindications: History of pancreatitis Diabetic ketoacidosis Type 1 DM Adverse effects: Placebo-like incidence of adverse effects (URI, headache, UTI) Hypoglycemia with monotherapy is minimal, but increased frequency with concurrent sulfonylurea therapy Sitagliptin has had some postmarketing reports of acute pancreatitis, angioedema, Stevens-Johnson syndrome, and anaphylaxis
The Kidneys Play an Important Role in Glucose Control Normal Renal Glucose Physiology 180 g of glucose is filtered each day Virtually all glucose reabsorbed in the proximal tubules & reenters the circulation SGLT2 reabsorbs about 90% of the glucose SGLT1 reabsorbs about 10% of the glucose Virtually no glucose excreted in urine Mather, A & Pollock, C. Kidney International. 2011;79:S1-S6.
Sodium- Glucose Cotransporters SGLT1 SGLT2 Site Mostly intestine with some kidney Almost exclusively kidney Sugar Specificity Glucose or galactose Glucose Affinity for glucose High Km= 0.4 Mm Low Km = 2 Mm Capacity for glucose transport Role Dietary glucose absorption Renal glucose reabsorption Lee YJ, at al. Kidney Int Suppl. 2007;72:S27-S35.
Targeting the Kidney Chao EC, et al. Nat Rev Drug Discovery. 2010;9:551-559.
Mechanism of Action of SGLT2 Inhibitors Inhibition of SGLT2 Reversal of glucotoxicity Insulin sensitivity in muscle ↑ GLUT4 translocation ↑ Insulin signaling Other SGLT2 inhibitors improve glucose control by reducing plasma glucose levels, which in turn reverses the effects of glucotoxicity, as follows: Insulin sensitivity in muscle increases via increased GLUT4 translocation and insulin signaling as well as other mechanisms. Insulin sensitivity also improves in the liver, with a decrease in glucose-6-phosphatase levels. Gluconeogenesis in the liver decreases as a result of a reduction in the Cori cycle and decreased PEP carboxykinase. β-Cell function improves. Insulin sensitivity in liver ↓ Glucose- 6-phosphatase Gluconeogenesis Decreased Cori cycle ↓ PEP carboxykinase -Cell function 55 55
SGLT2 Inhibitors Dapagliflozin(Farxiga) : 5-10 mg daily Canagliflozin(Invokana): 100-300 mg daily Reducing A1C by 0.55%–0.89% The long-term safety of this class remains to be proven Risk of nocturia and genitourinary infections may limit use in some patients SGLT2 inhibition may not be effective in patients with renal impairment
Perspectives on SGLT2 Inhibition Potential advantages Insulin Independence Weight loss (75g urine glucose = 300kcal/day) Low risk of hypoglycemia Blood pressure lowering? Concerns Polyuria Electrolyte disturbances Bacterial urinary tract infections Fungal genital infections Malignancies
Insulin ใช้ลดระดับน้ำตาลในเลือดในผู้ป่วยเบาหวานชนิดที่ 1 และ 2
Human Insulin 51 amino acids
Human Insulin Analog
Action of Insulin www.en.wikipedia.org Effect of insulin on glucose uptake and metabolism. Insulin binds to its receptor (1) which in turn starts many protein activation cascades (2). These include: translocation of Glut-4 transporter to the plasma membrane and influx of glucose (3), glycogen synthesis (4), glycolysis (5) and fatty acid synthesis (6). www.en.wikipedia.org
Insulin classification Rapid acting insulin: Aspart, Lispro Short acting insulin: Regular Intermediate acting insulin: NPH, Lente Long acting insulin: Ultralente, Glargine, Detemir
Insulin Fixed - Mix products Advantages “Easy” to use – usually two injections per day Not necessary to mix prior to administering (already mixed) Available in insulin pens
Insulin’s Pharmacokinetics Distribution: throughtout the extracellulars fluids, no plasma protein binding Metabolism: mainly in the liver Excretion: filtered through the glomeruli and completely(98%) reabsorbed in the proximal tubules
Type Drug Name Onset Peak Duration Rapid-Acting Aspart 5-15 minutes (10-20) 1-2 hours 4-6 hours Lispro (15-30) Glulisine (US) Short-Acting Regular 0.5-1 hour 2-5 hours 6-10 hours
Type Drug Name Onset Peak Duration Intermediate- Acting NPH 1-2 hrs 4-8 hrs 10-20 hrs Intermediate to Long Acting Detemir (US) 2-4 hrs 6-8 hrs 3-4h (0.2-0.4) 5.7-23.2 hrs 14h (0.2-0.4) Long-Acting Glargine Not significant (Flat) ~24 hrs
Insulin Dosing of Rapid and Short Acting Agents Type Drug Name Meal Timing Rapid-Acting Aspart ▪ 5-15 minutes before meals ▪ With first bite of food Lispro Glulisine 5-15 minutes before meals and up to 20 minutes after meals Short-Acting Regular 30 minutes before meals Regular
Insulin and Dosing of Intermediate & Long-Acting Agents Type Drug Name Meal Timing Intermediate- Acting NPH Within 15 minutes before meals when mixed with rapid-acting insulin; 30 minutes before meals when mixed with regular Long-Acting Glargine Not applicable
รูปแบบการให้บริหารอินซูลินใน ผู้ป่วยเบาหวาน type2 Basal insulin รักษาระดับกลูโคสให้คงที่ ให้ NPH หรือ Lante เช้าและก่อนนอน Continuous subcutaneous insulin infusion (CSII) Insulin gargline วันละ 1-2 ครั้ง Prandial insulin หลั่งออกมาเพื่อนำกลูโคสเข้าไปในเซลล์ + ยับยั้งการปลดปล่อยกลูโคสจากตับ Insulin aspart, insulin lispro หรือ regular insulin ก่อนอาหารทุกมื้อ Correction-dose insulin ควบคุมน้ำตาลที่มาจากสภาวะอื่น เช่น ได้รับ steroid
วิธีการบริหารอินซูลิน One daily insulin regimen ให้ NPH หรือ insulin gargline หรือ pre-mixed insulin 70/30 มื้อก่อนนอน Multiple dose insulin injection (MDI) ให้ regular insulin หรือ aspart หรือ lispro ก่อนอาหารทุกมื้อ + intermediate insulin เช้าและก่อนนอน Split and mixed insulin regimen ให้อินซูลินวันละ 2 มื้อ โดยให้ intermediate insulin + regular insulin หรือ aspart หรือ lispro ก่อนอาหารเช้า เย็น
วิธีการบริหารอินซูลิน Split and mixed insulin program with bedtime intermediate insulin ฉีด intermediate insulin + regular or insulin analog เช้า และ ฉีด regular or insulin analog และ ฉีด intermediate insulin ก่อนนอน continuous subcutaneous insulin infusion (CSII) ใช้เครื่องช่วยผลัก rapid-acting insulin analog เข้าสู่ร่างกายตลอดเวลา Intravenous insulin infusion
Morning hyperglycaemia Feature comparing Dawn phenomenon Somogyi effect Definition Recurring early morning hyperglycaemia Early morning hyperglycaemia due to treatment with excessive amount of exogenous insulin Cause Decrease of insulin secretion between 3a.m. and 5a.m. Nocturnal hypoglycemia due to excessive dose of insulin Diagnosis (3 a.m. and 5 a.m. glucose level) High/normal plasma glucose level Low plasma glucose level
Morning hyperglycaemia Somogyi effect Shift RI to NPH before bedtime Decrease insulin dose before bedtime Long-acting insulin analogues Go to bed with higher level of plasma glucose than usual Dawn phenomenon Increase insulin dose before bedtime Long-acting insulin analogues
Dawn phenomenon
Somogyi effect
กราฟเปรียบเทียบ down phenomenon กับ Somogyi effect
Insulin inj (vial)
Novomix flexpen (Insulin Aspart) Insulin gargline
Penfill
continuous subcutaneous insulin infusion (CSII)
Insulin storage & Shelf life -Unopened: 2-8๐ C -Opened: <30๐ C Shelf life -Unopened: (2-8๐ C) until expired date (15-30๐ C) 28 days -Opened: 28 days (independ on temperature)
Adverse Reactions of Insulin Possible Side Effects: Low blood sugar (Hypoglycemia) Weight gain Injection site reaction
Adverse Reactions of Insulin Hypoglycemic Symptoms Lipodystrophy Sweating / Fast Heartbeat / Shaking Blurred Vision / Hunger / Dizziness Irritable / Headache / Weakness www.bddiabetes.co.uk/dyn_en/what_is_lipodystrophy.html
When can Hypoglycemia occur? Eat too little food Delay or skip a meal or snack Exercise harder or longer than usual Take too much medicine or insulin Sickness Drink alcohol on an empty stomach
Diabetes Checklist 1. Hemoglobin A1c of 7% or less (6.5%) (not consistent with goals listed above) 2. Blood pressure 140/80 mm Hg or less (ACEI/ARB) 3. Low-density lipoprotein cholesterol of 100 (70) mg/dL or less (statin) 4. Daily ASA use for vascular protection 5. Smoking cessation 6. Immunizations (influenza, pneumococcal, HBV)
Diabetes Checklist 7. Urinalysis 8. Daily feet inspection 9. Annual dilated eye examinations 10. Realistic exercise program 11. Weight loss (5%–10%) 12. Dental examinations (peridontal disease)
Thank you