ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Neonatal Resuscitation
พ.ญ.พรมนัส พันธุ์สุจริตไทย 17 สิงหาคม 2554

2
Neonatal resuscitation
1. คาดการณ์ล่วงหน้า ประเมินปัจจัยเสี่ยง -ก่อนคลอด -ระหว่างคลอด 2. การเตรียมทีม 3. การเตรียมอุปกรณ์ที่ครบถ้วน 4. ประเมินทารกถูกต้องและสามารถปฏิบัติกู้ชีพ ได้อย่างเหมาะสมและทันท่วงที

3
ทารกคนใดที่ต้องการการช่วยกู้ชีพ
ประมาณ 10% ต้องการการช่วยเหลือเพียงเล็กน้อย เพื่อให้สามารถเริ่มต้นหายใจเอง 1% ที่ต้องการการช่วยกู้ชีพ มากกว่า 90% สามารถหายใจได้เองและ เปลี่ยนแปลงระบบการไหลเวียนโลหิตมาสู่ภาวะหลัง เกิดได้ โดยไม่ต้องการ หรือต้องการการช่วยเหลือ เพียงเล็กน้อย Which babies require resuscitation? Most newly born babies are vigorous. About 10% of newborns require some assistance to begin breathing at birth. Only about 1% need extensive resuscitation measures (intubation, chest compressions, and/or medications) to survive. Instructor Tip: Practice resuscitation skills frequently, especially if skills are not used often. This may be done with “mock codes.”
 to survive. Instructor Tip: Practice resuscitation skills frequently, especially if skills are not used often. This may be done with mock codes.")
4
การเตรียมการช่วยกู้ชีพทารก: ปัจจัยเสี่ยง
การช่วยกู้ชีพทารกส่วนใหญ่ สามารถรู้และเตรียม การณ์ล่วงหน้าได้ โดยการสอบถามถึงปัจจัยเสี่ยงก่อน คลอด และขณะคลอด ที่อาจต้องการการช่วยกู้ชีพ ทารก In many cases, delivery of a depressed newborn can be anticipated on the basis of the antepartum and intrapartum history.

5
ปัจจัยเสี่ยงก่อนคลอด
ทบทวนปัจจัยเสี่ยง ปัจจัยเสี่ยงก่อนคลอด มารดาเป็นเบาหวาน ภาวะความดันโลหิตสูงจากการตั้งครรภ์ โรคความดันโลหิตสูงเรื้อรัง ภาวะซีดของทารกหรือ isoimmunization เคยมีบุตรเสียชีวิตในครรภ์หรือหลังคลอด ภาวะเลือดออกในไตรมาสที่สองหรือสาม ภาวะติดเชื้อในมารดา ภาวะเจ็บป่วยเรื้อรังในมารดา เช่น โรคหัวใจ โรคไต โรคปอด โรคของ ต่อมธัยรอยด์ หรือ โรคระบบประสาท ครรภ์แฝดน้ำ (Polyhydramnios) ภาวะน้ำคร่ำน้อย (Oligohydramnios) ถุงน้ำคร่ำแตกก่อนกำหนด (Premature rupture of membranes) ภาวะบวมของทารกในครรภ์ (Fetal hydrops) ครรภ์เกินกำหนด (Post-term gestation) ครรภ์แฝด (Multiple gestation) น้ำหนักตัวเบี่ยงเบนจากอายุครรภ์ การได้รับยาบางชนิดในมารดา เช่น แมกนีเซียม (magnesium), adrenergic- blocking drugs การใช้ยาเสพติดในมารดา ทารกพิการแต่กำเนิด (Fetal malformation or anomalies) ทารกในครรภ์ดิ้นน้อยลง มารดาไม่ได้ฝากครรภ์ มารดาอายุน้อยกว่า 16 ปีหรือมากกว่า 35 ปี
 ภาวะน้ำคร่ำน้อย (Oligohydramnios) ถุงน้ำคร่ำแตกก่อนกำหนด (Premature. rupture of membranes) ภาวะบวมของทารกในครรภ์ (Fetal. hydrops) ครรภ์เกินกำหนด (Post-term gestation) ครรภ์แฝด (Multiple gestation) น้ำหนักตัวเบี่ยงเบนจากอายุครรภ์ การได้รับยาบางชนิดในมารดา เช่น. แมกนีเซียม (magnesium), adrenergic- blocking drugs. การใช้ยาเสพติดในมารดา. ทารกพิการแต่กำเนิด (Fetal malformation. or anomalies) ทารกในครรภ์ดิ้นน้อยลง. มารดาไม่ได้ฝากครรภ์ มารดาอายุน้อยกว่า 16 ปีหรือมากกว่า 35 ปี")
6
ทบทวนปัจจัยเสี่ยง ปัจจัยเสี่ยงขณะคลอด การทำผ่าตัดฉุกเฉินทางหน้าท้อง
(Emergency cesarean section) การช่วยคลอดด้วยคีมหรือเครื่องดูด สุญญากาศ (Forceps or vacuum assisted delivery) ทารกท่าก้นหรือท่าผิดปกติ การคลอดก่อนกำหนด การคลอดอย่างรวดเร็วผิดปกติ (Precipitous labor) การติดเชื้อในถุงน้ำคร่ำ Chorioamnionitis) ถุงน้ำแตกก่อนคลอดนาน (>18 ชั่วโมง ก่อนคลอด) ระยะการคลอดนานเกินปกติ (>24 ชั่วโมง) การคลอดระยะที่ 2 นานเกินปกติ (>2 ทารกตัวใหญ่ (Macrosomia) ทารกในครรภ์มีอัตราการเต้นของหัวใจช้า ผิดปกติ (Persistent fetal bradycardia) การเต้นของหัวใจทารกในครรภ์มีลักษณะ non-reassuring การใช้ยาดมสลบ มดลูกหดเกร็งมากกว่าปกติ (Uterine hyperstimulation) มารดาได้รับยากดประสาท (Narcotics) ภายใน 4 ชั่วโมงก่อนคลอด ภาวะขี้เทาปนในน้ำคร่ำ (Meconium- stained amniotic fluid) สายสะดือย้อย (Prolapsed cord) ภาวะรกลอกตัวก่อนกำหนด (Abruptio placentae) ภาวะรกเกาะต่ำ (Placenta previa) ภาวะเสียเลือดมากในขณะคลอด
 การช่วยคลอดด้วยคีมหรือเครื่องดูด. สุญญากาศ (Forceps or vacuum. assisted delivery) ทารกท่าก้นหรือท่าผิดปกติ การคลอดก่อนกำหนด. การคลอดอย่างรวดเร็วผิดปกติ (Precipitous labor) การติดเชื้อในถุงน้ำคร่ำ. Chorioamnionitis) ถุงน้ำแตกก่อนคลอดนาน (>18 ชั่วโมง. ก่อนคลอด) ระยะการคลอดนานเกินปกติ (>24. ชั่วโมง) การคลอดระยะที่ 2 นานเกินปกติ (>2. ทารกตัวใหญ่ (Macrosomia) ทารกในครรภ์มีอัตราการเต้นของหัวใจช้า. ผิดปกติ (Persistent fetal bradycardia) การเต้นของหัวใจทารกในครรภ์มีลักษณะ. non-reassuring. การใช้ยาดมสลบ. มดลูกหดเกร็งมากกว่าปกติ (Uterine. hyperstimulation) มารดาได้รับยากดประสาท (Narcotics) ภายใน 4 ชั่วโมงก่อนคลอด. ภาวะขี้เทาปนในน้ำคร่ำ (Meconium- stained amniotic fluid) สายสะดือย้อย (Prolapsed cord) ภาวะรกลอกตัวก่อนกำหนด (Abruptio. placentae) ภาวะรกเกาะต่ำ (Placenta previa) ภาวะเสียเลือดมากในขณะคลอด.")
7
อาการแสดงของทารกที่มีปัญหาขาดออกซิเจน
ความตึงตัวของกล้ามเนื้อ (muscle tone) ลดลง ภาวะกดการหายใจ (respiratory depression) อัตราการเต้นของหัวใจช้าลง (bradycardia) ความดันโลหิตต่ำ ภาวะหายใจเร็ว (tachypnea) เขียว (cyanosis) เขียวและความตึงตัวของกล้ามเนื้อปกติ เขียวและความตึงตัวของกล้ามเนื้อลดลง The compromised baby may exhibit one or more of the following clinical findings: Poor muscle tone Depression of respiratory drive due to insufficient oxygen reaching the brain Bradycardia Low blood pressure Cyanosis (blue color) Tachypnea (rapid respirations) Other conditions, such as infection, hypoglycemia, or depressant drugs given to the mother before birth, may also cause these symptoms.
 ลดลง. ภาวะกดการหายใจ (respiratory depression) อัตราการเต้นของหัวใจช้าลง (bradycardia) ความดันโลหิตต่ำ. ภาวะหายใจเร็ว (tachypnea) เขียว (cyanosis) เขียวและความตึงตัวของกล้ามเนื้อปกติ เขียวและความตึงตัวของกล้ามเนื้อลดลง. The compromised baby may exhibit one or more of the following clinical findings: Poor muscle tone. Depression of respiratory drive due to insufficient oxygen reaching the brain. Bradycardia. Low blood pressure. Cyanosis (blue color) Tachypnea (rapid respirations) Other conditions, such as infection, hypoglycemia, or depressant drugs given to the mother before birth, may also cause these symptoms.")
9
ขั้นตอนเบื้องต้น (A) A แรกเกิด ให้ความอบอุ่น
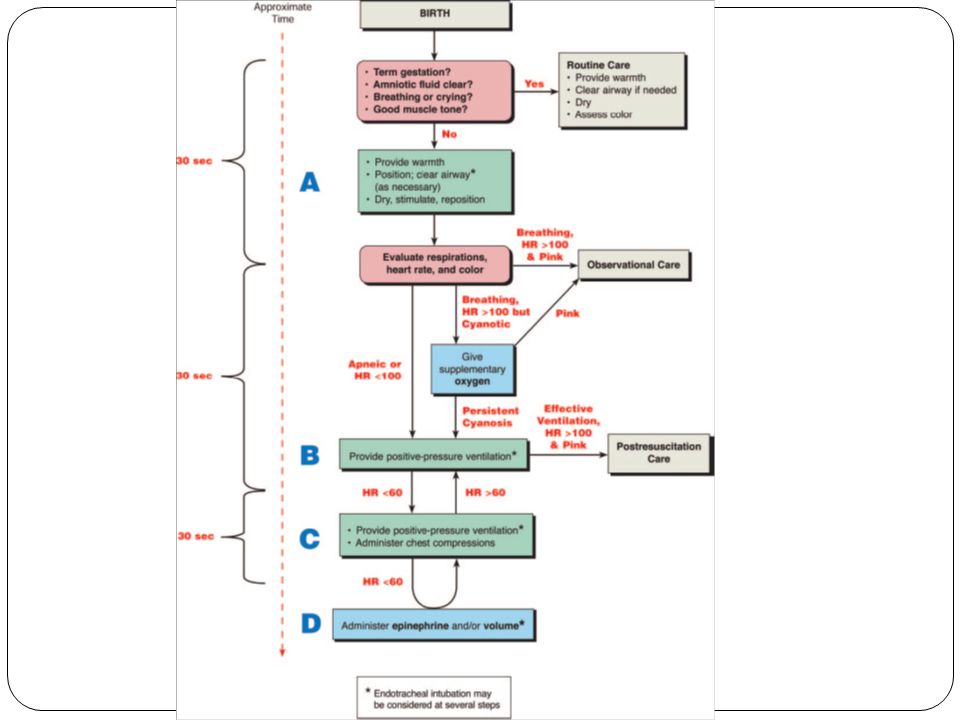
การประเมิน อายุครรภ์ครบกำหนดหรือไม่ น้ำคร่ำใสหรือไม่ หายใจหรือร้องดังหรือไม่ ความตึงตัวของกล้ามเนื้อดีหรือไม่ ให้ความอบอุ่น จัดท่าศีรษะ เปิดทางเดินหายใจ ให้โล่ง* (เท่าที่จำเป็น) เช็ดตัวให้แห้ง กระตุ้นให้หายใจ และจัดท่าศีรษะใหม่ ไม่ใช่ แรกเกิด ให้ความอบอุ่น จัดท่าศีรษะ ทำให้ ทางเดินหายใจโล่ง และดูดเสมหะตาม ความจำเป็น เช็ดตัวและให้การ กระตุ้นโดยการสัมผัส เพื่อให้ทารกหายใจ These are the initial steps you take to establish an airway and begin resuscitating a newborn. An asterisk (*) indicates intubation may be considered or required (eg, in a depressed newborn with meconium). * พิจารณาใส่ท่อหายใจ (ในกรณีที่ทารก ไม่หายใจ และมีขี้เทาปนเปื้อนในน้ำคร่ำ)
 เช็ดตัวให้แห้ง กระตุ้นให้หายใจ. และจัดท่าศีรษะใหม่ ไม่ใช่ แรกเกิด. ให้ความอบอุ่น. จัดท่าศีรษะ ทำให้ ทางเดินหายใจโล่ง และดูดเสมหะตาม ความจำเป็น เช็ดตัวและให้การ กระตุ้นโดยการสัมผัส เพื่อให้ทารกหายใจ. These are the initial steps you take to establish an airway and begin resuscitating a newborn. An asterisk (*) indicates intubation may be considered or required (eg, in a depressed newborn with meconium). * พิจารณาใส่ท่อหายใจ (ในกรณีที่ทารก. ไม่หายใจ และมีขี้เทาปนเปื้อนในน้ำคร่ำ)")
10
การให้ความอบอุ่นแก่ทารก
ป้องกันการสูญเสียความร้อนโดย วางทารกไว้ใต้เครื่องให้ความอบอุ่น (radiant warmer) เช็ดตัวให้แห้ง เอาผ้าเปียกออก Prevention of heat loss is critical during resuscitation. Place the newborn in a preheated overhead radiant warmer. It is important to preheat the radiant warmer so that the newborn is placed on a warm mattress. Instructor Tip: Do not pre-warm blankets or towels by placing them on top of the warmer, because of the risk of fire. Put the newborn’s head at the foot of the warmer for easy access to the airway. Quickly dry the newborn with a warm towel to remove amniotic fluid and prevent evaporative heat loss. This act of drying also provides gentle stimulation, which may initiate or help maintain breathing. The exception is when meconium is present in the trachea. Then it is preferable to delay stimulation that may be caused by drying until the meconium has been suctioned from the trachea. It is imperative to remember to remove wet towels. Don’t block the radiant heat with towels, blankets, or team members’ heads or upper bodies. Very preterm newborns may require placement, below the neck, in a food-grade plastic reclosable bag without drying to prevent heat loss. (See Lesson 8.) A pre-warmed overhead radiant warmer minimizes radiant heat loss and allows access to, and visualization of, the newborn.
 เช็ดตัวให้แห้ง. เอาผ้าเปียกออก. Prevention of heat loss is critical during resuscitation. Place the newborn in a preheated overhead radiant warmer. It is important to preheat the radiant warmer so that the newborn is placed on a warm mattress. Instructor Tip: Do not pre-warm blankets or towels by placing them on top of the warmer, because of the risk of fire. Put the newborn’s head at the foot of the warmer for easy access to the airway. Quickly dry the newborn with a warm towel to remove amniotic fluid and prevent evaporative heat loss. This act of drying also provides gentle stimulation, which may initiate or help maintain breathing. The exception is when meconium is present in the trachea. Then it is preferable to delay stimulation that may be caused by drying until the meconium has been suctioned from the trachea. It is imperative to remember to remove wet towels. Don’t block the radiant heat with towels, blankets, or team members’ heads or upper bodies. Very preterm newborns may require placement, below the neck, in a food-grade plastic reclosable bag without drying to prevent heat loss. (See Lesson 8.) A pre-warmed overhead radiant warmer minimizes radiant heat loss and allows access to, and visualization of, the newborn.")
11
วิธีการทำให้ทางเดินหายใจโล่ง
การเปิดทางเดินหายใจ ทำได้โดยการจัดศีรษะของ ทารกให้อยู่ในท่า “sniffing” ทารกควรนอนหงายหรือตะแคง โดยให้คอแหงน เล็กน้อย ท่า “sniffing” ทำให้ช่องคอ กล่องเสียงและหลอดลม อยู่ในแนวเส้นตรง และลมผ่านเข้าได้สะดวก Once the newborn has been placed under a preheated radiant warmer and dried, the next step is to ensure “A” of the ABCs—establishment of an open airway. Correct positioning of the newborn will bring the posterior pharynx, larynx, and trachea in line, which will facilitate unrestricted air entry. Instructor Tip: Although positioning before suctioning is suggested, if meconium is not present, you may position the newborn before or after suctioning. The important point is that opening the airway consists of both suctioning and positioning.

12
การเปิดทางเดินหายใจ ทางเดินหายใจ เปิดโล่ง ทางเดินหายใจอุดตันจากการงอคอ
มากเกินไป ทางเดินหายใจอุดตันจากการแหงนคอมากเกินไป The newborn should be placed on his or her back, with the neck slightly extended. Care should be taken to prevent hyperextension or flexion of the neck, since either may decrease air entry. To help maintain correct position, you may place a rolled blanket or towel under the shoulders, elevating them three fourths of an inch to 1 inch off the mattress. This roll may be particularly useful if the newborn has a large occiput. Correct positioning allows an open airway to be maintained. In addition, the newborn will be in the optimal position if assisted ventilation becomes necessary.

13
อัตราการเต้นของหัวใจ
การประเมิน ภายหลังการดูแลช่วยเหลือเบื้องต้น การช่วยเหลือขั้นต่อไป ขึ้นกับผลการประเมินดังต่อไปนี้ ประเมินการหายใจ อัตราการเต้นของหัวใจ และสีผิว การหายใจ อัตราการเต้นของหัวใจ สีผิว After initial steps, evaluate the newborn often, about every 30 seconds. If the newborn is not breathing (has apnea) or has a heart rate less than 100 beats per minute (bpm), proceed to Block B. Instructor Tip: Respirations and color are naturally assessed during the initial steps because you are handling the baby and assessing progress through the first moments of transition. ท่านมีเวลาประมาณ 30 วินาที ในการช่วยเหลือแต่ละขั้นตอน ก่อนการประเมินเพื่อตัดสินใจให้การช่วยเหลือขั้นต่อไป
 or has a heart rate less than 100 beats per minute (bpm), proceed to Block B. Instructor Tip: Respirations and color are naturally assessed during the initial steps because you are handling the baby and assessing progress through the first moments of transition. ท่านมีเวลาประมาณ 30 วินาที ในการช่วยเหลือแต่ละขั้นตอน ก่อนการประเมินเพื่อตัดสินใจให้การช่วยเหลือขั้นต่อไป.")
14
การดูแลทารกที่มีขี้เทาในน้ำคร่ำ
ขี้เทาปนในน้ำคร่ำ ไม่ ใช่ ทารก “vigorous”* ใช่ ไม่ ดูดเสมหะในปากและหลอดลมคอ After delivery, the appropriate method for clearing the airway further will depend on The presence of meconium The baby’s level of activity Studies have shown that direct suctioning of the trachea should be performed only if a meconium-stained newborn has depressed respirations, depressed muscle tone, and/or a heart rate less than 100 beats per minute. Instructor Tip: No clinical studies warrant basing tracheal suctioning guidelines on meconium consistency. ให้การช่วยกู้ชีพเบื้องต้น ดูดเสมหะในปากและจมูก เช็ดตัวให้แห้ง, กระตุ้น, จัดท่าศีรษะใหม่

15
ขั้นตอนเบื้องต้น: มีขี้เทาในน้ำคร่ำ
ทารก Not vigorous: ดูดขี้เทาในหลอดลมคอทันที หลังคลอด ก่อนให้การช่วยเหลือขั้นต่อไป ทารก Vigorous: ดูดขี้เทาและสารคัดหลั่งจากปากและจมูก และช่วยเหลือตามขั้นตอน “Vigorous” is defined as a newborn who has strong respiratory efforts, good muscle tone, and a heart rate greater than 100 beats per minute. If meconium is present and the newborn is not vigorous, suction the baby’s trachea before proceeding with any other steps. If the baby is vigorous, suction the mouth and nose only, and proceed with resuscitation as required. Vigorous คือ การหายใจได้ดี ความตึงตัวของกล้ามเนื้อดี อัตราการเต้นของหัวใจ >100 ครั้ง/นาที

16
ทารกแรกเกิดที่มีขี้เทาในน้ำคร่ำและทารกไม่ค่อยร้อง Not vigorous
ทำการดูดขี้เทาจากหลอดลมคอทันที ใส่ laryngoscope และใช้สายดูดเสมหะเบอร์ 12F หรือ 14F เพื่อจะดูดเสมหะในปาก ช่องคอด้านหลัง ใช้ท่อช่วยหายใจเป็นตัวดูดเสมหะ โดยต่อท่อช่วยหายใจกับ meconium aspirator และเครื่องดูดเสมหะ แล้วถอยท่อออกช้าๆ การดูดขี้เทา ใช้เวลาไม่เกิน 3-5 วินาที กรณีที่ดูดไม่ได้ขี้เทา ให้เริ่มปฏิบัติการช่วยกู้ชีพต่อทันที กรณีที่ทำการดูดครั้งแรกได้ขี้เทา ให้ฟังการเต้นของหัวใจทารก หากหัวใจเต้นเร็ว ให้ทำการใส่ท่อช่วยหายใจทำการดูดซ้ำ หากหัวใจทารกเต้นช้า ควรช่วยหายใจด้วยแรงดันบวก If the newborn has depressed respirations, depressed muscle tone, and/or a heart rate less than 100 beats per minute, direct suctioning of the trachea soon after delivery is indicated before many spontaneous respirations or assisted ventilation has occurred. The procedure for suctioning should be repeated as necessary until little additional meconium is recovered, or until the newborn’s heart rate indicates that resuscitation must proceed without delay.

17
อัตราการเต้นของหัวใจ
การช่วยหายใจ (B) B ให้ออกซิเจน ยังคงเขียวตลอด ให้การช่วยหายใจ ด้วยแรงดันบวก * หยุดหายใจหรือ อัตราการเต้นของ หัวใจ 100 หายใจได้เองและ หัวใจ 100 แต่ยังคงเขียว ประเมินการหายใจ อัตราการเต้นของหัวใจ และสีผิว ถ้าทารกหยุดหายใจ หรืออัตรา การเต้นของหัวใจ 100 ครั้งต่อ นาที : ช่วยหายใจด้วยแรงดันบวก * ถ้าทารกหายใจได้เอง และอัตราการเต้นของหัวใจ 100 ครั้งต่อนาที แต่เขียว ให้ออกซิเจน ถ้าอาการเขียวไม่ดีขึ้น ช่วย หายใจด้วยแรงดันบวก If the newborn is not breathing adequately (has apnea or is gasping), has a heart rate of <100 beats per minute (bpm), or appears blue (cyanotic), you proceed to block B. If the baby is apneic or has a heart rate of <100 bpm, give positive-pressure ventilation. If the baby is breathing and has a heart rate of >100 bpm but has central cyanosis, you should give supplemental oxygen. If central cyanosis persists after giving oxygen, you should then proceed to positive-pressure ventilation. * พิจารณาใส่ท่อหายใจ
 B. ให้ออกซิเจน. ยังคงเขียวตลอด. ให้การช่วยหายใจ. ด้วยแรงดันบวก * หยุดหายใจหรือ. อัตราการเต้นของ. หัวใจ 100. หายใจได้เองและ. หัวใจ 100. แต่ยังคงเขียว. ประเมินการหายใจ. อัตราการเต้นของหัวใจ. และสีผิว. ถ้าทารกหยุดหายใจ หรืออัตรา การเต้นของหัวใจ 100 ครั้งต่อ นาที : ช่วยหายใจด้วยแรงดันบวก * ถ้าทารกหายใจได้เอง และอัตราการเต้นของหัวใจ 100 ครั้งต่อนาที แต่เขียว. ให้ออกซิเจน. ถ้าอาการเขียวไม่ดีขึ้น ช่วย หายใจด้วยแรงดันบวก. If the newborn is not breathing adequately (has apnea or is gasping), has a heart rate of <100 beats per minute (bpm), or appears blue (cyanotic), you proceed to block B. If the baby is apneic or has a heart rate of <100 bpm, give positive-pressure ventilation. If the baby is breathing and has a heart rate of >100 bpm but has central cyanosis, you should give supplemental oxygen. If central cyanosis persists after giving oxygen, you should then proceed to positive-pressure ventilation. * พิจารณาใส่ท่อหายใจ.")
18
การให้ออกซิเจนผ่านตามสาย (Free-flow Oxygen)
ไม่สามารถให้ออกซิเจน free-flow ผ่าน self-inflating bag ที่ต่อกับหน้ากากได้ Deprivation of oxygen to vital tissues is one of the primary reasons for the clinical consequences associated with perinatal compromise. Free-flow oxygen refers to blowing oxygen over the newborn’s nose so that the newborn breathes oxygen-enriched air. For a brief time, free-flow oxygen can be given using one of the following methods: Flow-inflating bag and mask Oxygen tubing Free-flow oxygen CANNOT be given reliably by a mask attached to a self-inflating bag. Wall or portable oxygen sources send 100% oxygen through the tubing. As oxygen flows out of the tubing or mask, it mixes with room air, which contains only 21% oxygen. The concentration of oxygen that reaches the newborn’s nose is determined by the amount of 100% oxygen coming from the tube or mask (usually at least 5 L/min) and the amount of room air it must pass through to reach the newborn. Therefore, it is important to have the oxygen mask or tube very close to the newborn’s nose to provide the highest possible concentration of oxygen. Oxygen mask
 and the amount of room air it must pass through to reach the newborn. Therefore, it is important to have the oxygen mask or tube very close to the newborn’s nose to provide the highest possible concentration of oxygen. Oxygen mask.")
19
ข้อบ่งชี้ในการช่วยหายใจด้วยแรงดันบวก
หยุดหายใจหรือหายใจเฮือก อัตราการเต้นของหัวใจน้อยกว่า 100 ครั้ง/นาที ตัวเขียวขณะได้ก๊าซออกซิเจนเข้มข้น 100% If, after the initial steps, the baby is not breathing or is gasping, the heart rate is less than 100 bpm, or the color remains cyanotic despite 100% free-flow oxygen, the next step is to provide positive-pressure ventilation. This is a critically important skill and the single most important step in the resuscitation of the compromised newborn. The success of resuscitation may be dependent on the effectiveness of this procedure. การช่วยหายใจอย่างมีประสิทธิภาพ เป็นปัจจัย หลักในการช่วยกู้ชีพทารกให้ประสบผลสำเร็จได้

20
อุปกรณ์ที่ใช้ในการช่วยหายใจ ด้วยแรงดันบวก
Self-inflating bag ข้อดี: พองตัวได้เอง มีลิ้นลดความดัน (pop-off valve) กรณีที่บีบความดันเกิน 40 ซม.น้ำ ข้อเสีย: พองตัวได้เอง แม้ไม่มีก๊าซเข้าสู่ bag หน้ากากต้องแนบสนิทกับหน้าของทารก จึงจะทำให้ลมจากการบีบ bag เข้าปอดได้ ต้องต่ออุปกรณ์เก็บกักออกซิเจน (oxygen reservoir) ไม่สามารถใช้ในการให้ก๊าซออกซิเจนอย่างเดียว ถ้าไม่บีบ bag เพราะมีลิ้นปิดกั้นอยู่ ไม่สามารถให้ CPAP และ PEEP ได้ ยกเว้นต่อ PEEP valve Flow-inflating bag There are 3 types of devices to give positive-pressure ventilation to newborns. The self-inflating bag inflates without a compressed gas source after it is squeezed. It remains inflated at all times. The flow-inflating bag is collapsed when not in use, and it looks like a deflated balloon. It inflates only when gas flows into the bag and the opening is sealed, as when the mask is placed tightly on a newborn’s face. The T-piece resuscitator works only when gas flows into it. The gas is directed to the environment or to the baby by occluding or releasing the opening on a T-shaped tube with your finger or thumb.
 กรณีที่บีบความดันเกิน 40 ซม.น้ำ. ข้อเสีย: พองตัวได้เอง แม้ไม่มีก๊าซเข้าสู่ bag. หน้ากากต้องแนบสนิทกับหน้าของทารก จึงจะทำให้ลมจากการบีบ bag เข้าปอดได้ ต้องต่ออุปกรณ์เก็บกักออกซิเจน (oxygen reservoir) ไม่สามารถใช้ในการให้ก๊าซออกซิเจนอย่างเดียว ถ้าไม่บีบ bag เพราะมีลิ้นปิดกั้นอยู่ ไม่สามารถให้ CPAP และ PEEP ได้ ยกเว้นต่อ PEEP valve. Flow-inflating bag. There are 3 types of devices to give positive-pressure ventilation to newborns. The self-inflating bag inflates without a compressed gas source after it is squeezed. It remains inflated at all times. The flow-inflating bag is collapsed when not in use, and it looks like a deflated balloon. It inflates only when gas flows into the bag and the opening is sealed, as when the mask is placed tightly on a newborn’s face. The T-piece resuscitator works only when gas flows into it. The gas is directed to the environment or to the baby by occluding or releasing the opening on a T-shaped tube with your finger or thumb.")
21
ลักษณะสำคัญของอุปกรณ์ช่วยหายใจด้วยแรงดันบวก
ขนาดของหน้ากากที่เหมาะสม ความสามารถในการให้ออกซิเจนความเข้มข้นต่างๆ กันจนถึงออกซิเจนเข้มข้น 90% to 100% ความสามารถในการควบคุมความดันช่วงหายใจเข้า (PIP) และระยะเวลาช่วงหายใจเข้า (inspiratory time) ขนาดของ bag ที่เหมาะสม ( มิลลิลิตร) มาตรการป้องกันไม่ให้ทารกได้รับแรงดันมากเกินไป A variety of mask sizes, appropriate for newborns of different weights, should be available at every delivery. Cushioned, anatomically shaped masks are preferred. Term newborns who require positive-pressure ventilation at birth should be initially ventilated with a high concentration of oxygen (90%-100%). Bags used for newborns should have a volume of 200 to 750 mL. Term newborns require only 15 to 25 mL with each ventilation (5-8 mL/kg). To minimize complications resulting from high ventilation pressures, resuscitation devices should have certain safety features to prevent unwanted high pressures.
 และระยะเวลาช่วงหายใจเข้า (inspiratory time) ขนาดของ bag ที่เหมาะสม ( มิลลิลิตร) มาตรการป้องกันไม่ให้ทารกได้รับแรงดันมากเกินไป. A variety of mask sizes, appropriate for newborns of different weights, should be available at every delivery. Cushioned, anatomically shaped masks are preferred. Term newborns who require positive-pressure ventilation at birth should be initially ventilated with a high concentration of oxygen (90%-100%). Bags used for newborns should have a volume of 200 to 750 mL. Term newborns require only 15 to 25 mL with each ventilation (5-8 mL/kg). To minimize complications resulting from high ventilation pressures, resuscitation devices should have certain safety features to prevent unwanted high pressures.")
22
Self-inflating Bag: การควบคุมออกซิเจน
ต้องต่ออุปกรณ์เก็บกักออกซิเจน (oxygen reservoir) จึงจะได้ความเข้มข้นของออกซิเจนสูง แม้ว่าจะใช้ออกซิเจน 100% ถ้าไม่มีอุปกรณ์เก็บกักออกซิเจน ทารกจะได้รับออกซิเจนประมาณ 40% ซึ่งอาจไม่เพียงพอในการช่วยกู้ชีพทารกแรกเกิด Newborns who require resuscitation with assisted ventilation at birth may require a high concentration of oxygen (90% to 100%). Air drawn into a self-inflating bag through the air inlet dilutes the concentration of oxygen in the bag. As a result, the concentration of oxygen actually received by the patient is greatly reduced to about 40%. Click on the image to play video
 จึงจะได้ความเข้มข้นของออกซิเจนสูง. แม้ว่าจะใช้ออกซิเจน 100% ถ้าไม่มีอุปกรณ์เก็บกักออกซิเจน ทารกจะได้รับออกซิเจนประมาณ 40% ซึ่งอาจไม่เพียงพอในการช่วยกู้ชีพทารกแรกเกิด. Newborns who require resuscitation with assisted ventilation at birth may require a high concentration of oxygen (90% to 100%). Air drawn into a self-inflating bag through the air inlet dilutes the concentration of oxygen in the bag. As a result, the concentration of oxygen actually received by the patient is greatly reduced to about 40%. Click on the image to play video.")
23
Self-inflating Bag: การควบคุมออกซิเจน
อุปกรณ์เก็บกักออกซิเจน ชนิดปลายเปิด อุปกรณ์เก็บกักออกซิเจน ชนิดปลายปิด High concentrations of oxygen can be achieved with a self-inflating bag by using an oxygen reservoir. The reservoir is an appliance that can be placed over the bag’s air inlet. อุปกรณ์เก็บกักออกซิเจน

24
Self-inflating Bag: แรงดัน
ปริมาณความดันที่ทารกได้รับในแต่ละครั้ง ขึ้นอยู่กับ 3 ปัจจัย ดังนี้ ความแรงในการบีบ bag มีรอยรั่วระหว่างหน้ากาก (mask) กับหน้าทารกหรือไม่ ระดับของความดันที่กำหนดไว้ที่ลิ้นลดความดัน The amount of pressure delivered by a self-inflating bag is not dependent on the flow of oxygen entering the bag. When you seal the mask on the newborn’s face (or connect the bag to an endotracheal tube), there will be no change in the inflation of the self-inflating bag.
 กับหน้าทารกหรือไม่ ระดับของความดันที่กำหนดไว้ที่ลิ้นลดความดัน. The amount of pressure delivered by a self-inflating bag is not dependent on the flow of oxygen entering the bag. When you seal the mask on the newborn’s face (or connect the bag to an endotracheal tube), there will be no change in the inflation of the self-inflating bag.")
25
ความเข้มข้นของออกซิเจนที่ควรใช้ระหว่างการช่วยกู้ชีพทารกแรกเกิด
Neonatal Resuscitation Program มีข้อแนะนำให้ใช้ ออกซิเจนเข้มข้น 100% ระหว่างการช่วยหายใจด้วย แรงดันบวก มีบางการศึกษาพบว่า การให้ก๊าซออกซิเจนเข้มข้น น้อยกว่า 100% ก็อาจจะสามารถกู้ชีพทารกได้สำเร็จ ถ้าเริ่มการช่วยกู้ชีพทารกแรกเกิด โดยใช้ออกซิเจน เข้มข้นน้อยกว่า 100% เป็นเวลา 90 วินาที ทารกไม่ดี ขึ้น ควรเพิ่มความเข้มข้นของออกซิเจน จนถึง 100% One hundred percent oxygen should be used when positive-pressure ventilation is required during resuscitation of term babies. Some studies suggest that resuscitation with 21% oxygen (air) is just as successful as resuscitation with 100% oxygen. Prolonged exposure to 100% oxygen following perinatal asphyxia may have deleterious effects. However, supplemental oxygen during resuscitation may result in more rapid restoration of tissue oxygen and perhaps less permanent tissue damage. Some clinicians will elect to start resuscitation using less than 100% oxygen. If one chooses to start resuscitation with room air, it is recommended that oxygen be used if there is no improvement within 90 seconds following birth.
 is just as successful as resuscitation with 100% oxygen. Prolonged exposure to 100% oxygen following perinatal asphyxia may have deleterious effects. However, supplemental oxygen during resuscitation may result in more rapid restoration of tissue oxygen and perhaps less permanent tissue damage. Some clinicians will elect to start resuscitation using less than 100% oxygen. If one chooses to start resuscitation with room air, it is recommended that oxygen be used if there is no improvement within 90 seconds following birth.")
26
การใส่ท่อช่วยหายใจ: ข้อบ่งชี้
กรณีที่มีขี้เทาปนในน้ำคร่ำ หากทารก not vigorous การช่วยหายใจด้วยแรงดันบวกไม่มีประสิทธิภาพ หรือ ต้องช่วยหายใจเป็นเวลาหลายนาที เมื่อต้องทำการกดหน้าอก เพื่อให้สัมพันธ์กับการช่วย หายใจ เมื่อต้องการให้ยา epinephrine ระหว่างรอการหา หลอดเลือดดำ Endotracheal intubation may be performed at various points during resuscitation as indicated by the asterisk (*) in the flow diagram.
 in the flow diagram.")
27
ET tube ท่อช่วยหายใจ: ขนาดที่เหมาะสม ความลึกของท่อช่วยหายใจ น้ำหนัก
(กิโลกรัม) ความลึก (ซม.จากริมฝีปาก) 1* 7 2 8 3 9 4 10 *ทารกที่น้ำหนักน้อยกว่า 750 กรัม อาจใส่ท่อช่วยหายใจลึก 6 ซม. ก็เพียงพอ GA (wk) น้ำหนักตัว ขนาด ET-tube < < 1000 gram 2.5 gram 3 gram 3.5 > > 3000 gram ET tube
 ความลึก. (ซม.จากริมฝีปาก) 1* *ทารกที่น้ำหนักน้อยกว่า 750 กรัม อาจใส่ท่อช่วยหายใจลึก 6 ซม. ก็เพียงพอ. GA (wk) น้ำหนักตัว. ขนาด ET-tube. < 28 < 1000 gram gram gram > 38 > 3000 gram ET tube.")
28
การใส่ท่อช่วยหายใจ: อุปกรณ์
อุปกรณ์ที่ใช้ในการช่วยหายใจ ต้องสะอาดปราศจากเชื้อโรค และ พร้อมใช้อยู่เสมอ เตรียมอุปกรณ์สำหรับ ช่วยหายใจด้วย แรงดันบวก และ หน้ากาก เปิดออกซิเจน เตรียม Stethoscope เตรียมเทปกาว สำหรับติดท่อช่วย หายใจกับหน้าของ ทารก Each delivery room, nursery, and emergency department should have a complete set of the following items kept together and readily available: Laryngoscope with an extra set of batteries and extra bulbs. Blades: No. 1 (term newborns), No. 0 (preterm newborns); straight rather than curved blades are preferred. Endotracheal tubes with inside diameters of 2.5, 3.0, 3.5, and 4.0 mm (not tapered). Stylet (optional). Suction setup with 10F or larger suction catheter, plus sizes 5F or 6F and 8F for suctioning the endotracheal tube. Carbon dioxide (CO2) monitor or detector (a new recommendation). Roll of tape, ½ or ¾ inch, or endotracheal tube securing device. Scissors. Oral airway. Meconium aspirator. Stethoscope (neonatal head preferred). Positive-pressure device, pressure gauge (optional for self-inflating bags), and oxygen tubing. Self-inflating bag must have oxygen reservoir.
, No. 0 (preterm newborns); straight rather than curved blades are preferred. Endotracheal tubes with inside diameters of 2.5, 3.0, 3.5, and 4.0 mm (not tapered). Stylet (optional). Suction setup with 10F or larger suction catheter, plus sizes 5F or 6F and 8F for suctioning the endotracheal tube. Carbon dioxide (CO2) monitor or detector (a new recommendation). Roll of tape, ½ or ¾ inch, or endotracheal tube securing device. Scissors. Oral airway. Meconium aspirator. Stethoscope (neonatal head preferred). Positive-pressure device, pressure gauge (optional for self-inflating bags), and oxygen tubing. Self-inflating bag must have oxygen reservoir.")
29
การเตรียม Laryngoscope:
อุปกรณ์ประกอบ ควรเลือกขนาด blade ให้เหมาะสม เบอร์ 0 สำหรับทารกเกิดก่อนกำหนด เบอร์ 1 สำหรับทารกเกิดครบกำหนด ตรวจสอบความสว่างของหลอดไฟ เปิดเครื่องดูดเสมหะที่ความดัน 100 มม.ปรอท ต่อกับสายดูดเสมหะขนาด 10F (หรือใหญ่กว่า) เพื่อทำการ ดูดเสมหะในปาก ใช้สายดูดเสมหะที่เล็กกว่า เพื่อดูดเสมหะในท่อช่วยหายใจ Select the appropriately sized blade and attach it to the laryngoscope handle. No. 0 blade for preterm newborns and No. 1 for term newborns. Check the light to determine that the batteries and bulb are working. Suction equipment should be available and ready for use. Adjust the suction source to 100 mm Hg by occluding the end of the suction tubing. Smaller suction catheters (see chart) should be available for suctioning the tube if necessary. Connect a 10F or larger suction catheter to suction secretions from the mouth. Endotracheal Tube Size Catheter Size F or 6F F or 8F F or 10F F
 เพื่อทำการ ดูดเสมหะในปาก. ใช้สายดูดเสมหะที่เล็กกว่า เพื่อดูดเสมหะในท่อช่วยหายใจ. Select the appropriately sized blade and attach it to the laryngoscope handle. No. 0 blade for preterm newborns and No. 1 for term newborns. Check the light to determine that the batteries and bulb are working. Suction equipment should be available and ready for use. Adjust the suction source to 100 mm Hg by occluding the end of the suction tubing. Smaller suction catheters (see chart) should be available for suctioning the tube if necessary. Connect a 10F or larger suction catheter to suction secretions from the mouth. Endotracheal Tube Size Catheter Size F or 6F F or 8F F or 10F F.")
30
การช่วยเหลือขณะใส่ท่อช่วยหายใจ
เตรียมอุปกรณ์ให้พร้อม จัดท่า และจับศีรษะทารกให้อยู่นิ่ง ให้ free-flow oxygen ดูดเสมหะในปาก ส่งท่อช่วยหายใจให้ผู้ที่ทำการใส่ท่อ กดบริเวณ cricoid (ถ้าผู้ใส่ท่อช่วยหายใจร้องขอ) During the intubation procedure, the assistant plays a very important role. The intubator should never have to look away from the baby’s oropharynx. The assistant needs to anticipate the intubator’s needs and follow directions of the intubator. Free-flow oxygen should be provided during the procedure. If suction is needed, the assistant should hand the suction catheter to the intubator and occlude the port at the intubator’s request. The endotracheal tube needs to be handled cleanly and handed to the intubator so that it does not have to be turned around prior to insertion.
 During the intubation procedure, the assistant plays a very important role. The intubator should never have to look away from the baby’s oropharynx. The assistant needs to anticipate the intubator’s needs and follow directions of the intubator. Free-flow oxygen should be provided during the procedure. If suction is needed, the assistant should hand the suction catheter to the intubator and occlude the port at the intubator’s request. The endotracheal tube needs to be handled cleanly and handed to the intubator so that it does not have to be turned around prior to insertion.")
31
การใส่ท่อช่วยหายใจ: การเตรียมทารกเพื่อไม่ให้ขาดออกซิเจน
ให้ออกซิเจนและช่วยหายใจด้วยแรงดันบวกก่อนทำ การใส่ท่อช่วยหายใจ (ยกเว้นในกรณีที่มีขี้เทาปนใน น้ำคร่ำ) ให้ออกซิเจน free flow ระหว่างการใส่ท่อช่วยหายใจ ระยะเวลาในการใส่ท่อช่วยหายใจ ไม่เกิน 20 วินาที You can’t continue most resuscitation actions during intubation. To minimize hypoxia, the following steps are helpful: Pre-oxygenate the baby with positive-pressure ventilation and 100% oxygen before intubation attempts. Hold 100% free-flow oxygen by the baby’s face while the intubation is ongoing. Limit attempts to no longer than 20 seconds. If unsuccessful, remove the laryngoscope and give positive-pressure ventilation with the mask and then try again.
 ให้ออกซิเจน free flow ระหว่างการใส่ท่อช่วยหายใจ. ระยะเวลาในการใส่ท่อช่วยหายใจ ไม่เกิน 20 วินาที You can’t continue most resuscitation actions during intubation. To minimize hypoxia, the following steps are helpful: Pre-oxygenate the baby with positive-pressure ventilation and 100% oxygen before intubation attempts. Hold 100% free-flow oxygen by the baby’s face while the intubation is ongoing. Limit attempts to no longer than 20 seconds. If unsuccessful, remove the laryngoscope and give positive-pressure ventilation with the mask and then try again.")
32
การช่วยเหลือขณะใส่ท่อช่วยหายใจ
ทำการช่วยหายใจด้วยแรงดันบวก ระหว่างการใส่ท่อช่วยหายใจแต่ละครั้ง ต่อท่อช่วยหายใจเข้ากับอุปกรณ์ช่วยหายใจด้วยแรงดันบวก ประเมินอัตราการเต้นของหัวใจ ฟังเสียงลมเข้าปอด และประเมินการเคลื่อนขึ้นของหน้าอก ใช้เทปกาวติดท่อช่วยหายใจกับหน้าของทารก The assistant monitors the heart rate by tapping it out on the bed or quietly stating the heart rate periodically. The length of time for the attempt should be timed and not go much beyond 20 seconds. The assistant should be quietly supportive during this stressful period. If an intubation attempt is not successful, the assistant may help provide positive-pressure ventilation between attempts. (Ventilation is not possible if intubating to suction meconium.) CO2 detection is not appropriate when intubating for the purpose of suctioning meconium from the trachea. However, when intubating to ventilate the newborn, increasing heart rate and CO2 detection are the primary methods for confirming endotracheal tube placement. A rapid increase in heart rate is indicative of effective positive-pressure ventilation. If the heart rate does not rise after intubation, use the CO2 detector as the next indicator for confirming proper placement of the endotracheal tube. If the heart rate does not rise, and CO2 is not detected after several breaths, consider removing the tube, resuming bag-and-mask ventilation, and repeating the intubation process. Instructor Tip: Accidental extubation is more likely if one person holds the tube and another ventilates. The same person should hold the tube and ventilate. The assistant is then free to auscultate and secure the tube.
 CO2 detection is not appropriate when intubating for the purpose of suctioning meconium from the trachea. However, when intubating to ventilate the newborn, increasing heart rate and CO2 detection are the primary methods for confirming endotracheal tube placement. A rapid increase in heart rate is indicative of effective positive-pressure ventilation. If the heart rate does not rise after intubation, use the CO2 detector as the next indicator for confirming proper placement of the endotracheal tube. If the heart rate does not rise, and CO2 is not detected after several breaths, consider removing the tube, resuming bag-and-mask ventilation, and repeating the intubation process. Instructor Tip: Accidental extubation is more likely if one person holds the tube and another ventilates. The same person should hold the tube and ventilate. The assistant is then free to auscultate and secure the tube.")
33
การใส่ท่อช่วยหายใจ: ลักษณะทางกายภาพ
The anatomic landmarks that relate to intubation are labeled on the slides. Epiglottis: a lidlike structure overhanging the entrance to the trachea Vallecula: a pouch formed by the base of the tongue and the epiglottis Esophagus: the food passageway extending from the throat to the stomach 4. Glottis: the opening of the larynx leading to the trachea, flanked by the vocal chords 5. Vocal cords: mucous membrane-covered ligaments on both sides of the glottis

34
การใส่ท่อช่วยหายใจ: การจัดท่าของทารก
คอแหงน มากเกินไป คองอ ท่าที่ ถูก ต้อง The correct position of the newborn for intubation is the same as for mask ventilation. Place the newborn on a flat surface with the head in the midline position and the neck slightly extended. It may be helpful to place a roll under the newborn’s shoulders to maintain slight extension of the neck. This “sniffing” position aligns the trachea for optimal viewing by allowing a straight line of sight into the glottis once the laryngoscope has been properly placed. It is important not to hyperextend the neck, because this will raise the glottis above the line of sight and narrow the trachea. If there is too much flexion of the head toward the chest, you may not be able to directly visualize the glottis.

35
การตรวจสอบตำแหน่งของท่อช่วยหายใจ
สิ่งที่บ่งชี้ว่า ท่อช่วยหายใจอยู่ถูกตำแหน่ง ทารกมีสัญญาณชีพ (การเต้นของหัวใจ สีผิว การเคลื่อนไหว) ดีขึ้น ฟังปอดได้ยินเสียงลมเข้าเท่ากันทั้งสองข้าง ไม่ได้ยินเสียงลม ในกระเพาะอาหาร ขณะช่วยหายใจ เห็นการเคลื่อนขึ้นของทรวงอก เมื่อช่วยหายใจ ท้องของทารกไม่อืดขึ้น เห็นไอน้ำในท่อช่วยหายใจ ในขณะหายใจออก เอ็กซเรย์ดูตำแหน่งท่อช่วยหายใจ ใช้ laryngoscope ส่องดู และเห็นว่าท่อช่วยหายใจอยู่ ระหว่าง vocal cords An increasing heart rate and CO2 detection are the primary methods for confirming endotracheal tube placement. When listening to breath sounds, be sure to use a small stethoscope and place it laterally and high in the chest wall (in the axilla). Be cautious when interpreting breath sounds in newborns because they are easily transmitted. Sounds heard over the anterior portion of the lungs may be coming from the stomach or esophagus, and breath sounds can be transmitted to the abdomen. Detection of CO2 in the endotracheal tube can serve as confirmatory evidence that the tube is in the trachea rather than in the esophagus. Two basic types of CO2 detectors are available. Colorimetric devices connected to the endotracheal tube change color in the presence of CO2. This device is the most commonly used method. Capnographs rely on the placement of a detector device placed at the end of the endotracheal tube connector or a port through which exhaled air is aspirated. The capnograph will display a specific CO2 level and should read more than 2% to 3% CO2 if the tube is in the trachea. Instructor Tip: Colorimetric devices connected to the endotracheal tube change color in the presence of CO2. This color change should persist after 6 breaths, as CO2 may have been blown into the stomach during positive-pressure ventilation, causing an initial color change that does not persist. Remember: Yellow = Y for “Yes, we’re intubated.” Purple = P for “Problem, we’re not detecting CO2.”
 ดีขึ้น. ฟังปอดได้ยินเสียงลมเข้าเท่ากันทั้งสองข้าง ไม่ได้ยินเสียงลม ในกระเพาะอาหาร. ขณะช่วยหายใจ เห็นการเคลื่อนขึ้นของทรวงอก. เมื่อช่วยหายใจ ท้องของทารกไม่อืดขึ้น. เห็นไอน้ำในท่อช่วยหายใจ ในขณะหายใจออก. เอ็กซเรย์ดูตำแหน่งท่อช่วยหายใจ. ใช้ laryngoscope ส่องดู และเห็นว่าท่อช่วยหายใจอยู่ ระหว่าง vocal cords. An increasing heart rate and CO2 detection are the primary methods for confirming endotracheal tube placement. When listening to breath sounds, be sure to use a small stethoscope and place it laterally and high in the chest wall (in the axilla). Be cautious when interpreting breath sounds in newborns because they are easily transmitted. Sounds heard over the anterior portion of the lungs may be coming from the stomach or esophagus, and breath sounds can be transmitted to the abdomen. Detection of CO2 in the endotracheal tube can serve as confirmatory evidence that the tube is in the trachea rather than in the esophagus. Two basic types of CO2 detectors are available. Colorimetric devices connected to the endotracheal tube change color in the presence of CO2. This device is the most commonly used method. Capnographs rely on the placement of a detector device placed at the end of the endotracheal tube connector or a port through which exhaled air is aspirated. The capnograph will display a specific CO2 level and should read more than 2% to 3% CO2 if the tube is in the trachea. Instructor Tip: Colorimetric devices connected to the endotracheal tube change color in the presence of CO2. This color change should persist after 6 breaths, as CO2 may have been blown into the stomach during positive-pressure ventilation, causing an initial color change that does not persist. Remember: Yellow = Y for Yes, we’re intubated. Purple = P for Problem, we’re not detecting CO2.")
36
การตรวจสอบตำแหน่งของท่อช่วยหายใจ
ท่อช่วยหายใจ ไม่อยู่ในหลอดลมคอ ถ้า ทารกยังเขียว และหัวใจเต้นช้า ฟังไม่ได้ยินเสียงลมหายใจที่ปอดทั้งสองข้าง ท้องอืดขึ้น ได้ยินเสียงลมบริเวณกระเพาะอาหาร ไม่มีไอน้ำในท่อช่วยหายใจ ทรวงอกของทารกไม่เคลื่อนขึ้นเมื่อทำการช่วยหายใจด้วย แรงดันบวก It is very important to be certain that the tube is in the trachea. A misplaced tube is worse than having no tube at all. If the patient does not appear to be improving and the tube is possibly not in the trachea, use your right hand to hold the tube in place while you use your left hand to reinsert the laryngoscope so that you can visualize the glottis to see if the tube is passing between the vocal cords; and/or remove the tube, use positive-pressure ventilation until the heart rate is stabilized, and repeat the intubation procedure. Instructor Tip: The endotracheal tube is not in the trachea if the baby has an audible cry or regurgitates through the tube.

37
การไหลเวียนโลหิต (C) ถ้าอัตราการเต้นของหัวใจ 60 ครั้งต่อนาที
ภายหลังการช่วยหายใจด้วยแรงดันบวกนาน 30 วินาที กดหน้าอก ร่วมกับ ช่วยหายใจต่อไป ประเมินอีกครั้ง ถ้าอัตราการเต้นของหัวใจยัง 60 ครั้งต่อนาที ให้การ ช่วยเหลือขั้นต่อไป (D) If, after 30 seconds of adequate positive-pressure ventilation, the heart rate is less than 60 bpm, chest compressions and epinephrine may be needed for sufficient cardiac output so that blood can reach the lungs to pick up oxygen. Support circulation by starting chest compressions while continuing ventilation. After 30 seconds of chest compressions, evaluate the newborn again. If the heart rate is still less than 60 beats per minute, proceed to Block D. ช่วยหายใจด้วยแรงดันบวก (positive pressure ventilation) * กดหน้าอก (chest compression) * C * พิจารณาใส่ท่อหายใจ
 If, after 30 seconds of adequate positive-pressure ventilation, the heart rate is less than 60 bpm, chest compressions and epinephrine may be needed for sufficient cardiac output so that blood can reach the lungs to pick up oxygen. Support circulation by starting chest compressions while continuing ventilation. After 30 seconds of chest compressions, evaluate the newborn again. If the heart rate is still less than 60 beats per minute, proceed to Block D. ช่วยหายใจด้วยแรงดันบวก (positive pressure ventilation) * กดหน้าอก (chest compression) * C. * พิจารณาใส่ท่อหายใจ.")
38
การกดหน้าอก Chest Compressions
ช่วยเพิ่มการไหลเวียนเลือดชั่วคราว ต้องทำร่วมกับการช่วยหายใจ ควรใช้ออกซิเจน 100% When a newborn becomes hypoxic, the heart rate slows and myocardial contractility decreases. As a result, there is a diminished flow of blood and oxygen to the vital organs. The decreased supply of oxygen to these tissues can lead to irreparable damage to the brain, heart, kidneys, and bowel. Chest compressions are used to temporarily increase circulation and oxygen delivery. Chest compressions should always be accompanied by ventilation with 100% oxygen. Ventilation must be performed to ensure that the blood being circulated during chest compressions is oxygenated.

39
การกดหน้าอก: ข้อบ่งชี้
ช่วยหายใจ ด้วยแรงดันบวก * ช่วยหายใจด้วยแรงดันบวก * กดหน้าอก อัตราการเต้นของหัวใจ < 60 > 60 * พิจารณาใส่ท่อช่วยหายใจ ให้ออกซิเจน ยังคงเขียว หยุดหายใจ < 100 หายใจเอง > 100 แต่เขียว เมื่ออัตราการเต้น ของหัวใจน้อยกว่า 60 ครั้ง/นาที ทั้งๆ ที่ทารกได้รับการ ช่วยหายใจด้วยแรง ดันบวกอย่างเพียง พอแล้วเป็นเวลา 30 วินาที When chest compressions are indicated, the newborn probably has very low blood oxygen levels and significant acidosis. The myocardium is depressed and unable to contract strongly enough to pump blood to the lungs. Chest compressions will mechanically pump blood through the heart while ventilation continues. Instructor Tip: Even experienced resuscitators are concerned at the point when a baby requires chest compressions. Talk to each other and calmly plan your next steps. Concentrate on the tasks at hand and anticipate the need for additional help to record events, insert an orogastric tube if not already done, prepare for intubation if not already done, prepare for administration of epinephrine, and prepare for establishment of an umbilical venous line.

40
การกดหน้าอก: ต้องมีบุคลากร 2 คน
การกดหน้าอก: ต้องมีบุคลากร 2 คน คนหนึ่งกดหน้าอก อีกคนให้การช่วยหายใจ การกดหน้าอก: หัวใจไปชนกับกระดูก ไขสันหลัง ความดันในช่องอก เพิ่มขึ้น เกิดการไหลเวียนเลือด ไปยังอวัยวะสำคัญ Two people are required to administer chest compressions—one to compress the chest and one to continue ventilation. These 2 people need to coordinate their activities. The person administering chest compressions must have access to the chest and be able to position his or her hands correctly. The person assisting ventilation will need to be positioned at the newborn’s head to achieve an effective face-mask seal (or to stabilize the endotracheal tube), ventilate appropriately, and watch for effective chest movement.
, ventilate appropriately, and watch for effective chest movement.")
41
การกดหน้าอก: ตำแหน่งการวางมือและนิ้ว
การกดหน้าอก: ตำแหน่งการวางมือและนิ้ว ใช้นิ้วลากมาตามขอบ ล่างของกระดูกซี่โครง จนกระทั่งมาพบกระดูก xyphoid วางนิ้วหัวแม่มือหรือนิ้ว มือสองนิ้วเหนือต่อจาก กระดูก xyphoid ตาม แนวเส้นที่ลากระหว่าง หัวนม Run your fingers along the lower edge of the rib cage until you locate the xyphoid. Place your thumbs or fingers on the sternum, immediately above the xyphoid. Pressure is applied to the lower third of the sternum. Care must be used to avoid applying pressure to the xyphoid, which is a small projection where the lower ribs meet at the midline.

42
การกดหน้าอก: เทคนิคหัวแม่มือ (Thumb Technique)
นิ้วหัวแม่มืออยู่บน กระดูกหน้าอก นิ้วอื่นอยู่ใต้หลังทารก เพื่อหนุนกระดูกสันหลัง ใช้นิ้วหัวแม่มือกดลงบน กระดูกกลางอก (sternum) และปล่อย เพื่อให้หน้าอกคืนรูปได้ เต็มที่ ถูกต้อง ไม่ถูกต้อง The thumb technique is accomplished by encircling the torso with both hands and placing the thumbs on the sternum and the fingers under the baby’s back, supporting the spine. The thumbs can be placed side by side or, on a small baby, one over the other. เมื่อยล้าน้อยกว่า สามารถควบคุมความลึกของการกดหน้าอกได้ดีกว่า
 และปล่อย เพื่อให้หน้าอกคืนรูปได้ เต็มที่ ถูกต้อง. ไม่ถูกต้อง. The thumb technique is accomplished by encircling the torso with both hands and placing the thumbs on the sternum and the fingers under the baby’s back, supporting the spine. The thumbs can be placed side by side or, on a small baby, one over the other. เมื่อยล้าน้อยกว่า. สามารถควบคุมความลึกของการกดหน้าอกได้ดีกว่า.")
43
การกดหน้าอก: เทคนิคการใช้สองนิ้วมือ (2-Finger Technique)
ปลายของนิ้วกลางและ นิ้วชี้หรือนิ้วนางใช้ใน การกดหน้าอก มืออีกข้างให้วางหนุนที่ ด้านหลังของทารก Position the 2 fingers perpendicular to the chest, as shown, and press vertically with your fingertips. When compressing the chest, only the 2 fingertips should rest on the chest. This gives the best control of the pressure applied to the sternum. If you rest other portions of your hand on the chest, you can restrict chest expansion during ventilation and apply pressure to the vulnerable area of the chest, risking a pneumothorax or fractured ribs. เหมาะสำหรับผู้ช่วยกู้ชีพที่มีมือขนาดเล็ก ใช้พื้นที่ไม่มาก เปิดทางเข้าสู่สะดือได้ดีกว่าเมื่อต้องการให้ยา

44
การกดหน้าอก: ความแรงและความลึกในการกด
การกดหน้าอก: ความแรงและความลึกในการกด ความลึกของการกด หน้าอกประมาณ 1 ใน 3 ของความกว้างทรวงอกใน แนวหน้าหลัง ถูกต้อง ไม่ถูกต้อง การกดหน้าอก: เทคนิค ระยะเวลาที่ใช้ในการกด ควรจะสั้นกว่าระยะเวลา ในการปล่อย เพื่อให้ได้ ปริมาณเลือดที่ออกจาก หัวใจมากที่สุด Controlling the pressure used in compressing the sternum is an important part of the procedure. With your fingers and hands correctly positioned, you should use enough pressure to depress the sternum to a depth of approximately one third of the anterior-posterior diameter of the chest, then completely release the pressure to allow the heart to refill. One compression consists of the downward stroke plus the release. The actual distance compressed will depend on the size of the newborn. The duration of the downward stroke of the compression should be somewhat shorter than the duration of the release for generation of maximum cardiac output.

45
การกดหน้าอก : อันตรายที่อาจเกิดขึ้น
การกดหน้าอก : อันตรายที่อาจเกิดขึ้น ตับ หัวใจ ปอด การฉีกขาดของตับ กระดูกซี่โครงหัก กระดูก ซี่โครงหัก เลือดออก ลมรั่วใน ช่องอก As you perform chest compressions, you must apply enough pressure to compress the heart between the sternum and spine without damaging underlying organs. Potential complications can occur. The ribs are fragile and can be easily broken. Pressure over the lower tip of the sternum (xyphoid) can lead to laceration of the liver.
 can lead to laceration of the liver.")
46
การกดหน้าอกประสานงานกับการช่วยหายใจ
1 รอบ ประกอบด้วยการกด หน้าอก 3 ครั้ง และการ ช่วยหายใจ 1 ครั้ง ในเวลา 2 วินาที ทำการช่วยหายใจ 30 ครั้ง และกดหน้าอก 90 ครั้ง/ นาที รวมกันเป็น 120 ครั้ง ต่อนาที During chest compressions, the ventilation rate is actually 30 breaths per minute rather than the rate you previously learned for positive-pressure ventilation without compressions, which was 40 to 60 breaths per minute. This lower ventilatory rate is necessitated by the need to provide an adequate number of compressions, yet avoid simultaneous compressions and ventilation. To ensure that the process can be coordinated, it is important that you practice with another person and practice both roles.

47
การกดหน้าอก: การหยุดกดหน้าอก
หลังจากทำการกด หน้าอกและช่วย หายใจแล้ว 30 วินาที ควรหยุดกดหน้าอก เพื่อตรวจอัตราการ เต้นของหัวใจอีกครั้ง * พิจารณาใส่ท่อช่วยหายใจ หายใจอย่างมี ประสิทธิภาพ อัตราการเต้น ของหัวใจ >100 สีผิวเป็นสีชมพู ช่วยหายใจ ด้วยแรงดันบวก * ช่วยหายใจด้วยแรงดันบวก * กดหน้าอก ของหัวใจ< 60 ของหัวใจ > 60 ยังคงเขียว หยุดหายใจ ของหัวใจ < 100 หายใจเอง อัตราการเต้นของหัวใจ > 100 แต่เขียว ประเมินการหายใจ อัตราการเต้นของหัวใจและสีผิว ให้ยา epinephrine* ของหัวใจ < 60 การดูแลหลัง การช่วยกู้ชีพ ให้ออกซิเจน After approximately 30 seconds of well-coordinated compressions and ventilation, stop for 6 seconds to determine the heart rate again. To determine heart beats per minute, count the beats in 6 seconds and multiply by 10. Announce the actual heart rate (say “the heart rate is 70” not “I count 7 beats”). If the heart rate is >60 bpm, discontinue chest compressions but continue positive-pressure ventilation at the rate of 40 to 60 breaths per minute If the heart rate is >100 bpm and the newborn begins to breathe spontaneously, slowly withdraw positive-pressure ventilation and move the newborn to the nursery for post resuscitation care If the heart rate is <60 bpm, intubate the infant (if not already done), insert an umbilical venous catheter and give epinephrine Instructor Tip: Learn to assess the heart rate quickly. You should be able to recognize, within a few beats, if the heart rate is less than 60 bpm, 100 bpm, and more than 100 bpm.
. If the heart rate is >60 bpm, discontinue chest compressions but continue positive-pressure ventilation at the rate of 40 to 60 breaths per minute. If the heart rate is >100 bpm and the newborn begins to breathe spontaneously, slowly withdraw positive-pressure ventilation and move the newborn to the nursery for post resuscitation care. If the heart rate is <60 bpm, intubate the infant (if not already done), insert an umbilical venous catheter and give epinephrine. Instructor Tip: Learn to assess the heart rate quickly. You should be able to recognize, within a few beats, if the heart rate is less than 60 bpm, 100 bpm, and more than 100 bpm.")
48
การกดหน้าอก: อัตราการเต้นของหัวใจยังคงต่ำกว่า 60 ครั้ง/นาที
ตรวจสอบว่าการช่วยหายใจมีประสิทธิภาพหรือไม่ พิจารณาใส่ท่อช่วยหายใจ ถ้ายังไม่ได้ใส่ ใส่สายสวนหลอดเลือดของสะดือ เพื่อให้ยา epinephrine When you are administering chest compressions and coordinating ventilation, continue to ask yourself the following questions: Is chest movement adequate? Is supplemental oxygen being given? Is the depth of chest compression approximately one third of the anterior-posterior diameter of the chest? Are the chest compressions and ventilation being well-coordinated? If the heart rate remains less than 60 beats per minute, you should give epinephrine, as described in Lesson 6. By this point in resuscitation, you most likely will have intubated the trachea, giving a more reliable means of ventilating, and called for additional personnel to record events. Because epinephrine administration seems likely, establishment of an umbilical venous line should be in progress. Instructor Tip: A newborn who requires chest compressions is seriously ill and needs a skilled and coordinated team to administer interventions. This is why we practice these skills frequently, so that all team members feel confident and competent during a more extensive resuscitation.

49
การให้ยาและสารน้ำ (D)
ถ้าอัตราการเต้นของหัวใจ 60 ครั้งต่อนาที ภายหลังการช่วยหายใจและกดหน้าอกอย่างเต็มที่ ให้ยา epinephrine ร่วมกับช่วยหายใจ และกดหน้าอกต่อไป ช่วยหายใจด้วยแรงดันบวก * กดหน้าอก * 30 วินาที ให้ยา epinephrine อัตราการเต้น ของหัวใจ 60 ครั้งต่อนาที C D การประเมิน If the heart rate remains less than 60 beats per minute, the actions in Blocks C and D are continued and repeated. This is indicated by the curved arrow. * พิจารณาใส่ท่อหายใจ

50
ข้อบ่งชี้ในการให้ยา epinephrine
ช่วยหายใจด้วยแรงดันบวกอย่างมีประสิทธิภาพแล้ว 30 วินาที ตามด้วย ช่วยหายใจด้วยแรงดันบวกร่วมกับการกดหน้าอกอีก 30 วินาที รวม = 60 วินาที If the heart rate remains below 60 bpm despite effective ventilation and chest compressions, ensure that ventilation and compressions are being given optimally and that you are using 100% oxygen. Epinephrine is not indicated before adequate ventilation has been established and chest compressions have been initiated for 30 seconds because You will waste valuable time that should be focused on establishing effective ventilation and oxygenation. Epinephrine will increase the workload and oxygen consumption of the heart muscle, which, in the absence of available oxygen, may cause myocardial damage. ไม่ควรให้ยา epinephrine ก่อนช่วยหายใจด้วย แรงดันบวกอย่างมีประสิทธิภาพ

51
การให้ยาและสารน้ำทางหลอดเลือดดำของสะดือ
ใส่สายสวนในหลอดเลือดของสะดือ เป็นทางให้สารน้ำและยา ใช้สายสวนขนาด 3.5F หรือ 5F ใช้เทคนิคปลอดเชื้อ To place a catheter in the umbilical vein, Clean the cord with antiseptic. Place a loose tie of umbilical tape around the base of the cord. Pre-fill a 3.5F or 5F single end-hole catheter with normal saline. Connect catheter to stopcock and syringe. Close the stopcock to the catheter to prevent fluid loss and air entry. Using sterile technique, Cut the cord with the scalpel below the clamp about 1 to 2 cm from the skin line. The umbilical vein will be seen as a large, thin-walled structure, usually at the 11- to 12-o’clock position. Insert the catheter into the umbilical vein. The course of the vein will be up toward the heart, so this is the direction you should point the catheter. Instructor Tip: Keep all umbilical venous catheter insertion supplies together in one sealed bag or tray. To prevent injury, stop compressions and alert team members when scalpel is being used.

52
Epinephrine: ผลของยา และการให้ซ้ำ
เพิ่มอัตราการเต้นของหัวใจ และความแรงของการ บีบตัวของกล้ามเนื้อหัวใจ ทำให้เกิดหลอดเลือดส่วนปลายหดตัว ถ้าให้ยาครั้งแรกทางท่อช่วยหายใจ การให้ยาซ้ำ ควรให้ทางหลอดเลือดดำของสะดือ As positive-pressure ventilation and chest compressions are continued, the rate should increase to more than 60 beats per minute within 30 seconds after giving epinephrine. If this does not happen, you may repeat the dose every 3 to 5 minutes. If the first dose has been given per endotracheal tube, give repeat doses via umbilical vein, if possible. Instructor Tip: If first dose is given via the endotracheal tube, REMEMBER the dose given intravenously will be a DIFFERENT dose of a SMALLER volume. LABEL SYRINGES for ET or IV use and double-check dosage prior to administration.

53
การบริหารยา Epinephrine
ความเข้มข้นของยาที่แนะนำ = 1:10,000 วิธีบริหารยาที่แนะนำ = ทางหลอดเลือดดำ (ให้ทางท่อช่วยหายใจได้ในระหว่างรอการใส่สายสวนหลอดเลือดดำ) ขนาดของยาที่แนะนำ = มล./กก. ของยา epinephrine 1:10,000 (ให้ มล./กก. ถ้าให้ทางท่อช่วยหายใจ) อัตราการให้ยาที่แนะนำ = เร็วที่สุดเท่าที่ทำได้ Epinephrine should be given by the umbilical vein. The endotracheal route is often faster than placing an umbilical catheter, but is associated with unreliable absorption and may not be effective at the lower dose. If a dose of epinephrine is given via the endotracheal tube while umbilical venous access is being established, consider a higher dose (0.3 mL-1.0 mL/kg) by this route only. Do not give high doses of epinephrine intravenously.
 ขนาดของยาที่แนะนำ = มล./กก. ของยา epinephrine 1:10,000 (ให้ มล./กก. ถ้าให้ทางท่อช่วยหายใจ) อัตราการให้ยาที่แนะนำ = เร็วที่สุดเท่าที่ทำได้ Epinephrine should be given by the umbilical vein. The endotracheal route is often faster than placing an umbilical catheter, but is associated with unreliable absorption and may not be effective at the lower dose. If a dose of epinephrine is given via the endotracheal tube while umbilical venous access is being established, consider a higher dose (0.3 mL-1.0 mL/kg) by this route only. Do not give high doses of epinephrine intravenously.")
54
ถ้าทารกอาการไม่ดีขึ้นหลังให้ยา epinephrine (อัตราการเต้นของหัวใจ < 60 ครั้ง/นาที)
ตรวจสอบประสิทธิภาพของ การช่วยหายใจ การกดหน้าอก การใส่ท่อช่วยหายใจ ว่าอยู่ในหลอดลมคอหรือไม่ วิธีบริหารยา epinephrine พิจารณาว่า ทารกมีภาวะความดันเลือดต่ำจนช็อคหรือไม่ (hypovolemic shock) If the newborn is not responding to resuscitation, recheck the effectiveness of the interventions to this point. If the baby is pale and there is evidence of blood loss, consider the possibility of volume loss.
 If the newborn is not responding to resuscitation, recheck the effectiveness of the interventions to this point. If the baby is pale and there is evidence of blood loss, consider the possibility of volume loss.")
55
ทารกไม่ตอบสนองต่อการช่วยกู้ชีพ: ช็อค (hypovolemic shock)
ข้อบ่งชี้ในการให้สารน้ำทดแทน ทารกไม่ตอบสนองต่อการช่วยกู้ชีพ และ ทารกอยู่ในภาวะช็อค (สีผิวซีด ชีพจรเบา อัตราการเต้น ของหัวใจช้า หรืออาการไม่ดีขึ้นภายหลังการช่วยกู้ชีพ) มีประวัติทารกในครรภ์เสียเลือด ได้แก่ มารดามีเลือดออก ทางช่องคลอดจำนวนมาก รกลอกตัวก่อนกำหนด รกเกาะ ต่ำ และมีภาวะ twin-to-twin transfusion If there has been placental abruption, a placenta previa, or blood loss from the umbilical cord, the baby may be in hypovolemic shock. In some cases, the baby may have lost blood into the maternal circulation and there will be signs of shock with no obvious evidence of blood loss. Newborns in shock appear pale and have a weak pulse; they may have a persistently lower heart rate. Circulatory status often will not improve in response to effective ventilation, chest compressions, and administration of epinephrine. The baby may need re-expansion of his or her intravascular volume.
 มีประวัติทารกในครรภ์เสียเลือด ได้แก่ มารดามีเลือดออก ทางช่องคลอดจำนวนมาก รกลอกตัวก่อนกำหนด รกเกาะ ต่ำ และมีภาวะ twin-to-twin transfusion. If there has been placental abruption, a placenta previa, or blood loss from the umbilical cord, the baby may be in hypovolemic shock. In some cases, the baby may have lost blood into the maternal circulation and there will be signs of shock with no obvious evidence of blood loss. Newborns in shock appear pale and have a weak pulse; they may have a persistently lower heart rate. Circulatory status often will not improve in response to effective ventilation, chest compressions, and administration of epinephrine. The baby may need re-expansion of his or her intravascular volume.")
56
การให้สารน้ำทดแทน: ปริมาณและวิธีการให้
ชนิดของสารน้ำทดแทนที่แนะนำ = Normal saline สารน้ำทดแทนอื่นๆ = Ringer’s lactate หรือ เลือดกลุ่ม O Rh-negative ปริมาณของสารน้ำทดแทนที่แนะนำ = 10 มล./กก. วิธีการให้ที่แนะนำ= ทางหลอดเลือดดำของสะดือ วิธีการเตรียม = เตรียมสารน้ำปริมาณที่ต้องการใน กระบอกฉีดยาขนาดใหญ่ อัตราการให้สารน้ำที่แนะนำ = ให้ในเวลา 5-10 นาที The initial dose of solution is 10 mL/kg; however, if the newborn shows minimal improvement after the first dose, you may need to give another dose of 10 mL/kg. Volume expander must be given into the vascular system. The umbilical vein is usually the most accessible vein in a newborn, although the intraosseous route can be used. Some clinicians are concerned that rapid administration of volume to a newborn may result in intracranial hemorrhage. A steady infusion rate over 5 to 10 minutes is reasonable.

57
การตอบสนองต่อการให้สารน้ำทดแทน
อาการที่บ่งชี้ว่าทารกมีอาการดีขึ้น ภายหลังการ ให้สารน้ำทดแทน อัตราการเต้นของหัวใจเพิ่มขึ้น ชีพจรแรงขึ้น สีผิวซีด ลดลง ความดันโลหิตเพิ่มขึ้น ถ้าภาวะช็อค (hypovolemic shock) ไม่ดีขึ้น พิจารณาให้สารน้ำทดแทนอีกครั้ง (ปริมาณ 10 มล./กก.) The heart rate should increase, pulses should become stronger, color should improve, and blood pressure should increase. Volume expanders may be repeated if signs of hypovolemia persist. The same dose (10 mL/kg) should be given intravenously over 5 to 10 minutes.
 ไม่ดีขึ้น. พิจารณาให้สารน้ำทดแทนอีกครั้ง. (ปริมาณ 10 มล./กก.) The heart rate should increase, pulses should become stronger, color should improve, and blood pressure should increase. Volume expanders may be repeated if signs of hypovolemia persist. The same dose (10 mL/kg) should be given intravenously over 5 to 10 minutes.")
58
ภายหลังการให้ยา: ทารกอาการไม่ดีขึ้น
นึกถึงภาวะต่อไปนี้ ความผิดปกติของทางเดินหายใจ ปัญหาของปอด - ลมรั่วในช่องอก - ไส้เลื่อนกระบังลม โรคหัวใจพิการแต่กำเนิด ตรวจสอบประสิทธิภาพของ การช่วยหายใจ การกดหน้าอก การใส่ท่อช่วยหายใจ การให้ epinephrine พิจารณาว่าทารกมี ภาวะปริมาณสารน้ำในร่างกายต่ำ อัตราการเต้นของหัวใจ <60 หรือเขียวทั้งตัว หรือไม่สามารถช่วยหายใจได้ หัวใจหยุดเต้น พิจารณาหยุด การช่วยกู้ชีพ Approximately 30 seconds each should be required for a trial of the following 4 steps of resuscitation: Assessment and initial steps Positive-pressure ventilation Positive-pressure ventilation and chest compressions Positive-pressure ventilation, chest compressions, and epinephrine If you are certain that effective ventilation, chest compressions, and medications are being provided, consider mechanical causes of poor response, such as an airway malformation, pneumothorax, diaphragmatic hernia, or congenital heart disease. If the heart rate is absent or no progress is made in certain conditions, such as extreme prematurity, it may be appropriate to discontinue resuscitative efforts. Be confident that optimum technique has been administered for a minimum of 10 minutes before considering such a decision (Lesson 7). Instructor Tip: Stay calm and work as a team under these particularly stressful conditions.
. Instructor Tip: Stay calm and work as a team under these particularly stressful conditions.")
59
ทารกไม่ตอบสนองต่อการช่วยกู้ชีพ
อาจเห็นควรให้ยุติการช่วยชีวิต ถ้าไม่มีชีพจร หลังจากพยายามช่วยชีวิตอย่างเต็มที่นาน 10 นาที If there is no heart rate after 10 minutes of complete and adequate resuscitation efforts and there is no evidence of other causes of newborn compromise, discontinuation of resuscitation efforts may be appropriate. Current data indicate that, after 10 minutes of asystole, newborns are very unlikely to survive, or likely to survive with severe disability. However, more than 10 minutes after birth may have been required to assess the baby and optimize the resuscitation efforts. There is no obligation to continue life support if it is the judgment of experienced clinicians that such support would not be in the best interest of the baby or would serve no useful purpose (ie, would be futile). In the case of withdrawal of critical care interventions and institution of comfort care support after successful initial resuscitation, the parents should be in agreement with this judgment.
. In the case of withdrawal of critical care interventions and institution of comfort care support after successful initial resuscitation, the parents should be in agreement with this judgment.")
60
ให้ออกซิเจน* แรกเกิด อายุครรภ์ครบกำหนดหรือไม่ การดูแลทารกปกติ
ช่วยหายใจด้วยแรงดันบวก * กดหน้าอก * ให้ยา epinephrine อัตราการเต้น ของหัวใจ 60 ครั้งต่อนาที อายุครรภ์ครบกำหนดหรือไม่ น้ำคร่ำใสหรือไม่ หายใจหรือร้องดังหรือไม่ ความตึงตัวของกล้ามเนื้อดีหรือไม่ ให้ความอบอุ่น จัดท่าศีรษะ เปิดทางเดินหายใจ * ให้โล่ง* (เท่าที่จำเป็น) เช็ดตัวให้แห้ง กระตุ้นให้หายใจ และจัดท่าศีรษะใหม่ ไม่ใช่ แรกเกิด ให้ออกซิเจน* ยังคงเขียวตลอด ให้การช่วยหายใจ * ด้วยแรงดันบวก * หยุดหายใจหรือ อัตราการเต้นของ หัวใจ 100 หายใจได้เองและ หัวใจ 100 แต่ยังคงเขียว ประเมินการหายใจ อัตราการเต้นของหัวใจ และสีผิว การดูแลทารกปกติ ทำให้ทางเดินหายใจโล่ง เช็ดตัวให้แห้ง ประเมินสีผิว หายใจเอง สังเกตอาการ การดูแลภายหลัง การช่วยกู้ชีพ 100 สีผิวแดง การหายใจมีประสิทธิภาพ อัตราการ เต้นของหัวใจ 60 60 30 วินาที ใช่ * พิจารณาใส่ท่อหายใจ
 เช็ดตัวให้แห้ง กระตุ้นให้หายใจ. และจัดท่าศีรษะใหม่ ไม่ใช่ แรกเกิด. ให้ออกซิเจน* ยังคงเขียวตลอด. ให้การช่วยหายใจ * ด้วยแรงดันบวก * หยุดหายใจหรือ. อัตราการเต้นของ. หัวใจ 100. หายใจได้เองและ. หัวใจ 100. แต่ยังคงเขียว. ประเมินการหายใจ. อัตราการเต้นของหัวใจ. และสีผิว. การดูแลทารกปกติ ทำให้ทางเดินหายใจโล่ง. เช็ดตัวให้แห้ง. ประเมินสีผิว. หายใจเอง. สังเกตอาการ. การดูแลภายหลัง. การช่วยกู้ชีพ. 100. สีผิวแดง. การหายใจมีประสิทธิภาพ. อัตราการ. เต้นของหัวใจ. 60. วินาที ใช่ * พิจารณาใส่ท่อหายใจ.")
61
สิ่งสำคัญที่ควรทราบ จากแผนภูมิขั้นตอนการช่วยกู้ชีพ
อัตราการเต้นของหัวใจ 60 ครั้ง/นาที ให้การช่วยกู้ชีพตามขั้นตอนต่อไป อัตราการเต้นของหัวใจ 60 ครั้ง/นาที หยุดกดหน้าอก อัตราการเต้นของหัวใจ 100 ครั้ง/นาที และหายใจได้เอง หยุดการช่วยหายใจด้วยแรงดันบวก To follow the resuscitation flow diagram, it is important to remember the following heart rates and time sequences. Instructor Tip: The flow diagram may look complex at first, but the Neonatal Resuscitation Program (NRP) takes you through each step. Practice helps ensure rapid, simultaneous assessment of the newborn and timely interventions. เครื่องหมาย () ในแผนภูมิแสดงถึง ความจำเป็นที่อาจต้องการ การใส่ท่อช่วยหายใจ (endotracheal intubation) ถ้าทารกอาการไม่ดีขึ้น ภายใน 30 วินาที ภายหลังการช่วยเหลือ แต่ละขั้นตอน ควรให้การช่วยเหลือขั้นต่อไป
 takes you through each step. Practice helps ensure rapid, simultaneous assessment of the newborn and timely interventions. เครื่องหมาย () ในแผนภูมิแสดงถึง ความจำเป็นที่อาจต้องการ การใส่ท่อช่วยหายใจ (endotracheal intubation) ถ้าทารกอาการไม่ดีขึ้น ภายใน 30 วินาที ภายหลังการช่วยเหลือ แต่ละขั้นตอน ควรให้การช่วยเหลือขั้นต่อไป.")
62
การดูแลทารกหลังจากช่วยกู้ชีพแล้ว
ทารกต้องการ การติดตามอย่างใกล้ชิด ความดันโลหิต อัตราการเต้นของหัวใจ Oxygen saturation หรือ สีผิว การตรวจทางห้องปฏิบัติการ ความเข้มข้นของเลือด (Hematacrit) น้ำตาลในเลือด (Glucose) เคราะห์ก๊าซในเลือด (Blood gas) การดูแลภาวะแทรกซ้อน Do not assume that a newborn who has been resuscitated successfully is normal and can be treated as a routine newborn. If substantial resuscitation was required, the newborn should be cared for in an environment where close monitoring and anticipatory care can be provided. Also monitor and manage oxygenation, infection, blood pressure, fluids, apnea, blood sugar, feeding, and temperature.
 น้ำตาลในเลือด (Glucose) เคราะห์ก๊าซในเลือด (Blood gas) การดูแลภาวะแทรกซ้อน. Do not assume that a newborn who has been resuscitated successfully is normal and can be treated as a routine newborn. If substantial resuscitation was required, the newborn should be cared for in an environment where close monitoring and anticipatory care can be provided. Also monitor and manage oxygenation, infection, blood pressure, fluids, apnea, blood sugar, feeding, and temperature.")
63
ภาวะแทรกซ้อนที่พบได้หลังการช่วยกู้ชีพ
ทารกแรกเกิดที่ต้องการการช่วยกู้ชีพ ต้องได้รับการเฝ้าระวังและให้การรักษาปัญหาต่อไปนี้ ภาวะความดันโลหิตในปอดสูง ปอดอักเสบ หรือ ภาวะแทรกซ้อนทางปอดอื่นๆ ภาวะเลือดเป็นกรด ภาวะความดันเลือดต่ำ การให้สารน้ำ ภาวะชัก หรือ หยุดหายใจ ภาวะน้ำตาลในเลือดต่ำ ปัญหาการให้อาหาร การควบคุมอุณหภูมิ Pulmonary hypertension may result in babies who have been stressed at birth. Avoid episodes of hypoxemia after resuscitation and monitor oxygenation with an oximeter and/or arterial blood gases. Instructor Tip: Episodes of hypoxia, which may exacerbate persistent pulmonary hypertension, can be caused by suctioning or other interruptions in oxygen administration and stimulation from excessive handling, light, and noise. Resuscitated babies are at higher risk for developing pneumonia, from aspiration or a congenital infection. Metabolic acidosis results from a buildup of lactic acid, which forms when tissues have insufficient oxygen. If giving sodium bicarbonate, be certain that ventilation of the lungs is adequate. Hypotension may follow perinatal compromise. Monitor heart rate and blood pressure closely. Volume expansion may be indicated. Renal dysfunction is usually transient but can cause electrolyte and fluid shifts. Check urine output, body weight, and serum electrolyte levels frequently for the first few days after birth. Seizures or apnea may appear several hours following perinatal compromise as symptoms of HIE. Monitor hypoglycemia and electrolytes because seizures and apnea can also be caused by metabolic abnormalities. Glucose stores are depleted rapidly during perinatal compromise. Check blood glucose levels soon after resuscitation and sequentially. IV glucose is often necessary. The newborn GI tract is sensitive to hypoxia-ischemia and at risk for ileus, GI bleeding, and even necrotizing enterocolitis. IV fluids and nutrition may be required for several days. Do not overheat the baby during and after resuscitation. Maintain baby’s temperature in normal range.

64
การควบคุมอุณหภูมิ การทำให้ทารกมีอุณหภูมิกายสูง (hyperthermia) ก่อให้เกิดอันตรายกับทารก ดังนั้นควรระมัดระวัง ไม่ให้ทารกมีอุณหภูมิกายสูงเกินไป ระหว่างหรือ ภายหลังการช่วยกู้ชีพ
 ก่อให้เกิดอันตรายกับทารก ดังนั้นควรระมัดระวัง ไม่ให้ทารกมีอุณหภูมิกายสูงเกินไป ระหว่างหรือ ภายหลังการช่วยกู้ชีพ.")
65
ทำไมทารกที่เกิดก่อนกำหนดจึงมีความเสี่ยงสูงมากกว่าปกติ
ปอดยังขาดสารลดแรงตึงผิวของถุงลม (surfactant) สมองยังพัฒนาไม่เต็มที่ อาจทำให้ควบคุมการหายใจได้ไม่ดี มีการสูญเสียความร้อนได้ง่าย และควบคุมอุณหภูมิร่างกายได้ไม่ดี มีความเสี่ยงสูงต่อการติดเชื้อ หลอดเลือดในสมองเปราะบางมาก อาจทำให้มีเลือดออกในสมองได้ง่าย มีความเสี่ยงต่อการเกิดความดันโลหิตต่ำหรือช็อคได้ง่ายเมื่อมีการเสียเลือด กล้ามเนื้ออ่อนแรง ทำให้หายใจเองได้ลำบาก เนื้อเยื่อยังเจริญไม่สมบูรณ์ จึงเสี่ยงต่อการถูกทำลายจากการได้รับออกซิเจนที่มากเกินไป Premature babies have anatomical and physiologic characteristics that are quite different from babies born at term. These and other unique characteristics present special challenges during resuscitation of premature babies. These and other aspects of prematurity should alert you to seek extra help when anticipating a preterm birth. (See Lesson 8.)
 สมองยังพัฒนาไม่เต็มที่ อาจทำให้ควบคุมการหายใจได้ไม่ดี มีการสูญเสียความร้อนได้ง่าย และควบคุมอุณหภูมิร่างกายได้ไม่ดี มีความเสี่ยงสูงต่อการติดเชื้อ. หลอดเลือดในสมองเปราะบางมาก อาจทำให้มีเลือดออกในสมองได้ง่าย. มีความเสี่ยงต่อการเกิดความดันโลหิตต่ำหรือช็อคได้ง่ายเมื่อมีการเสียเลือด. กล้ามเนื้ออ่อนแรง ทำให้หายใจเองได้ลำบาก. เนื้อเยื่อยังเจริญไม่สมบูรณ์ จึงเสี่ยงต่อการถูกทำลายจากการได้รับออกซิเจนที่มากเกินไป. Premature babies have anatomical and physiologic characteristics that are quite different from babies born at term. These and other unique characteristics present special challenges during resuscitation of premature babies. These and other aspects of prematurity should alert you to seek extra help when anticipating a preterm birth. (See Lesson 8.)")
งานนำเสนอที่คล้ายกัน







>")



>")
>")

>")




