ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
โดย มณีพรรณ์ เหล่าโพธิ์ศรี สุปรียา ราชสีห์
Case conference โดย มณีพรรณ์ เหล่าโพธิ์ศรี สุปรียา ราชสีห์

2
Personal data : ผู้ป่วยชายไทยคู่ อายุ 49 ปี อาชีพ รับราชการ
ที่อยู่ อ.น้ำพอง จ.ขอนแก่น Medical diagnosis : HCV with liver cirrhosis child Ward : SICU Chief complaint : secretion accumulation and decrease lung volume

3
Subjective examination :
Present history : - ปี 2550 ผู้ป่วยมีอาการอ่อนเพลีย แน่นท้อง จึงไปพบแพทย์ แพทย์ได้ตรวจ US และ CT upper abdomen จึงได้วินิจฉัยว่าเป็น liver cirrhosis with portal hypertention and portosystemic collaterals ได้รับการรักษาทางยามาเรื่อยๆ

4
Past history: วันที่ 10 มิ.ย. 2551 ผู้ป่วยได้รับการผ่าตัด
liver transplantation ด่วน เวลา น. – น. - 11 มิ.ย. 51 แพทย์ส่งปรึกษานักกายภาพบำบัด Past history: - no underlying - ปฏิเสธการแพ้ยา - เคยผ่าตัดลำไส้ทะลุ เมื่อ 20 ปีที่ผ่านมา

5
Medical assessment : - US of upper abdomen วันที่ 24 เม.ย cirrhotic liver with portal hypertension with 0.7 cm gallstone - CT of upper abdomen วันที่ 26 พ.ย liver cirrhosis with portal hypertension and portosystemic collaterals no evidence of hepatoma. Minimal ascitis at Rt.subphenic region Lt. renal cortical cysts.

6
- Vital sign วันที่ 11 มิ.ย. 2551 BP : 136/42* RR : 24 Pulse : 50* Temp : 37 Analysis : diastolic hypotension and tachycadia

7
-ABG on oxigen 10 l/min normal Assessed value PH 7.57* PCO2 35- 45 38 PO2 156* BE 12.8* HCO3 22 -26 34.8* O2 100 Interpretation : Metabolic alkalosis

8
Interpretation : - Anemia
- CBC วันที่ 11 มิ.ย.51 Item Normal value Assessed value Hb 12-15 g/dl 7* Hct % 21.3* Wbc 4,500 – 11,500 cell/mm³ 4,700 Plt 140, ,000cell/mm³ 88,000* Interpretation : - Anemia - เกล็ดเลือดต่ำ อาจมีปัญหาม้ามโตในผู้ป่วยโรคตับ

9
- Clinical Chemistry Laboratory วันที่ 11 มิ.ย. 51
Item Normal value Assessed value BUN 27.5* Cr 1.6* Na 145 K 3.7 HCO3 32.7* Cl 105 Ca 8.9 PO4 4.2 Chol 75* Abl 3.4* Glob 1.9* ALT 4- 36 344* AST 12- 32 516* Interpretation : มีการอักเสบของตับ

10
Objective examination
General observation - Sthenic body built, Good conciousness&cooperation On O2 mask with reseurviour bag O2 flow 10 LPM No sign of central and peripheral cyanosis, No dry skin Incision at adbminal Abdominal distention On abdominal drainage tube, on pulse oxemiter, on IV fluid upper chest breathing pattern Short of breathing Ineffective cough (can not deep inhale) Pain at incision line ADL: Lying to sitting maximal assistance
 Pain at incision line. ADL: Lying to sitting maximal assistance.")
11
-Symmetry of chest movement
Palpation -Symmetry of chest movement - No rhonchal fremitus - No subcutaneous emphysema - Pitty edema at both foot

12
Auscultation - Decrease breath sound at both lower lobe
-No adventitious sound

13
Neuromuscular system Muscle tone: Normal Muscle length: Normal
Muscle power: Grade 5 of all limb PROM: Full ROM of all joints in all directions. Active ROM: Full ROM of all joints in all directions

14
Problem list 1. Decrease lung volume - due to post op (pain)
- decrease deep breath -Abdominal distention 2. Abnormal breathing pattern - Decrease lung volume -Pain 3. Maximal dependent ambulation

15
Goal of treatment Short term goal 1. Improve lung volume
2. Normal breathing pattern 3. Independent ambulation Normal function Long term goal

16
Plan of treatment Airway clearance - Airway clearance technique.
Re - expansion lung - Active chest mobilization Strengthening inspiratory muscle - Inspiratory muscle loading exercise - Breathing exercise Encourage ambulation

17
Plan of treatment (cont.)
Education and ward program to - ผู้ป่วยปฏิบัติตัวได้ถูกต้อง - Prevent complication.

18
Treatment Chest Physical therapy
Breathing exercise 6 times/set/hour , every hours - Diaphragmatic breathing - Lower costal breathing 2. Coughing training 3 times / set , 2 sets / hour, every hours 3. Active chest mobilization 10 times/set 6 sets/day

19
Therapeutic exercise - ward program Treatment (cont.)
Inspiratory muscle loading - Incentive spirometry 6 times / set , 5 sets / hour, every hours Therapeutic exercise -Pumping exs. - Active free exercise for all limb. -Ambulation training : lying to sitting walking - ward program

20
S : ผู้ป่วยสดชื่นดี ให้ความร่วมมือในการรักษา ไม่หอบเหนื่อย
Progression note วันที่ 13 มิ.ย. 2551 S : ผู้ป่วยสดชื่นดี ให้ความร่วมมือในการรักษา ไม่หอบเหนื่อย สามารถลุกขึ้นนั่งห้อยขาข้างเตียงและยืนข้างเตียงได้ vital sign normal ABG Item normal Assessed value PH 7.52* PCO2 35- 45 44 PO2 205* BE 0 +- 2 12.7* HCO3 22 -26 35.9* O2 sat 100 On canula 5 LPM Interpretation : Metabolic alkalosis

21
Interpretation : Anemia
CBC วันที่ 13 มิ.ย.51 Item Normal value Assessed value Hb 12-15 g/dl 10* Hct % 31.6* Wbc 4,500 – 11,500 cell/mm³ 5,800 Plt 140, ,000cell/mm³ 69,000* Interpretation : Anemia - เกล็ดเลือดต่ำ อาจมีปัญหาม้ามโตในผู้ป่วยโรคตับ

22
Clinical Chemistry Laboratory วันที่ 13 มิ.ย. 51
Item Normal value Assessed value BUN 41.4* Cr 1.2 Na 135 K 3.2 CHO3 28.9* Cl 96 Ca 7.8* PO4 Chol 93* Abl 3.9 Glob 2* ALT 4- 36 584* AST 12- 32 72* Interpretation : มีการอักเสบของตับ

23
O : -Dullness at both lungs
Medical assessment : - CXR : Plueral effusion in both lungs O : -Dullness at both lungs - No rhoncal fremitus - Auscultation - Decrese breath sound at both lower lobe - Pleural fiction rub at both lungs

24
A : หลังจากผ่าตัดได้ 3 วันผู้ป่วยอาการดีขึ้น สามารถเคลื่อนไหวตัวเองได้มากขึ้น จึงทำให้ผู้ป่วยสามารถฝึกนั่ง ฝึกยืนข้างเตียงได้ เนื่องมาจากการที่ผู้ป่วยมีอาการปวดที่บริเวณแผลที่ได้รับการผ่าตัดลดลง ส่วนปัญหาทางด้านทรวงอก จาก Chest X-ray พบ Pleural effusion อาจเนื่องมาจากผลของการผ่าตัด ดังนั้นการรักษาทางกายภาพจึงน่าจะเพิ่มการฝึกการกระตุ้นการดูดกลับของของเหลวและกระตุ้นการเคลื่อนไหวเพื่อให้ปอดมีการขยายตัวได้มากขึ้น P: Add ACBT and Swedish pleurisy exercise, exs. to increase functional movement , increase ambulation, other same.

25
Interpretation : Hyperoxigenation
วันที่ 17 มิ.ย. 2551 S : ผู้ป่วยเริ่มเคลื่อนไหวตัวได้มากขึ้น หน้าตาสดชื่น off drain แล้ว สามารถนั่ง ยืน ข้างเตียงได้เอง ผู้ป่วยสามารถเดินได้รอบเตียง vital sign normal ABG normal 17 มิ.ย.51 PH 7.41 PCO2 35- 45 36 PO2 118* BE 0 +- 2 -1.3 HCO3 22 -26 23.5 O2 sat 99 Interpretation : Hyperoxigenation

26
Medical assessment : CXR วันที่ 14 มิ.ย. 2551 : Plueral effusion improve form 13/6/51. : 16 /6/51 ; Rt. Lower lobe atelectasis O : - No ICD - No rhoncal fremitus - Auscultation Decrease breath sound at Rt. lower lobe

27
A : จากผล chest X-ray พบ Pleural effusion ลดลงบ้างแล้ว แต่มีปัญหา RLL atelectasis อาจเนื่องมาจากผู้ป่วยยังหายใจเข้าลึกไม่พอ และอาจจะเป็นผลจากการผ่าตัดทำให้เกิดการจำกัดการขยายตัวของปอดและผู้ป่วยยังปวดแผลอยู่จึงทำให้เกิดปอดแฟบได้ ดังนั้นการรักษาทางกายภาพบำบัดจะเน้นเพิ่มการฝึกหายใจเข้าลึก P : - Same add Rt. unilateral costal breathing exercise with sustain maximum inspiration 6 times / set , 5 sets / hour, every hours - Paced br. ex เดินรอบๆ เตียงได้ประมาณ 6 รอบ

28
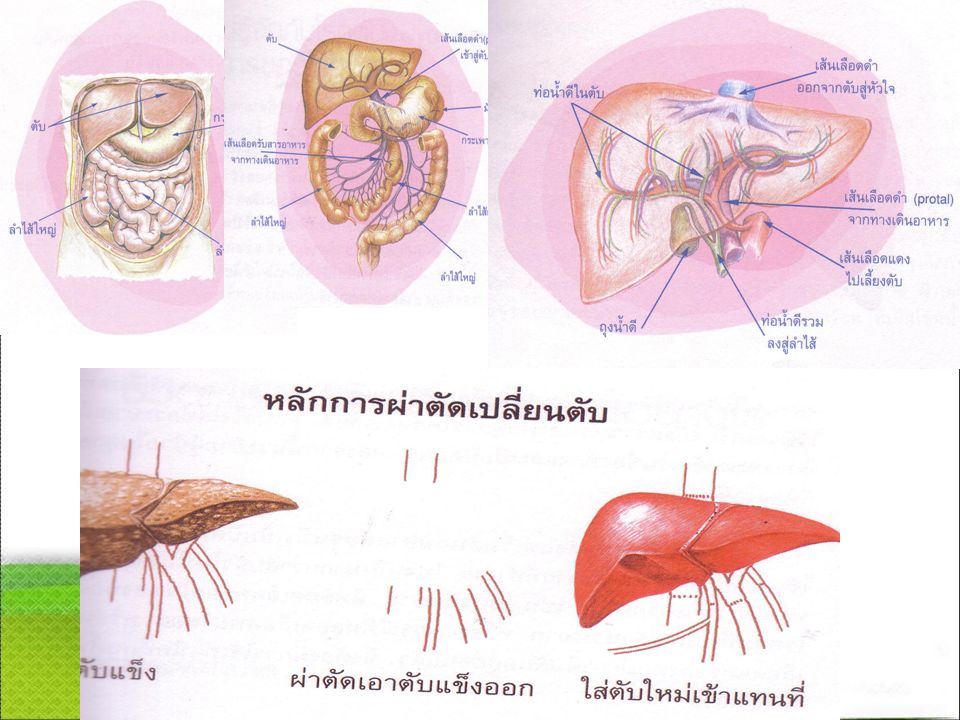
Liver transplantation
Discussion Liver transplantation สาเหตุ อาการ การรักษาโดยการผ่าตัด ภาวะแทรกซ้อน กายภาพบำบัด

30
ภาวะแทรกซ้อนจากการเปลี่ยนตับ
Discussion กายภาพบำบัด ภาวะแทรกซ้อนจากการเปลี่ยนตับ 1. Decrease lung volume 2. Abnormal breathing pattern 3. Maximal dependent ambulation 4. pain 1. การติดเชื้อ 2.ภาวะต้านตับ 3.แทรกซ้อนจากยา 4.เกิด HT 5.ท่อน้ำดีของตับตีบ-ตัน 6.กลับเป็นตับอักเสบซ้ำ

31
ขอบคุณค่ะ

งานนำเสนอที่คล้ายกัน











 98.08% 100.02% จังหวัด.>")







