ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
นายแพทย์ชำนาญการพิเศษ
Peripheral Arterial Disease :PAD นพ.ธีรพล เกาะเทียน นายแพทย์ชำนาญการพิเศษ ศัลยแพทย์โรคหัวใจ หลอดเลือด และทรวงอก โรงพยาบาลสรรพสิทธิประสงค์ อุบลราชธานี

2
Introduction PAD caused by atherosclerotic occlusion of arteries to legs Prevalence 12% and increases to 20% if persons older than 70 yr. Affects men and women equally pt. with PAD , even absence of Hx of MI or ischemic stroke have same relative risk of death from CVS cause as pt. with Hx of CAD or CVD

3
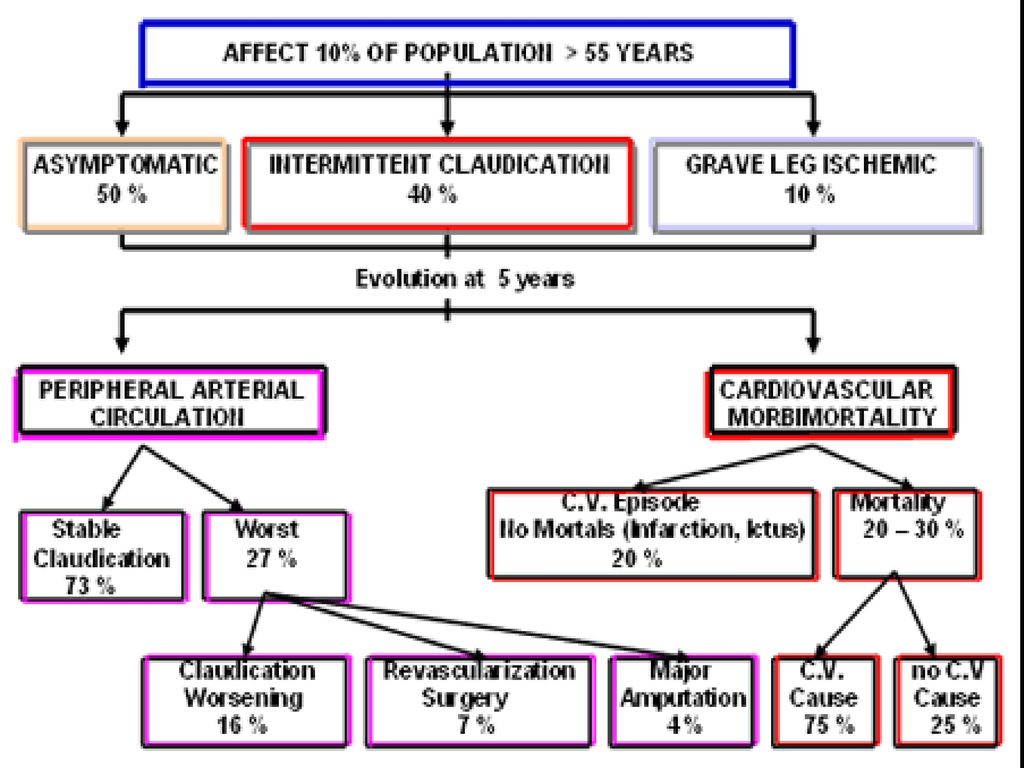
Introduction Rate of death of all causes equal in men and women and is elevated even in asymptomatic pt. Severity of PAD is closely associated with risk of MI , ischemic stroke , and death from vascular cause Lower ABI – greater risk of CVS events Critical leg ischemia – mortality of 25%

4
RISK FACTOR Smoking DM HT Hypercholesterolemia

5
Normal Artery and Artery With Plaque Buildup

6
PAD in THAILAND Male % Female % Risk Factor Age DM > 12 yrs HT

7
A Life Threatening Condition
The REACH (Reduction of Atherothrombosis for Continued Health) Registry has expanded mortality associated with PAD At one year, 19% of the PAD population had experienced either an MI, a stroke or were hospitalised for an atherothrombotic event or had died from CV causes compared to 10% of the CAD population and 7% of CVD population.
 Registry has expanded mortality associated with PAD. At one year, 19% of the PAD population had experienced either an MI, a stroke or were hospitalised for an atherothrombotic event or had died from CV causes compared to 10% of the CAD population and 7% of CVD population.")
8
PAD vs DM DM ทำให้เพิ่มความชุกของ PAD 2เท่า
50% จะถูกตัดเพิ่ม 50% ถูกตัดอีกข้าง ภายใน 2 ปี 50% ที่ถูกตัดขา เสียชีวิต ภายใน 5 ปี

9
Clinical Staging of LEAD

11
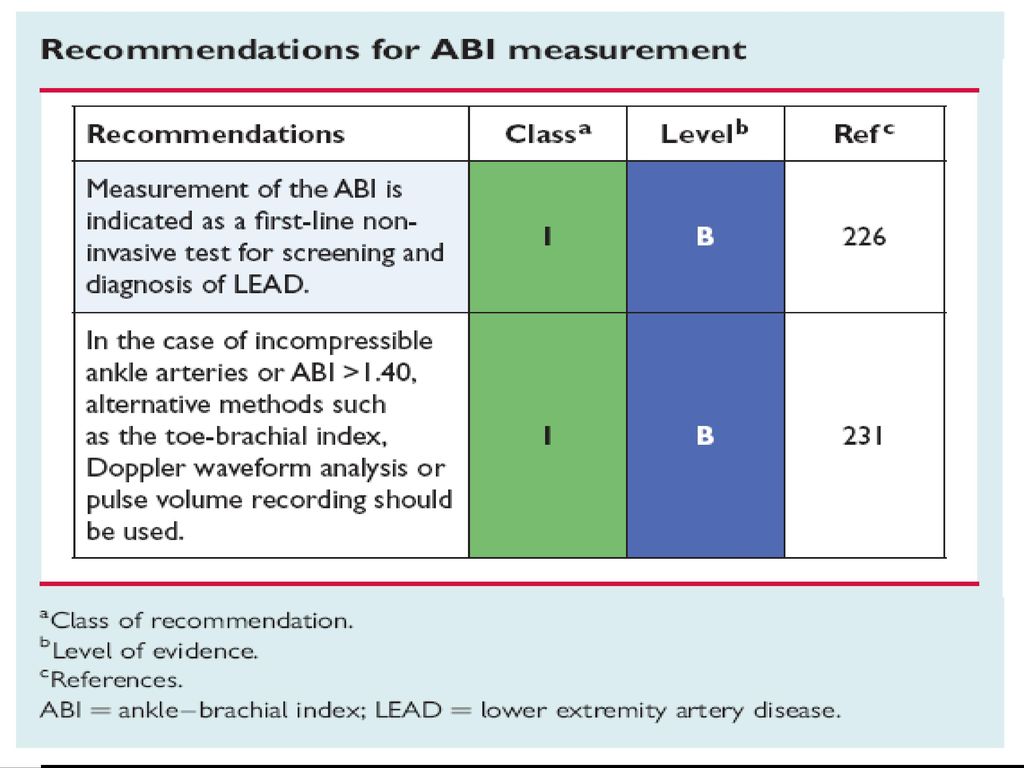
Screening for PAD ABI Selection of patient high risk DM Age 50 years.

13
Ankle-Brachial Index (ABI)
")
14
INTERPRETATION NORMAL 0.9 -1.30 MILD 0.7-0.89 MODERATE 0.4-0.69
SEVERE < 0.4 POORLY COMPRESSIBLE > 1.3

15
TREATMENT งดสูบบุหรี่ ออกกำลังกาย ควบคุม ความดัน (140/90 mmHg)
LDH < 100 Medication Endovascular treatment Surgery

17
การประเมินผู้ป่วยที่มีอาการ Claudication
ผู้ป่วยที่มีอาการแบบ classic claudication ตรวจร่างกายระบบหลอดเลือด ตรวจ resting ankle - brachial index (resting ABI) ABI ≤ 0.90 ABI > 0.90 - Exercise ABI - Toe-brachial index - Segmental pressure measurement - Duplex ultrasound exam. Confirmation of PAD diagnosis Abnormal results Normal results No PAD or consider arterial entrapment syndrome - Risk factors normalization - Pharmacological risk การรักษาภาวะ claudication
 ABI ≤ ABI > Exercise ABI. - Toe-brachial index. - Segmental pressure measurement. - Duplex ultrasound exam. Confirmation of. PAD diagnosis. Abnormal results. Normal results. No PAD or consider arterial entrapment syndrome. - Risk factors normalization. - Pharmacological risk. การรักษาภาวะ claudication.")
19
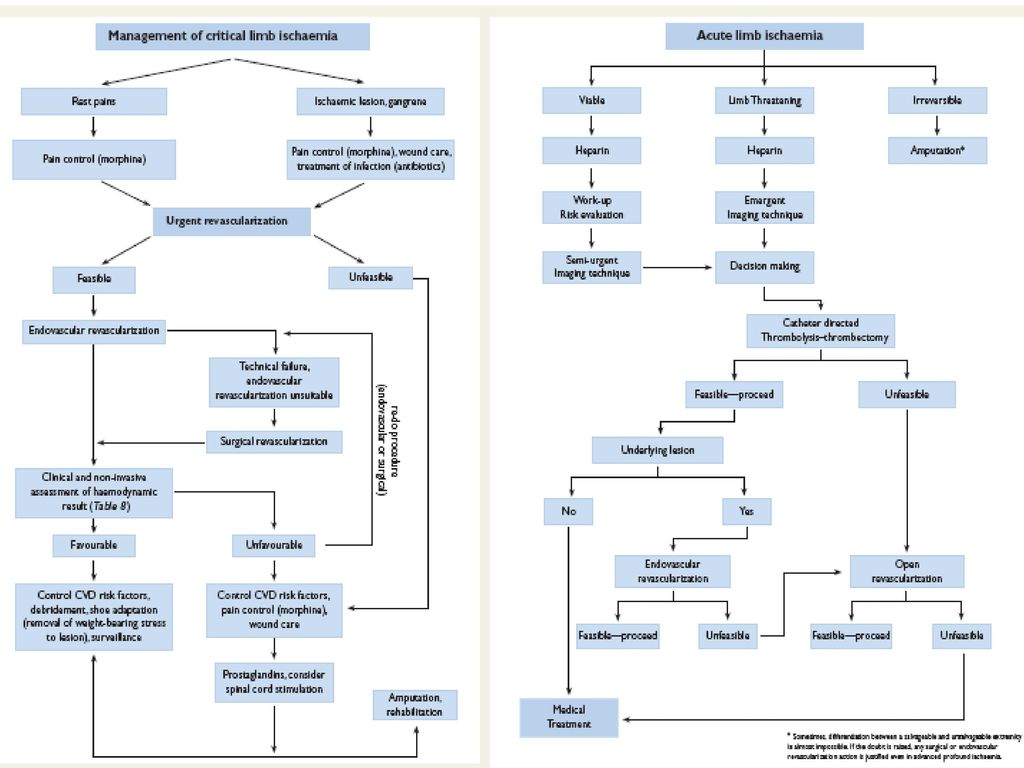
Intervention of PAD

20
Toe gangrene in a patient with diabetes
21
AORTO-ILIAC LESIONS Description Lesion type Type A Type B
* Unilateral or bilateral single short (≤3cm) stenosis of EIA * Unilateral or bilateral stenosis of CIA * Single or multiple stenosis totaling 3-10cm. Involving the EIA occlusion not involving the origins of internal iliac of CFA * Unilateral CIA Occlusion * Short (≤3cm) stenosis of infrarenal aorta
 stenosis of EIA. * Unilateral or bilateral stenosis of CIA. * Single or multiple stenosis totaling 3-10cm. Involving the EIA occlusion not involving the origins of internal iliac of CFA. * Unilateral CIA Occlusion. * Short (≤3cm) stenosis of infrarenal aorta.")
22
AORTO-ILIAC LESIONS Description Lesion type Type C Type D
* Heavily calcified unilateral EIA occlusion with or without involvement of origins of internal iliac and/or CFA * Unilateral EIA occlusion that involves the origins of internal iliac and/or CFA * Unilateral EIA stenosis extending tnto the CFA * Bilateral EIA stenosis 3-10cm long not extending into the CFA * Bilateral CIA occlusion * Bilateral occlusion of EIA * Iliac stenosis in patients with AAA requiring treatment and not amenable to endograft placement or other laesions requiring open aortic or iliac surgery * Unilateral occlusions of both CIA and EIA * Diffuse multiple stenosis involving the unilateral CIA, EIA and CFA * Diffuse disease involving the aorta and both iliac arteries requiring treatment * Infra-renal aorto-iliac occlusion

23
FEMORAL-POPLITEAL LESIONS
Lesion type Type A Type B Description * Single occlusion ≤5cm in length * Single stenosis ≤10cm in length * Single popliteal stenosis * Heavily calcified occlusion ≤5cm inlength * Single or multiple lesions in the absence of continuous tibial vessels to improve inflow for a distal bypass * Single stenosis or occlusion ≤15cm not involving the infra geniculate popliteal artery * Multiple lesions (stenoses or occlusion),each ≤5cm
,each ≤5cm.")
24
FEMORAL-POPLITEAL LESIONS
Lesion type Type C Type D Description * Recurrent stenoses or occlusion that need treatment after two endovascular interventions * Multiple stenoses or occlusions totaling >15cm with or without heavy calcifications * Chronic total occlusion of popliteal artery and proximal trifurcation vessels * Chronic total occlusion of CFA of SFA (>20cm, involving the popliteal artery)
")
25
THANK YOU Question ?

งานนำเสนอที่คล้ายกัน








>")




 trial: factorial randomised placebo controlled trial of aspirin and antioxidants.>")


>")



