ดาวน์โหลดงานนำเสนอ
1
Interhospital conference

2
เด็กชายไทย อายุ 4 เดือน ภูมิลำเนา จ.ปทุมธานี
CC; มีตุ่มหนองขึ้นตามตัว 2 สัปดาห์ก่อนมา รพ. PI ; 2 สัปดาห์ก่อนมารพ. มีไข้สูง เป็นๆหายๆ ไอมีเสมหะ น้ำมูกใสช่วงแรก ต่อมาข้นสีขาว ไม่มีหายใจหอบเหนื่อย ไปรักษา รพ.เอกชน ได้ยาแก้อักเสบมาทาน ต่อมามีตุ่มหนอง 6-7 ตุ่มที่ศีรษะ ร้องกวน และผื่นขึ้นมากขึ้น กระจายจากศีรษะไป คอ หลัง หน้าอก ปัสสาวะอุจจาระปกติ

3
PH ; c/s due to abnormal presentation BW 3000gm Development ; ยิ้มได้ มองจ้องหน้า คอแข็ง Nutrition ; นม 4 oz x 5-6 ขวด เริ่มทานกล้วยบด ตอนอายุ 3 เดือน Vaccination ; รับvaccine ช่วงแรกเกิด

4
PE ; V/S: Temp = 37.8 c , RR = 46 /min, PR= 110 /min , BP = 90 / 50 mmHg BW 5 kg, length 55 cm, HC 38 cm GA :active , mild pale HEENT : AF 4x4 cm, no jx, no injected pharynx Lung: clear ,no adventitious sound Heart: regular no murmur Abdomen : liver 3 cm below right costal margin spleen 2 cm below right costal margin Extremities : BCG abscess at lt arm 1 cm Skin : generalized erythematous papule and pustule at back,neck, head

5
Discussion

6
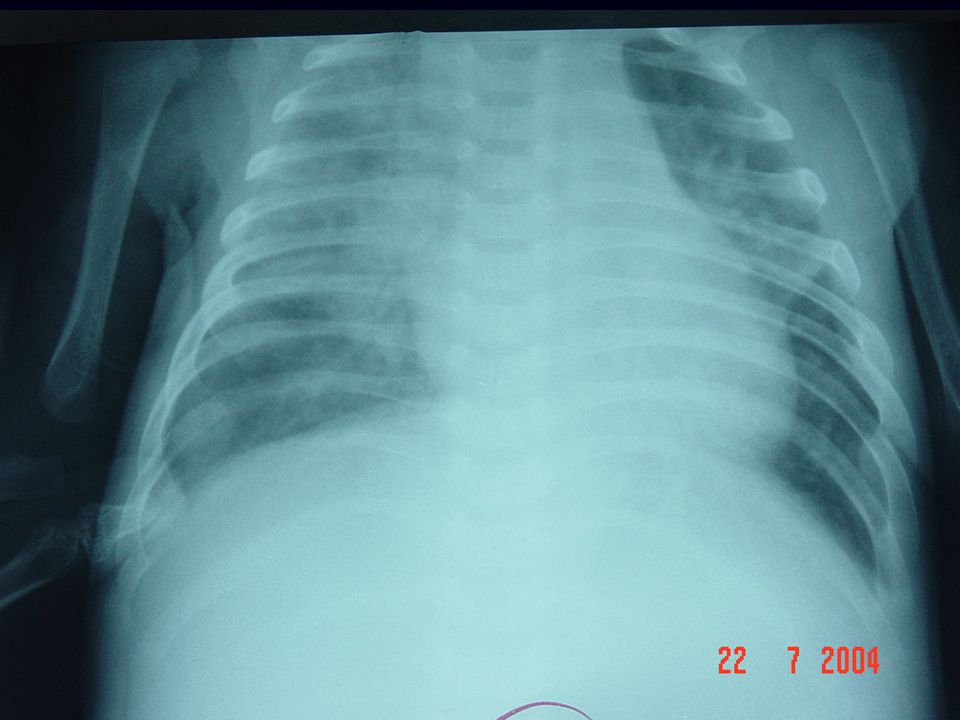
Problem list ; 1)pyoderma 2)pneumonia 3)BCG abscess 4) hepatosplenomegaly
pyoderma 2)pneumonia 3)BCG abscess 4) hepatosplenomegaly")
7
Investigation 1 1 5 9 2 6 11 3 7 12 4 8 Investigation 2

8
Investigation CBC : Hb 9.5 Hct 25%
WBC (PMN 47 ,M 10 ,L 40, E 3%) plt 400,000 hypochromic2+, microcytic 1+ U/A : clear, spec 1.005, pH 7, other neg
 plt 400,000. hypochromic2+, microcytic 1+ U/A : clear, spec 1.005, pH 7, other neg.")
9
Investigation pus (skin) G/S : Gram positive cocci in cluster
 G/S : Gram positive cocci in cluster")
10
Investigation Day2 : dyspnea , sternal and subcostal retraction

11
Discussion

12
Treatment ; cloxacilin + gentamycin iv

13
Investigation Pus(skin) C/S : Staphylocccus aureus
H/C : Staphylococcus coagulase negative (MRSE)
")
14
Investigation H/C : x 2 specimens
Staphylococcus coagulase negative x 2 specimens sensitive : cloxacillin

15
Investigation BCG abscess pus Gram stain : -ve AFB : +ve

16
Investigation Gastric lavage for AFB x3 days : negative

17
Investigation Bronchroscopy; consistent c chronic inflammation
(non specific) PCP, AFB : negative C/S : Staphylococcus coagulase negative
 PCP, AFB : negative. C/S : Staphylococcus coagulase negative.")
18
Investigation Anti HIV –ve

19
CMV IgM +ve Rubella IgM -ve HSV IgM -ve Toxoplasma IgM -ve

20
Investigation F/U : อาการ ไม่ดีขึ้น , ไข้ หายใจหอบ H/C : MRSE
Treatment : vancomycin ผู้ป่วยขอกลับบ้าน-> fucidin+ rifampicin (3wk)
")
22
Second admission CC; ไข้ หายใจหอบเหนื่อย 6 วัน
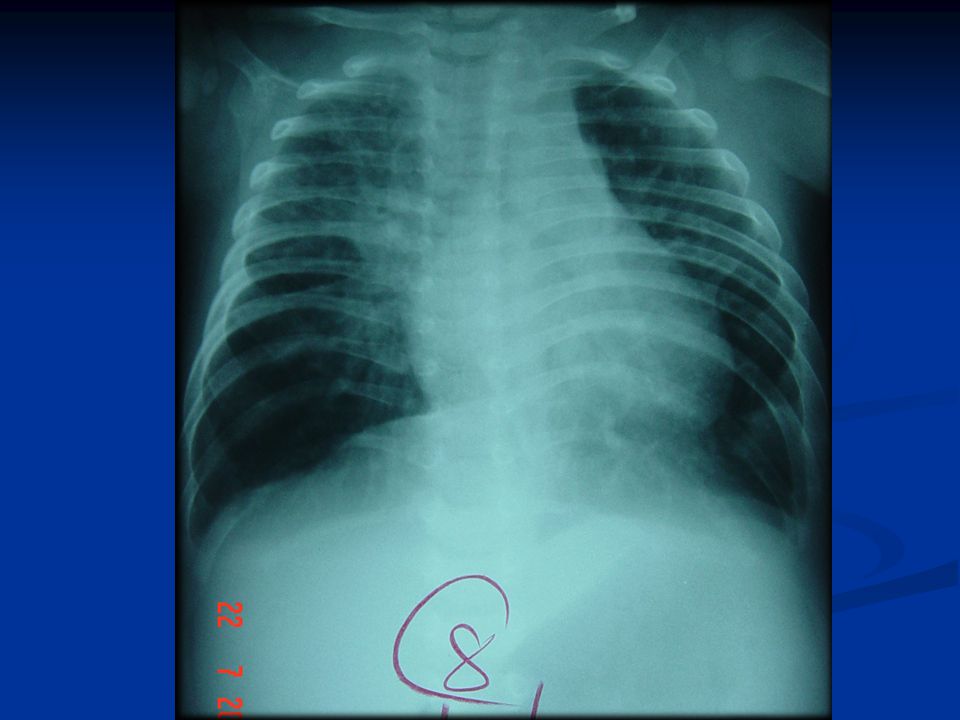
PI; หลังจากกลับบ้าน 1 wk ผู้ป่วยเริ่มมีอาการหอบเหนื่อย มีไข้ มีผื่นแดงและตุ่มหนองตามศรีษะและลำตัว ก้อนที่ขาหนีบซ้ายโต ไปรพ. รามา ได้admit CXR – alveolar infiltration มี axillary and inguinal lymphadenopathy ได้ทำ fine needle aspiration axillary lymphnode - neutrophilic infiltration with minimal lymphoid necrosis and much granuration tissue reaction consistent with necrotizing granulomatous lymphadenitis Dx TB ได้ให้ IRZS 2 วันจึงส่งตัวมารักษาต่อที่ รพ.ธรรมศาสตร์

23
PE : V/S : BT 37.8 c, RR 60 /min GA : dyspnea ,mild retraction Lung : normal BS Heart : normal s1 s2 , no murmur Abdomen : liver 3 cm below RCM, span 8 cm LN : Lt axillary LN 4x5 cm , Lt inguinal LN 2 cm skin : generalized pustule and erythematous papule

26
Investigation; CBC WBC 14,600 PMN 44 %, L 42% Hb 11,Hct 32, plt CXR; alveolar infiltration

28
Discussion

29
Investigation 2 Investigation 1

30
Investigation Pyoderma Pus Gram stain : not found organism

31
Investigation Skin biopsy : rupture folliculitis, supurative granulomatous lesion Skin biopsy culture for bacteria, TB , fungus : no growth

32
Investigation Left axillary LN : AFB + , MAFB - Culture

33
Investigation Left inquinal LN : Gram stain : negative AFB : negative
Culture : Torulopsis glabata

34
Investigation Gastric content : AFB -ve Culture TB -ve

35
Investigation Hemo culture for TB : no growth

36
Investigation T cell subpopulation : CD3 : 5,396 (62.3%)
")
37
Investigation PPD 13 mm.

38
Investigation Immunoglobulin level IgA 95.5 mg/dl IgM 132.2 mg/dl
IgG 1250 mg/dl IgE 76 mg/dl CD 19 : 2,524 (29.14%)
")
39
Investigation for phagocytic function
Quality : absolute neutrophil count 7,560 /mm3 Function : nitroblue tetrazolium dye test – abnormal dihydrorhodamine (DHR) reduction - abnormal
 reduction - abnormal.")
40
Chronic granulomatous disease
Diagnosis Chronic granulomatous disease

41
The NBT test

42
Chronic Granulomatous Disease
Smear in slide, stain, count no. of PMN w/c reduce NBT dye to a blue formozan precipitate in 100 PMN Normal : > 50%

43
DHR assay a fluorescent flow cytometry assay
conversion of dihydroxyrhodamine 123 (DHR) to rhodamine 123 which detects hydrogen peroxide After stimulate w/ PMA (Phorbol myristate acetate) The DHR method can diagnose CGD And also suggest the CGD genotype
 to rhodamine 123. which detects hydrogen peroxide. After stimulate w/ PMA (Phorbol myristate acetate) The DHR method can diagnose CGD. And also suggest the CGD genotype.")
44
DHR assay The results of the DHR assay in this patient show abnormal oxidative burst with stimulation index of < 10 on two occasions. This result compatible with X-linked CGD.

45
Clinical course Treatment; INH , Rifampin ,PZA, Streptomicin
Fluconazone

46
Clinical course Recurrent axillary lymphadenitis
Recurrent inquinal lymphadenitis Recurrent pneumonia Recurrent perianal abscesses Rcurrent skin infection

47
Investigation Left axillary LN : AFB + , MAFB - Culture for TB : -ve
PCR for TB : -ve PCR for M. bovis : -ve PCR for M. fortuitum : -ve

48
Clinical course Recurrent axillary lymphadenitis IRZE x 2 month
IR, ofloxacin, amikacin x 2 month Clarithromycin + o floxacin มี hepatitis จึง off ยาไป

49
Clinical course Recurrent inquinal lymphadenitis
Biopsy : acute and chronic nongranulomatous inflammation Culture for TB : no growth Culture for bacteria : no growth Culture for fungus : no growth

50
Treatment Infection : systemic antibiotic Prophylaxis of infection :
trimethoprim-sulfamethoxazole Itraconazole Curative treatment : Bone marrow transplantation

51
Prognosis median survival duration : 20-25 years
mortality rate 2 – 3 % per year Cause of death is infection