ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Approach to Pediatric Patients Chaisit Sangtawesin Queen Sirikit National Institute of Child Health

2
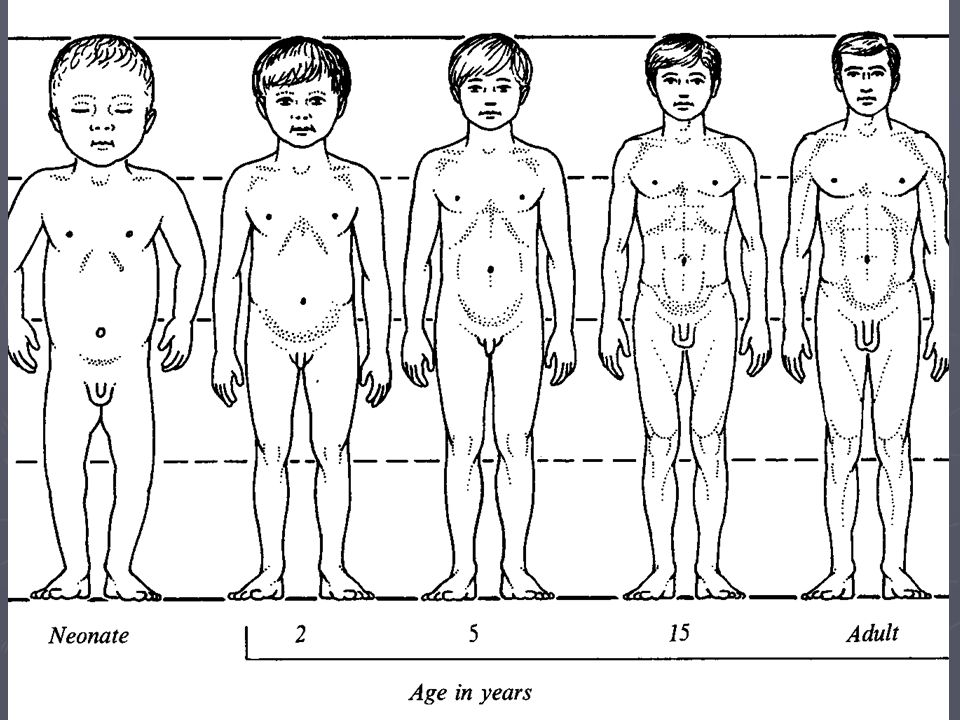
What are the differences between pediatric and adult?

3
► NeonateThe first 4 weeks of life ► InfantThe first year ► Preschool2 - 4+ years ► School age5 – 15 years ► Childhood1 – 15 years ► Adolescent13 – 19 years

4
First of all ► The child should be placed where he wishes. ► The examiner must remain on patient, friendly, tolerant, good-natured and restrained. ► Use soft, persuative voice.

5
หลักในการซักประวัติ ► พยายามลดความกังวล ให้ความสนใจอาการ เจ็บป่วย ► กรณีผู้ป่วยมีอาการหนักก็ควรเริ่มถามเฉพาะ จุดที่สำค้ญและตรวจผู้ป่วย ให้การวินิจฉัย และรีบให้การรักษาเบื้องต้นก่อน แล้วจึง ค่อยเก็บรายละเอียดในภายหลัง ► พยายามเข้าใจ เห็นใจ เป็นกันเอง และ ละ เว้นการวิพากษ์วิจารณ์ ► นึกถึงเด็กด้วยเสมอระหว่างการซักประวัติ ► ต้องเข้าใจว่าเด็กแต่ละวัยมีความแตกต่างกัน เด็กแต่ละวัยมีการรับรู้ ปฏิกิริยาตอบสนอง แตกต่างกันตามวุฒิภาวะ การศึกษา พฤติกรรมและการพัฒนาด้านอารมณ์

6
General inspection ► State of nutrition ► State of activity ► Posture ► Reaction to environment ► Overt deformity ► Relationship to parents ► Conversation ► Injury ► Speech ► Hemorrhage ► Cry ► Facial expression ► Size relative to weight ► Dehydration ► Edema

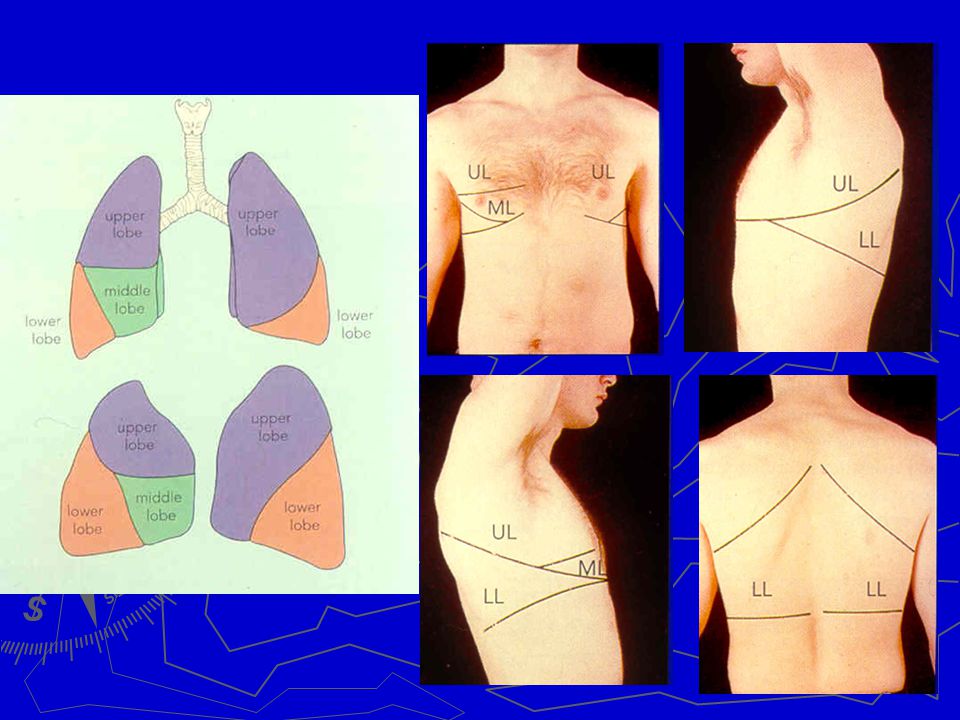
8
General inspection ► Respiratory rate ► Respiratory pattern ► Abnormal sounds during breathing:- hoarseness, wheeze, stridor, whoop, cry ► Abnormal smell ► Abnormal posture ► Emotion ► Mouth breathing ► Jaundice ► Cyanosis ► Characteristic facies ► Rash – color, size, distribution, nature ► Fingers ► Nails

11
Respiratory pattern

12
► Inspiration composes approximately one-third of the respiratory cycle and expiration the remaining two-thirds. ► It is easiest to hear breath sounds during inspiration and expiratory sounds are less well heard. ► The intensity of breath sounds depends on the location of auscultation and on the bodyshape. auscultation and on the bodyshape. ► They are loudest where the large airways are closest to the body surface, and they are more distant in obese individuals body surface, and they are more distant in obese individuals than thin ones. than thin ones. ► They also tend to be louder in children than in adults. NORMALNORMAL BREATH SOUND

13
Bronchial breath sounds Bronchial breath sounds Bronchial breath sounds Bronchial breath sounds ► These sounds are louder than normal breath sounds. ► They are heard when there is consolidation of lung tissue with bronchi that open into the consolidation, such as occurs in pneumonia. ► The consolidation leads to better transmission of sound than when the lungs are filled with air.

14
► Noisy breath sounds produced by the obstruction of the extrathoracic airway. STRIDOR

15
Grunting Grunting ► Grunting is an abnormal breath sound heard during expiration from the closing of the glottis in respiratory distress of a small infant. ► This grunting was recorded with a microphone in front of the mouth of a premature baby girl with respiratory distress 7 hours after birth

16
CREPITATION COARSE CREPITATION FINE CREPITATION

17
Wheezing ► Wheezes are loud sounds that originate in the small airways. ► These sounds have a longer duration than crackles and also have a musical quality. ► They are often detected more easily with forced expiration and are heard in patients with asthma or other obstructive diseases.

19
Respiratory rate Tachypnea Tachypnea ► Neonate – 2 months < 60/min. ► Infancy< 50/min. ► 1-5 years< 40/min. ► Older children< 30/min.

20
Heart rate ► HR < 60/min. is considered to be bradycardia ► HR > 220/min. in infancy or > 180/min. in older children is considered to be tachycardia

21
Blood Pressure

22
5 th Percentile for Blood Pressure ► Neonate60 ► 1 month – 1 year 70 ► 1+ year70 + (2 X age in years)
")
23
Weight ► At birth 3 Kg ► The first 4 monthsBW + (month X 0.8) ► The second 4 monthsBW + (month X 0.7) ► The third 4 monthsBW + (month X 0.6) Infants normally double their birthweight by 5 months and triple their birthweight by 1 year ► Between 1-9 years (4 + years) X 2 ► Between 9-12 yearsYears X 3
 ► The second 4 monthsBW + (month X 0.7) ► The third 4 monthsBW + (month X 0.6) Infants normally double their birthweight by 5 months and triple their birthweight by 1 year ► Between 1-9 years (4 + years) X 2 ► Between 9-12 yearsYears X 3")
24
Length ► At birth 50 cm ► At 6 months65 cm ► At 1 year75 cm ► At 2 years85 cm ► At 3 years95 cm ► At 4 years 100 cm Infants normally double their height by 4 years old ► Over the next 8 years there is an annual increase of 5.5 cm/year

25
female males

27
Upper / Lower segment ► At birth1.7 ► 6 months1.6 ► 15 months1.5 ► 2 years1.4 ► 3 years1.3 ► 5 years1.2 ► Adolescent1

28
Achondroplasia Marfan syndrome

29
Anterior fontanelle Posterior fontanelle Frontal bone Parietal bone Sagittal suture Occipital bone

31
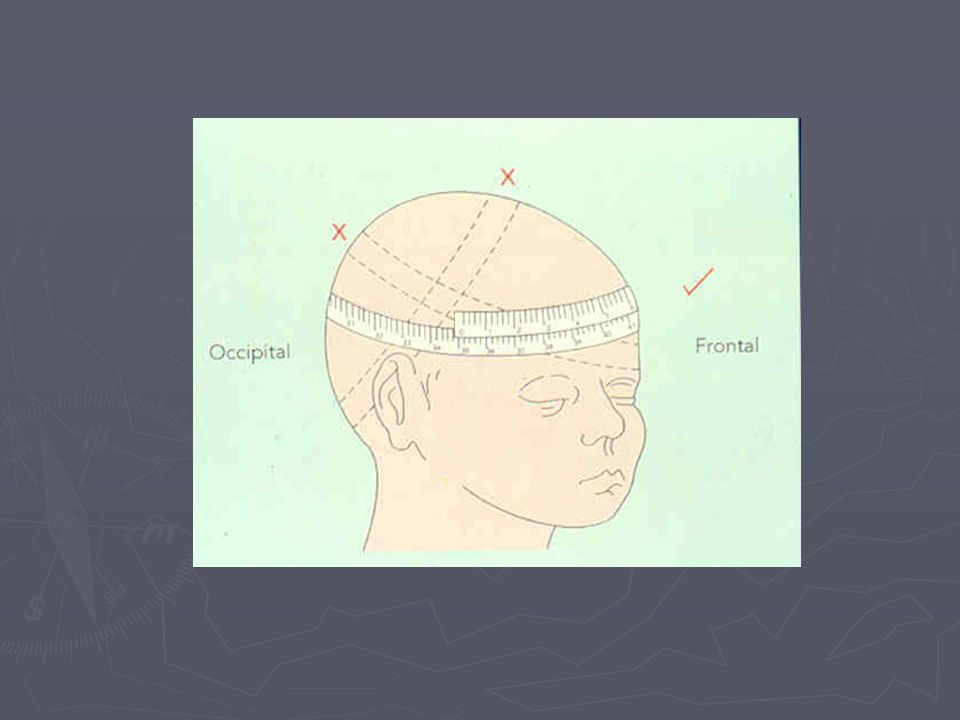
Head circumference ► At birth35 cm ► At 4 months40 cm ► At 1 year45 cm ► At 2 years47 cm ► At 5 years50 cm

33
Dirty white patches over tonsils and posterior pharyngeal wall Diphtheria

34
Milky white patches over tonsils Infectious mononucleosis

35
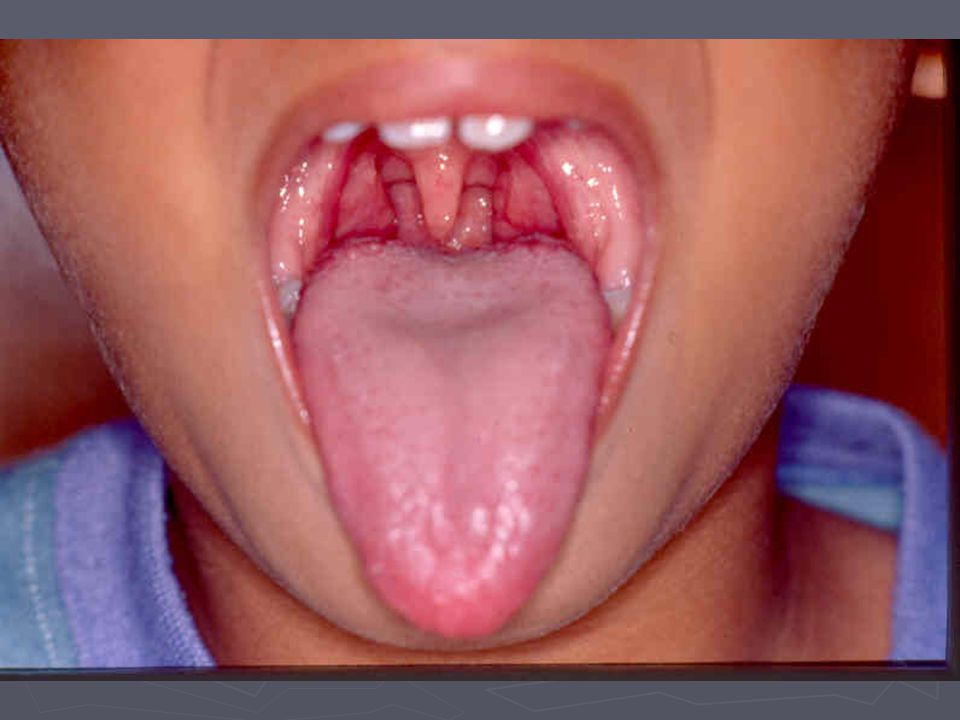
Enlarge and injected tonsils Acute tonsillitis

37
Measles Kopliks’ spots

38
Baby-bottle syndrome

39
Pectus excavatum Pectus carinatum

43
Normal Congenital hip dislocation

44
Barlow Test

45
Ortolani Test

งานนำเสนอที่คล้ายกัน

























>")