ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Hypertension Chorchana Wichian MD.

2
ผู้ป่วย ชาย อายุ 55 ปี โรคประจำตัว โรคความดันโลหิตสูง รักษาไม่สม่ำเสมอ
อาการสำคัญ : แขนขาทางด้านซ้าย อ่อนแรง 2 ชั่วโมงก่อนมาโรงพยาบาล นักเรียน เคยเจอ ผู้ป่วยอย่างนี้ หรือไม่

3
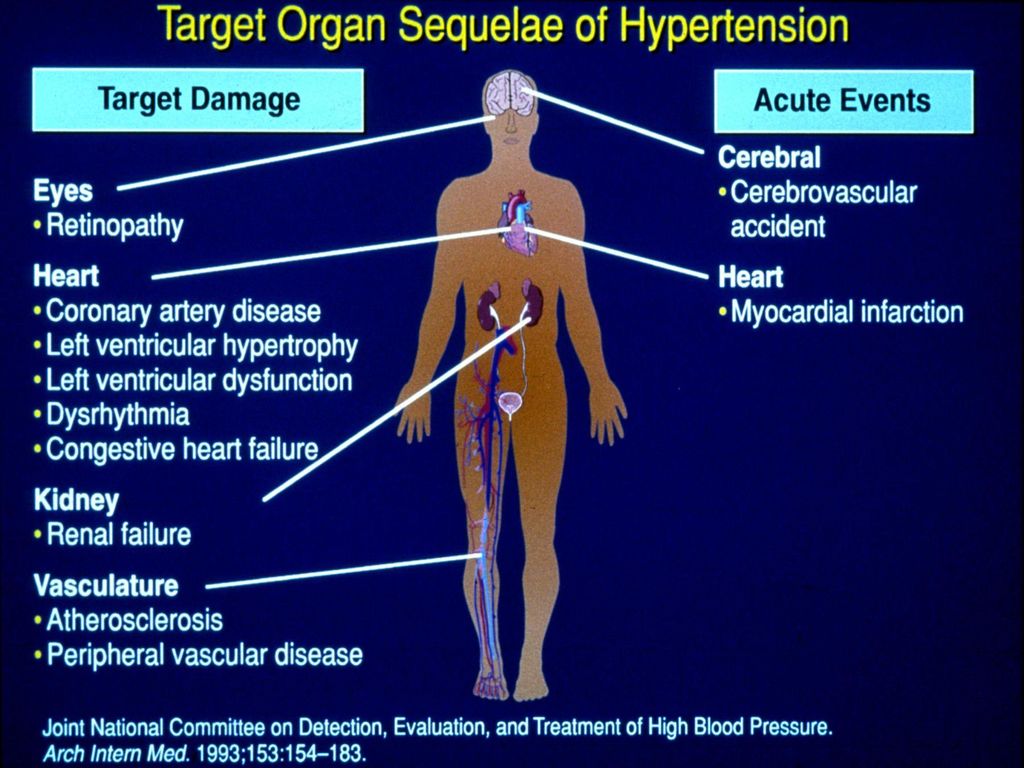
Hypertension Important chronic disease
Leading causes of global burden of disease Doubles the risk of cardiovascular diseases Coronary heart disease Congestive heart failure Ischemic and hemorrhagic stroke Renal failure Peripheral artery disease ความดันโลหิตสูง โรคเรื้อรัง ที่สำคัญ เป็นปัจจัยหลักที่เสี่ยงต่อ โรคหัวใจและหลอดเลือด ทั้งประเทศที่พัฒนาแล้ว และกำลังพัฒนา

4
Epidemiology In the United states , the National Health and nutritional examination survey (NHANES) 1999 – 2000 Approximately 30% of adults have hypertension 33.5 % non Hispanic black 28.9 % non Hispanic white 20.7% Mexican americans 70 % of hypertensive Pt awareness The burden of hypertension increase with age

5
Epidemiology 2nd Thai National Survey 1996 Cases enrolled
7,544 children (<13 yrs) 4,228 working group (13-59 yrs) 4,048 elderly (>60 yrs)
 4,228 working group (13-59 yrs) 4,048 elderly (>60 yrs)")
6
Prevalence of HT = (94+395) x100=11.6% (BP alone)
Prevalence of Hypertension in working group Actual HT No HT 94 395 59 3,683 HT No HT History Prevalence of HT = (94+395) x100=11.6% (BP alone) Prevalence of HT = ( ) x100=12.9% (BP+Hx) 4,228 4,228 2nd National survey of Hypertension ( )
 x100=11.6% (BP alone) Prevalence of HT = ( ) x100=12.9% (BP+Hx) 4,228. 4,228. 2nd National survey of Hypertension ( )")
7
Prevalence of HT = (314+692) x100 =24.8% (BP alone)
Prevalence of Hypertension in elderly Actual HT No HT 314 692 304 2,738 HT No HT History Prevalence of HT = ( ) x100 =24.8% (BP alone) Prevalence of HT = ( ) x100 =32.4% (BP+Hx) 4,048 4,048 2nd National survey of Hypertension ( )
 x100 =24.8% (BP alone) Prevalence of HT = ( ) x100 =32.4% (BP+Hx) 4,048. 4,048. 2nd National survey of Hypertension ( )")
8
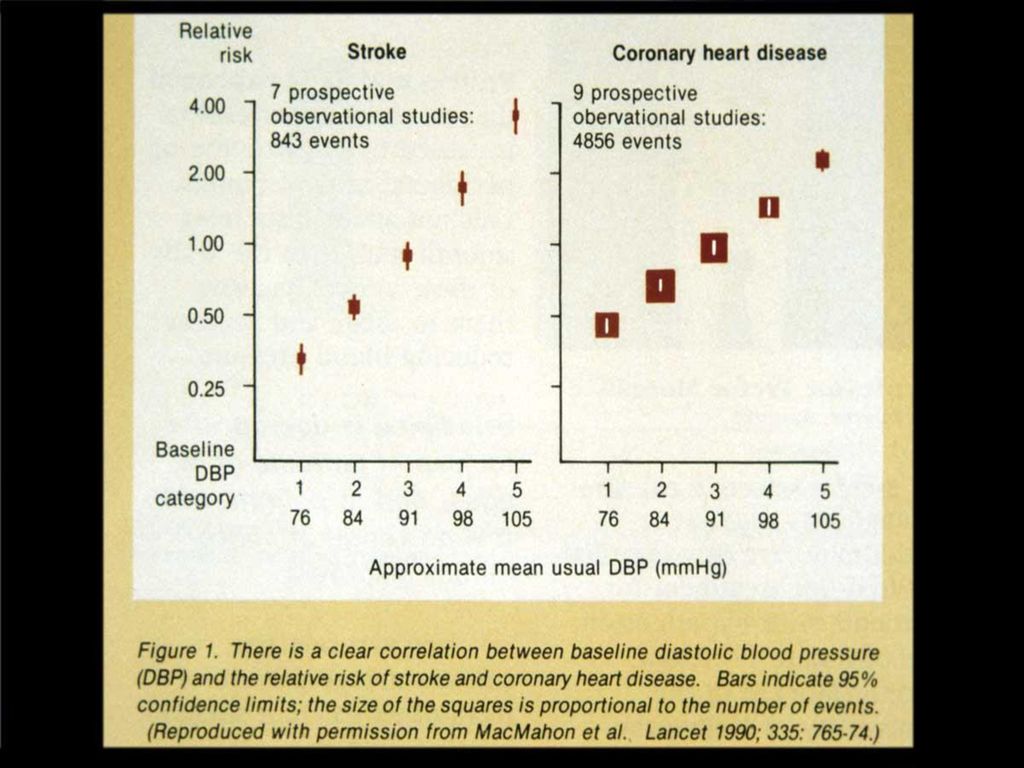
Differing influence of hypertension on
absolute and relative risk of stroke and MI 5 10 15 20 Normotensives Hypertensives 5 Year Risk (%) Stroke Myocardial Infarction ข้อมูลปัจจุบัน พบว่า ผู้ป่วยที่เป็นความดันโลหิตสูง มีดอกาศในการเกิด ภาวะ stroke หรือ MI อย่างชัดเจน 20 40 60 80 100 120 140 160 180 200 220 240 260 280 300 Systolic Blood Pressure (mmHg) Brown, M.J. Lancet 2000; 355: 3
 Stroke. Myocardial. Infarction. ข้อมูลปัจจุบัน พบว่า ผู้ป่วยที่เป็นความดันโลหิตสูง มีดอกาศในการเกิด ภาวะ stroke หรือ MI อย่างชัดเจน Systolic Blood Pressure (mmHg) Brown, M.J. Lancet 2000; 355:")
9
MRFIT Multiple risk factor intervention trial include black white รวมแล้วมากกว่า คนพบว่า ความดันที่เพิ่มขึ้น เพิ่มอัตราการเกิด CHD อย่างชัดเจน

10
Genetic and environmental factor
Obesity and overweight Dietary salt intake Alcohol consumption Low level of physical activtiy Positive family history 3.8 times more frequently ปัจจัย ทางสิ่งแวดล้อมและกรรมพันธ์ อาจทำให้ ความชุกของความดันโลหิตสูงในแต่ละที่ มีความแตกต่างกัน

11
The physiology of normal BP
กลไก การควบคุมความดันโลหิต ขึ้นอยู่กับ cardiac output และ total peripheral resistance เป็นสิ่งสำคัญ

12
The physiology of normal BP
CV กลไก การควบคุมความดันโลหิต ขึ้นอยู่กับ cardiac output และ total peripheral resistance เป็นสิ่งสำคัญ

13
Adrenergic receptor

14
RAS in control of BP RAS system ควบคุม BP โดยทำให้ หลอดเลือด หดตัว โดยผลของ angiotensin II RENIN ที่สร้างจาก JUXTAGLOMERULAR CELL เปลี่ยน AngN > AI AI >AII AII > arteriolar vasoconstriction และ adrenal gland หลั่ง aldosterone

15
RAS in control of BP RAS system ควบคุม BP โดยทำให้ หลอดเลือด หดตัว โดยผลของ angiotensin II RENIN ที่สร้างจาก JUXTAGLOMERULAR CELL เปลี่ยน AngN > AI AI >AII AII > arteriolar vasoconstriction และ adrenal gland หลั่ง aldosterone

16
RAS system ควบคุม BP โดยทำให้ หลอดเลือด หดตัว โดยผลของ angiotensin II
RENIN ที่สร้างจาก JUXTAGLOMERULAR CELL เปลี่ยน AngN > AI AI >AII AII > arteriolar vasoconstriction และ adrenal gland หลั่ง aldosterone

17
RAS system ควบคุม BP โดยทำให้ หลอดเลือด หดตัว โดยผลของ angiotensin II
RENIN ที่สร้างจาก JUXTAGLOMERULAR CELL เปลี่ยน AngN > AI AI >AII AII > arteriolar vasoconstriction และ adrenal gland หลั่ง aldosterone

20
Left Ventricular Hypertrophy

21
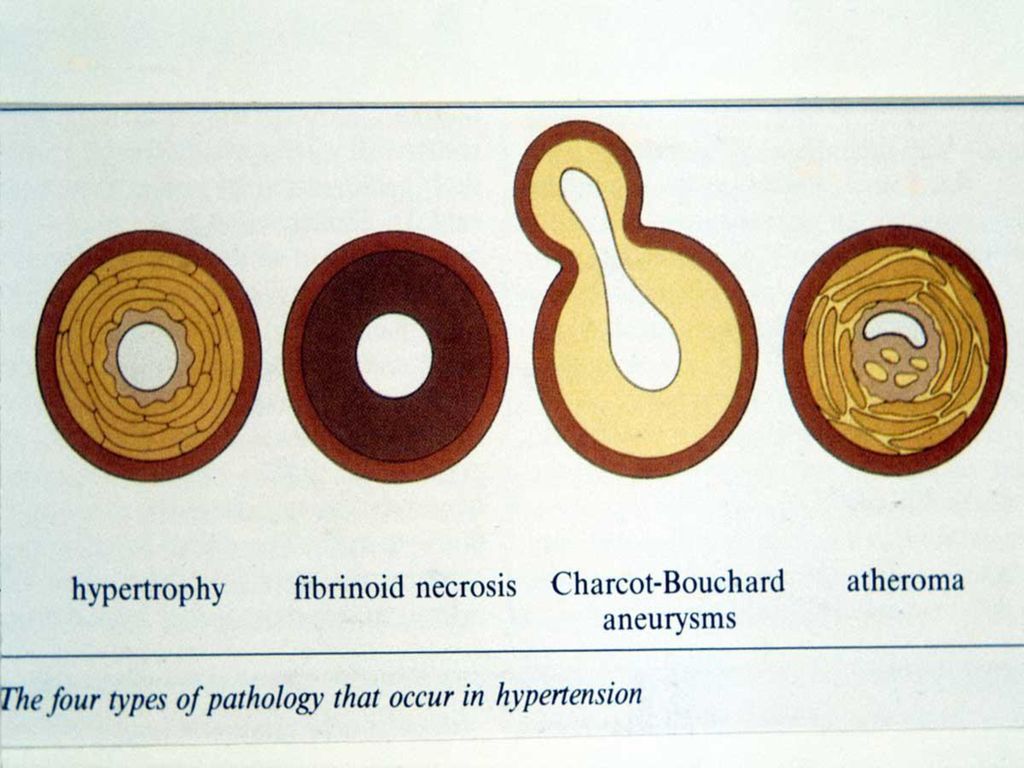
Vascular remodelling ในผู้ป่วย ความดันโลหิตสูง ได้แก่ การลดลงของ lumen ใน small artery และ compliance ที่ลดลง ใน large artery

23
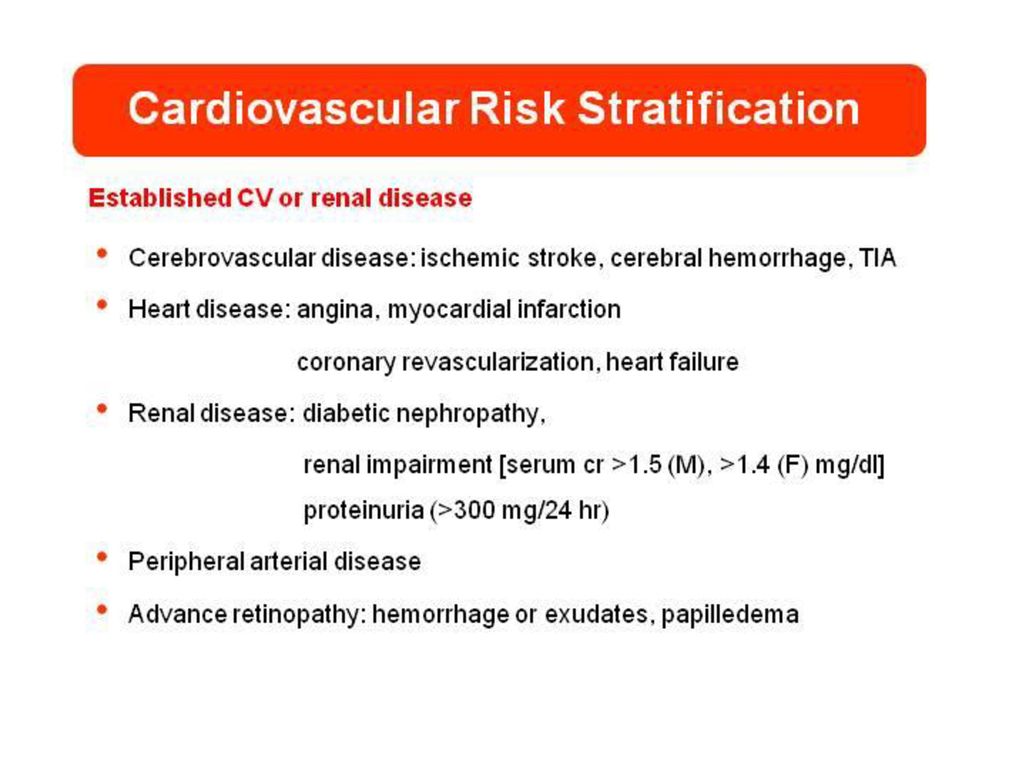
Hypertensive retinopathy
Gr l : arteriolar narrowing Gr ll: copper – wiring/AV nicking Gr lll: hemorrhage and exudate Gr lV: papilledema
24
N Engl J Med 2004;351;2310-7

28
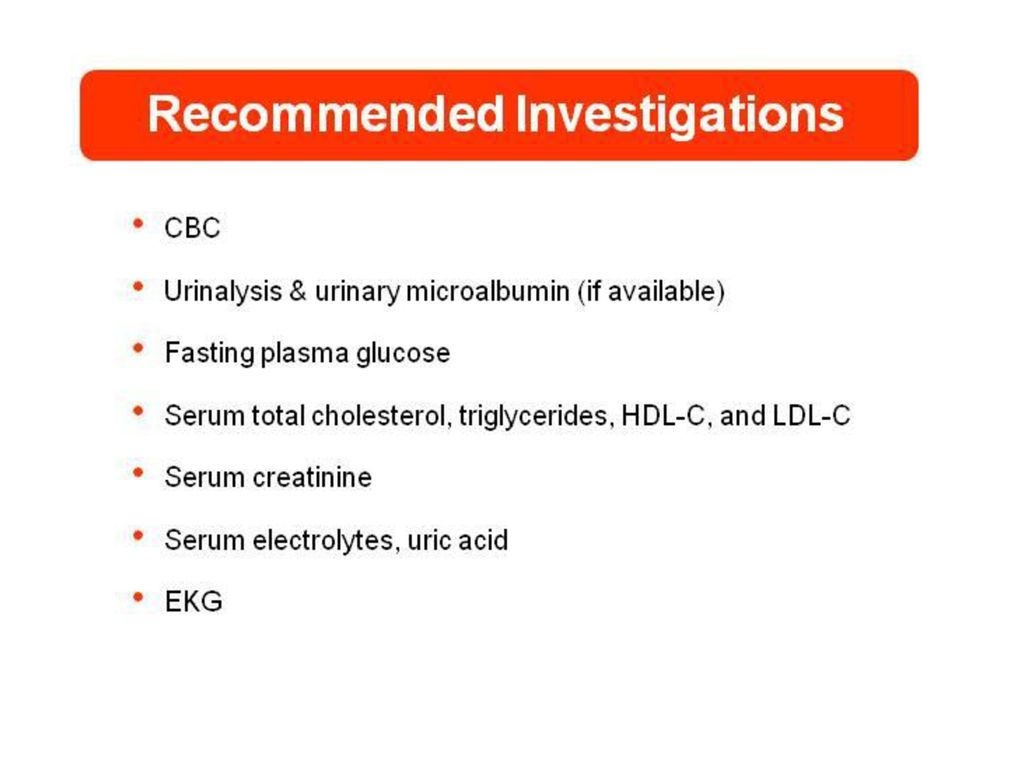
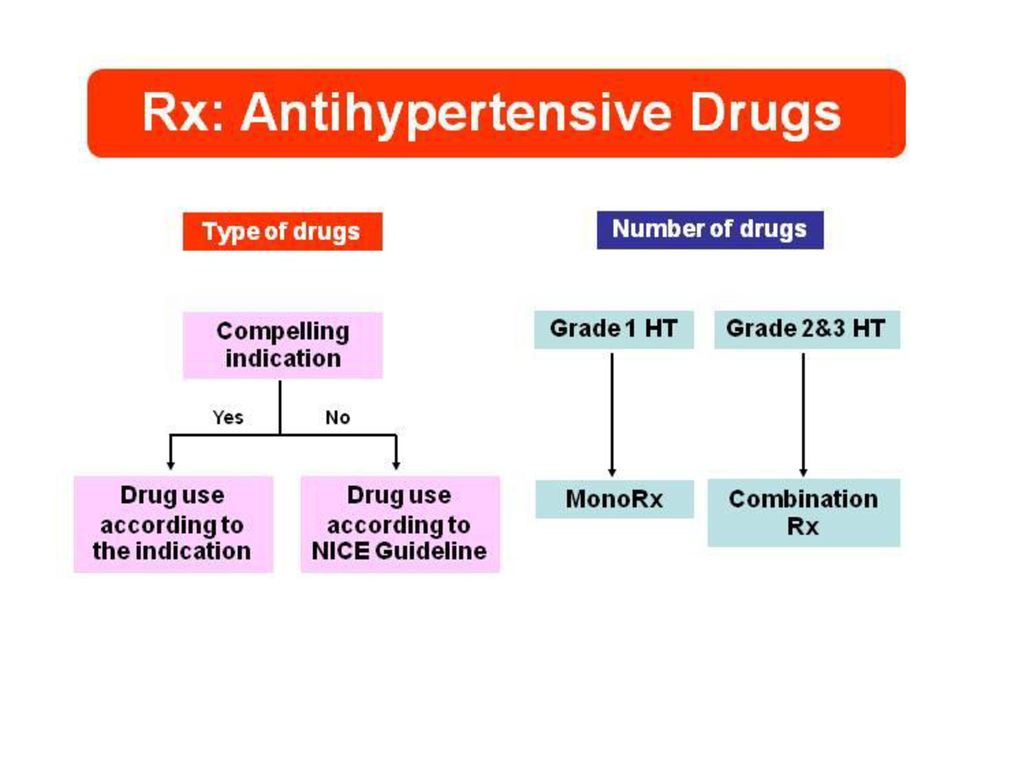
Objective Diagnostic Treatment Follow up

29
Mercury sphygomomanometer ถือว่าเป็น gold standard ในการวัดความดันโลหิต เครื่องอื่นต้องมา เปรียบเทียบ และต้อง calibrate q 6 – 12 เดือน

30
Home BP device British Hypertension Society (BHS)
Home BPควรต้อง เปรียบเทียบ กับ office measurement ในเวลาเดียวกัน อย่ากังวลกับ bp ที่ขึ้น ๆ ลง ควรวัด สองครั้งโดย วันเช้าและเย็น โดยความดันที่จัดว่า เป็นความดันโลหิตสูง คือ มากกว่า 135 และ 85 mmHg ให้หา end target organ damge ร่วมด้วยเสมอ British Hypertension Society (BHS) American Association for the advancement medical Instrument (AAMI)
 American Association for the advancement medical Instrument (AAMI)")
31
24 hr ambulatory BP monitoring
ยืนยันการวินิจฉัย ติดตามการรักษา การควบคุมความดันโลหิตของยา การวินิจฉัยภาวะดื้อต่อยาความดันโลหิต ความสัมพันธ์ของยา กับผลที่ไม่พึงประสงค์ ของยา

32
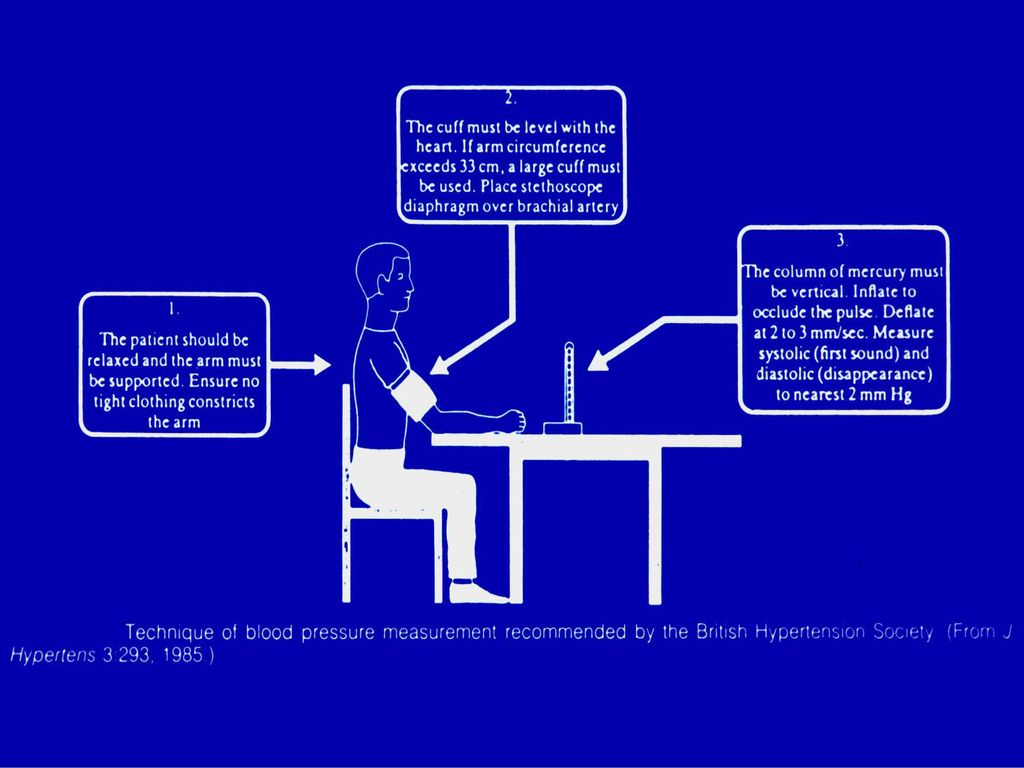
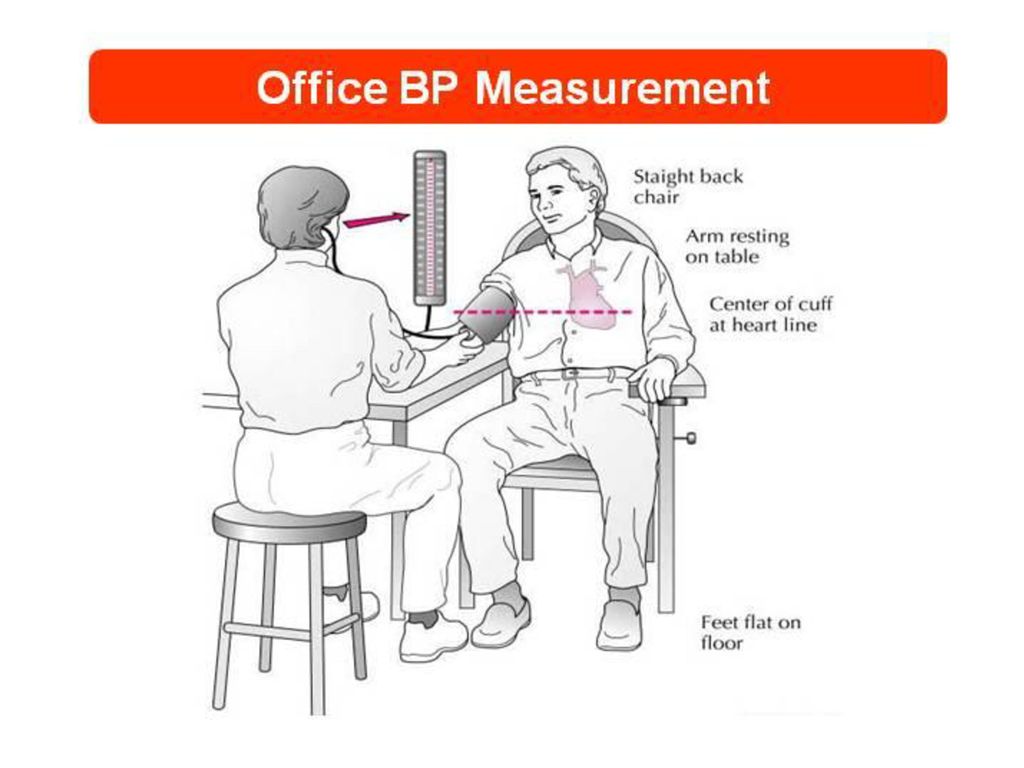
BP should be measured several times on several
BP measurements BP should be measured several times on several occasions with the patient in a sitting position 1. Allow the patient to sit for several minutes 2. Use a cuff with a bladder of cm x 35 cm, with larger bladder for fat arms 3. Use phase 5 Korotkoff sounds to measure DBP 4. Measure the BP in both arms at first visit 5. Measure standing BP in the elderly and diabetic patients. 6. Place the cuff at heart level, whatever the position of the patient Cuff ที่เป็น bladder อย่างร้อยละ 80% ของเส้นรอบวงต้นแขน และ ความกว้าง คลอบคลุมประมาณ 2/3 ของความยาวต้นแขน เครื่องหมาย ที่ brachial artery และขอบล่างอยู่เหนือ cuff 2.5 cm

33
Recommended cuff-width for children
and obese adults Under one year cm 1-3 years cm 4-8 years cm Average adults cm Obese adults cm

36
Koratkoff sound 5 phase phase 1 systolic phase 5 diastolic

37
Isolated office (‘white-coat’) hypertension
In some patients, office blood pressure is persistently elevated whereas daytime blood pressure outside the clinic environment is not Office BP ≥ 140/90 mmHg Out of office BP < 135/85 mmHg White coat hypertension เป็นภาวะ ที่ความดันโลหิต ขึ้นจากผู้ป่วยมีภาวะตื่นตัว (white coat effect) ซึ่งปฏิกิริยา ที่เกิดขึ้นสั้น ๆ ในผู้ส่วนใหญ่ ขึ้นอยู่กับ ปัจจัย สองอย่าง คือ สภาพแวดล้อม และผู้ทำการวัดความดันโลหิต White-coat 1. WHO/ISH 1999.
 ซึ่งปฏิกิริยา ที่เกิดขึ้นสั้น ๆ ในผู้ส่วนใหญ่ ขึ้นอยู่กับ ปัจจัย สองอย่าง คือ สภาพแวดล้อม และผู้ทำการวัดความดันโลหิต. White-coat 1. WHO/ISH")
38
Hypertension Primary or essential hypertension Secondary hypertension

39
Definition ข้อมูล พบว่า ระดับ ของ SBP ที่เพิ่มสูงขึ้น 20 DBP > 10 ทำให้ เพิ่ม risk ของ cardiovascular risk 2 เท่า

40
Essential hypertension Secondary hypertension
Classification Primary hypertension Essential hypertension Secondary hypertension ข้อมูล พบว่า ระดับ ของ SBP ที่เพิ่มสูงขึ้น 20 DBP > 10 ทำให้ เพิ่ม risk ของ cardiovascular risk 2 เท่า

41
Features of “Inappropriate” Hypertension
Onset before 20 or after 50 years of age Level of blood pressure > 180/110 mmHg Organ damage : - - Fundoscopic findings of grade 2 or higher - Serum creatinine > 1.5 mg/100 mL - Cardiomegaly or left ventricular hypertrophy Features indicative of secondary causes - Unprovoked hypokalemia - Abdominal bruit - Variable pressure with tacycardia, sweating, tremor - Family history of renal disease Poor response therapy that is usually effective Braundwald’s Heart disease 7th ed. 2005

42
Drugs Sleep apnea,tumor Endocrine: 0.5% 5-10% Renal : 4% Coarc: 0.2%

47
Figure “3” sign Rib notching

59
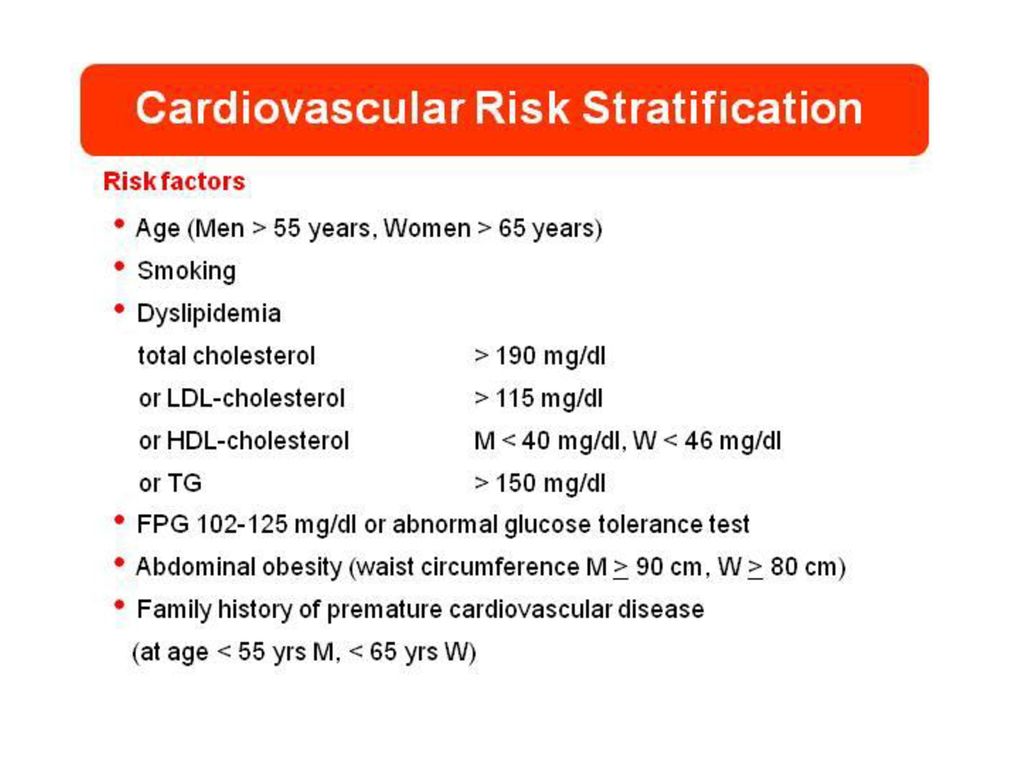
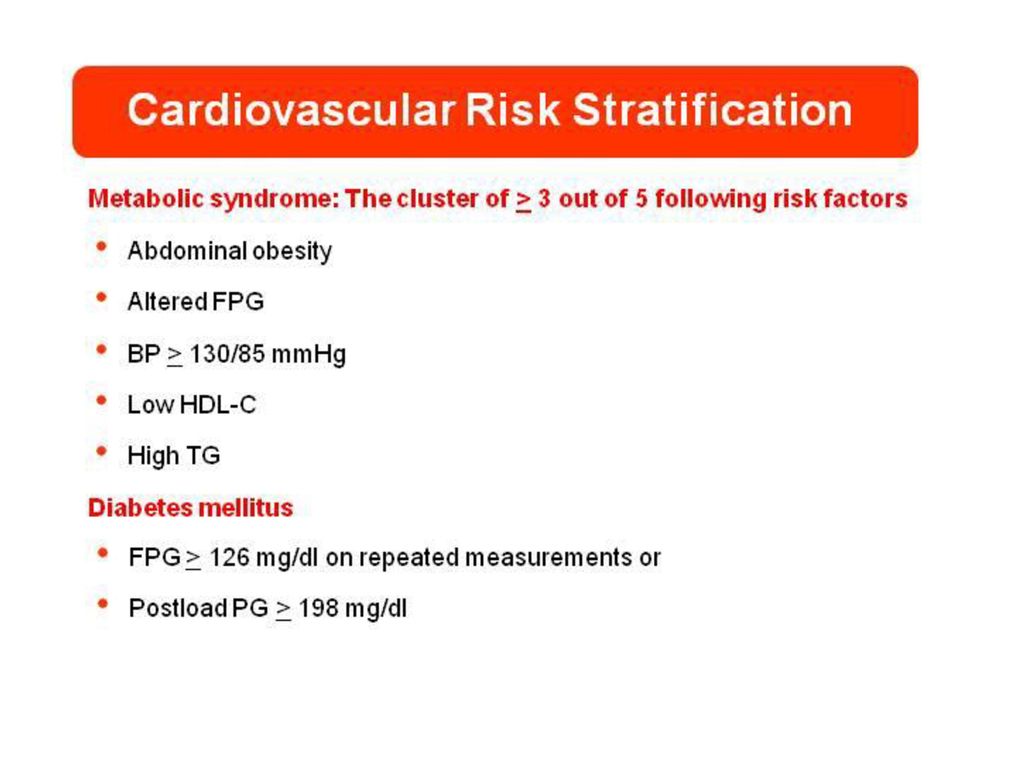
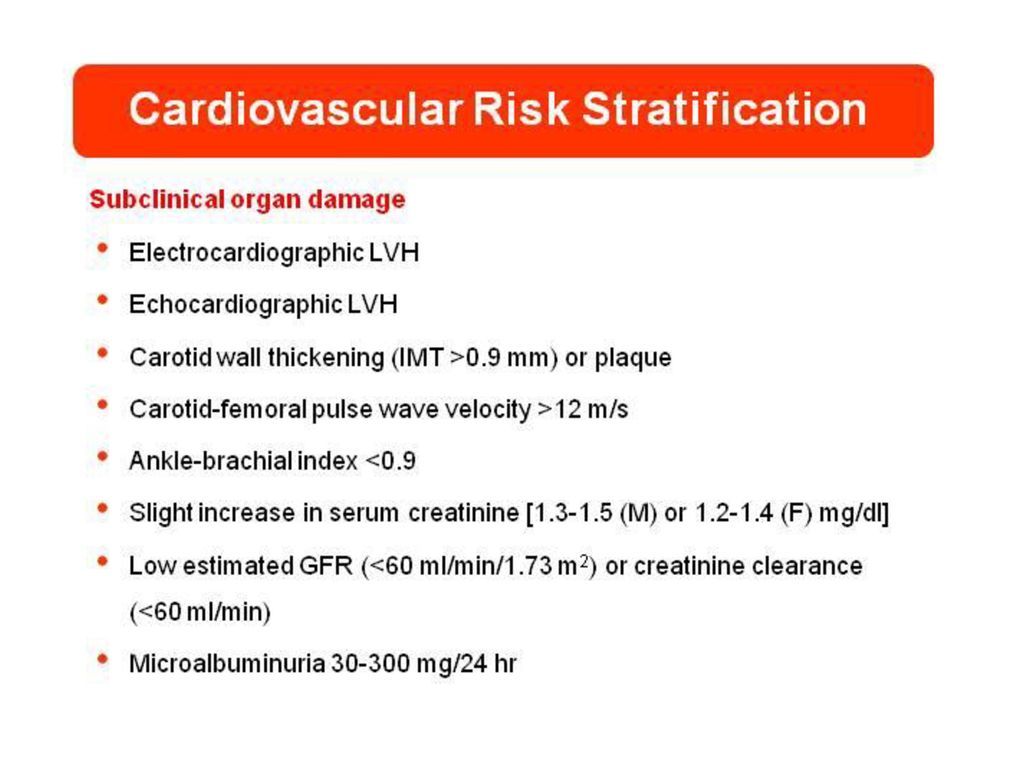
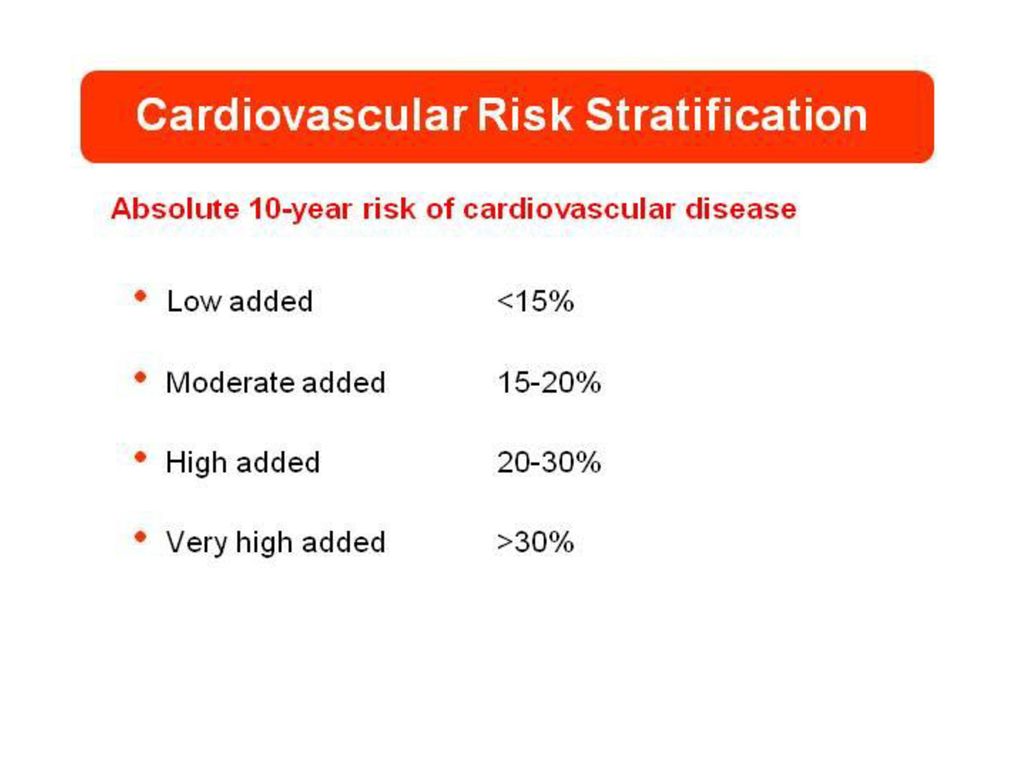
การพยากรณ์โรค ถึงปัจจัยเสี่ยง ในการเกิดโรคหลอดเลือดและหัวใจในอนาคตที่แตกต่างกัน

68
Diuretics b-receptor Angiotensin receptor antagonists a-receptor
Calcium antagonists ACE inhibitors Possible combinations of different classes of antihypertensive agents. Among calcium antagonists, only dihydropyridines can associated with betablockers. ACE, angiotensin-converting enzyme. The most rational combinations are represented as thick lines. 2003 ESH/ESC Hypertension Guidelines

69
2007 ESH/ESC Hypertension Guidelines

70
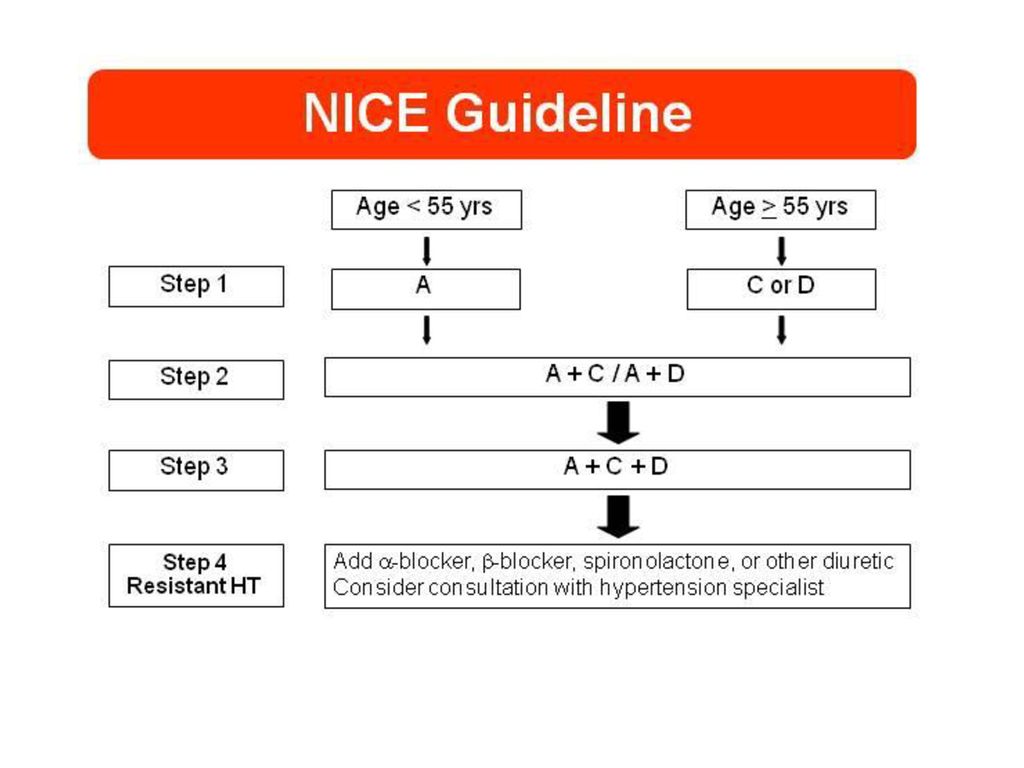
แนวทางเวชปฏิบัติ ความดันโลหิตสูงประเทศไทย 2555

74
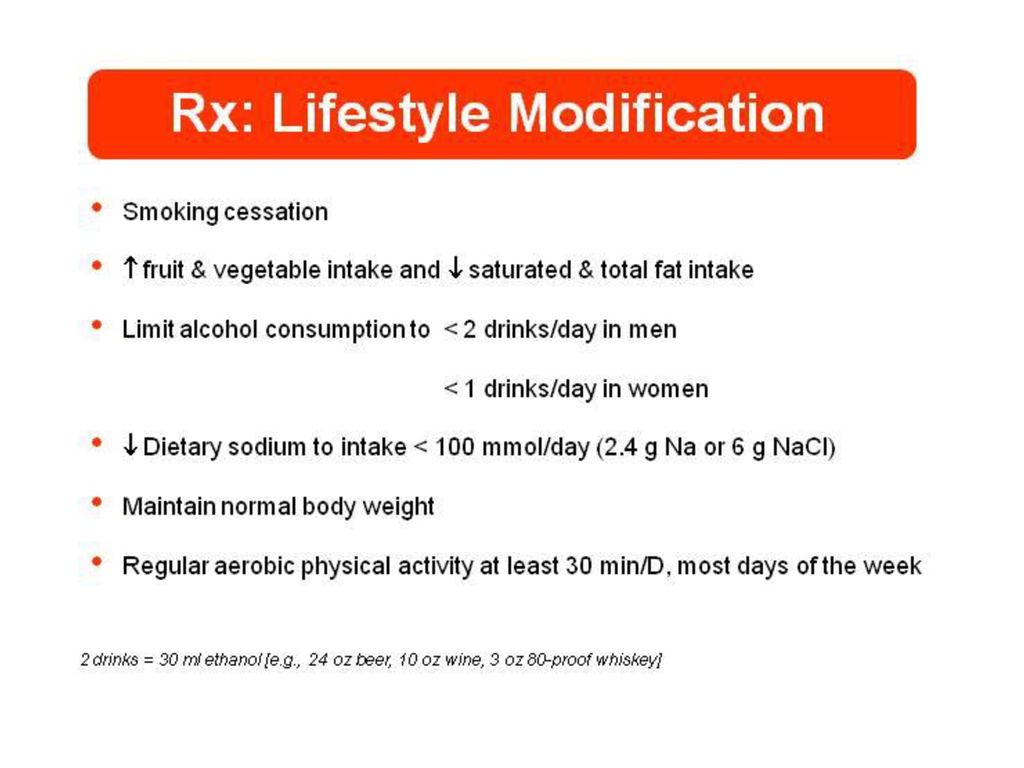
คำแนะนำผู้ป่วย การปรับเปลี่ยนวิถีการดำรงชีวิต ที่มีการยอมรับชัดเจน
การหยุดสูบบุหรี่ การดื่มแอลกอฮอล์ในระดับปานกลาง ไม่เกิน 20 – 30 กรัมต่อวัน การบริโภคอาหาร DASH อาหารกลุ่มผัก ผลไม้ นมไขมันต่ำ ลดปริมาณไขมันอิ่มตัว ไขมันรวม ลดน้ำหนัก ควบคุมน้ำหนักให้ BMI 18.5 – 24.9 kg/m2 ควบคุมระดับ โซเดียมให้ต่ำกว่า 100 มิลลิโมลต่อวัน ( 2.4 g sodium) ระดับออกกำลังกาย 30 นาทีต่อวัน อย่างน้อย 4 วันต่อสัปดาห์
 ระดับออกกำลังกาย 30 นาทีต่อวัน อย่างน้อย 4 วันต่อสัปดาห์")
75
คำแนะนำผู้ป่วย Alcohol raises blood pressure and can harm liver, brain, and heart What counts as a drink? 12 oz beer 5 oz of wine 1.5 oz of 80 proof whiskey

76
คำแนะนำผู้ป่วย

77
คำแนะนำผู้ป่วย

78
Thank you

งานนำเสนอที่คล้ายกัน



















 23-24 กุมภาพันธ์ 2558 สำนักงานสาธารณสุข จังหวัดบุรีรัมย์>")