ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

2
Drug-induced Kidney Stone

3
ความสำคัญของโรค - โรคไต (kidney stone-obstructive nephropathy) รองจากเบาหวานและความดันโลหิต -99.25/100,000 พ. ศ.2550 -122.46/100,000 พ. ศ.2553 - ชาย > หญิง -40-50 ปี - เหนือ / ตะวันออกเฉียงเหนือ

4
อาการ -colicky pain -bilateral obstruction -metabolic acidosis

5
ชนิด ก้อนนิ่ว 2 องค์ประกอบ 1-mineral composition(ca oxalate phosphate and uric acid) 2 -organic matrix(protein carbohydrate lipid) พบบ่อย 1.calium oxalate stone 75-80 % 2.struvite stone 15 % 3.uric acid stone 6 %
 2 -organic matrix(protein carbohydrate lipid) พบบ่อย 1.calium oxalate stone % 2.struvite stone 15 % 3.uric acid stone 6 %")
6
ปัจจัยเสี่ยง - สารก่อนิ่ว / สารยับยั้งนิ่ว (citrate potassium and magnesium) - ยาหรือเมตาบอไลต์ ขับออกทางไตสูง / ละลาย น้ำน้อย - นิ่วที่เกิดจากยาร้อยละ 1-2%. ยาทำให้เกิดส่วนประกอบของนิ่ว. ยาหรือเมตาบอไลต์ทำให้เกิด crytal และ ตกตะกอน

7
ตัวอย่างยาเกิดโรคนิ่วในไต นิ่วแคลเซียม -antacid -acetazolamide -glucocorticoids -theophyline -vitamin D และ vitamin C

8
นิ่วกรดยูริก -thiazides -salicylates -probenecid -allopurinol

9
นิ่วคริสตัลและตกตะกอน -acyclovir- ขนาดยาสูง / เร็ว / ขาดสารน้ำ //euvolemia -sulfonamide antibiotics- ปัสสาวะกรด / ขนาดยาสูง / ไตบกพร่อง / อัลบูมินต่ำ //euvolemia, ปัสสาวะ >7.5 -ethylene glycol -megadose vitamin c -methotrexate- ขนาดสูง /ph<7.0 กรด / ขาดสารน้ำ / ไต -protease inhibitors-indinavir – ปัสสาวะด่าง / ขาด สารน้ำ // ดื่มน้ำ 1.5 ลิตร / วัน ติดตามไต 2 ครั้ง / ปี

10
ภก. นิรุตน์ ศิริพันธุ์พรชนะ

11
การวินิจฉัยปอดอักเสบจาก เชื้อในชุมชน Clinical presentation Chest x-ray, CXR

12
การวินิจฉัยปอดอักเสบจาก เชื้อในชุมชน การปันทึกภาพทรวงอกด้วยคลื่นเสียงความถี่สูง (Chest ultrasonography, CUS) การศึกษาของ Taghisadieh และคณะ, 2015 - Chest x-ray, CXR - Chest ultrasonography, CUS Update!
 การศึกษาของ Taghisadieh และคณะ, Chest x-ray, CXR - Chest ultrasonography, CUS Update!")
13
การจัดกลุ่มความรุนแรงของ โรคและโอกาสเสียชีวิต Pneumonia Severity Index (PSI) CURB - 65 Procalcitonin (PCT) The National Early Warning Score-Lactate (NEWS-L)
 CURB - 65 Procalcitonin (PCT) The National Early Warning Score-Lactate (NEWS-L)")
14
การจัดกลุ่มความรุนแรงของ โรคและโอกาสเสียชีวิต

15
Confusion, Disorientation BUN > 7 mmol/l Respiratory Rate > 30 bpm BP ≤ 90/60 Age ≥ 65 Outpatient (0.7-2.1%) Inpatient (9.2%) ICU (15-40%)
 Inpatient (9.2%) ICU (15-40%)")
16
การจัดกลุ่มความรุนแรงของ โรคและโอกาสเสียชีวิต Procalcitonin (PCT) การศึกษาแบบ meta-analysis, 2016 - ค่า PCT ที่เพิ่มขึ้นเป็นปัจจัยเสี่ยงต่อการเสียชีวิต ( RR 4.18, 95%CI 3.19- 5.48, p= 0.046) Update!
 การศึกษาแบบ meta-analysis, ค่า PCT ที่เพิ่มขึ้นเป็นปัจจัยเสี่ยงต่อการเสียชีวิต ( RR 4.18, 95%CI , p= 0.046) Update!")
17
การจัดกลุ่มความรุนแรงของ โรคและโอกาสเสียชีวิต NEWS-L อัตราการเสียชีวิต ≤ 32.2 3.1-5.27.9 5.3-89.6 ≥ 623.9 Update!

18
การรักษาเพื่อลดอัตราการ เสียชีวิต การศึกษาแบบ cohort โดย Daniel และคณะ ปี 2016 ผู้ป่วยได้รับยาต้านจุลชีพภายใน 4 ชั่วโมงมีอัตราการเสียชีวิตภายใน 30 วัน (Adjusted 30-day inpatient mortality) ตำกว่าอย่างมีนัยสำคัญทางสถิติ OR 0.84, 95%CI 0.74-0.94, p<0.003)
 ตำกว่าอย่างมีนัยสำคัญทางสถิติ OR 0.84, 95%CI , p<0.003)")
19
การเปลี่ยนยาต้านจุลชีพชนิดหยด เข้าหลอดเลือดดำ เป็นชนิดรับประทาน Respiratory Rate < 25 bpm Oxygen saturation > 90% OR arterial oxygen partial pressure > 55 mmHg Hemodynamics stable Temperature decrease > 1 ◦ C Normal mental confusion Ability to maintain oral intake

20
การให้ยา Corticosteroids ร่วมด้วย การศึกษาแบบ systematic review และ meta-analysis ของ Marti และ คณะ ผู้ป่วยได้รับ Corticosteroid 14-420 mg ของ Methylprednisolone อัตราการเสียชีวิตต่ำกว่า (RR 0.84, 95%CI 0.55-1.29, p= 0.429) ภาวะแทรกซ้อนรุนแรง (RR 0.36, 95%CI 0.23-0.56, p<0.0001) ระยะเวลาในการนอน รพ. สั้นกว่า

21
การให้วัคซีน Pneumococcal Polysaccharide-based [23-valent pneumococcal polysaccharide vaccine, PS-23] ; Pneumo-23 ®, Pneumovax ® Conjugate-based [pneumococcal conjugate vaccine, PCV] ; Prevnar 13 ®, Synflorix ® 10
![การให้วัคซีน Pneumococcal Polysaccharide-based [23-valent pneumococcal polysaccharide vaccine, PS-23] ; Pneumo-23 ®, Pneumovax ® Conjugate-based [pneumococcal conjugate vaccine, PCV] ; Prevnar 13 ®, Synflorix ® 10](http://images.slideplayer.in.th/42/11448519/slides/slide_21.jpg "การให้วัคซีน Pneumococcal Polysaccharide-based [23-valent pneumococcal polysaccharide vaccine, PS-23] ; Pneumo-23 ®, Pneumovax ® Conjugate-based [pneumococcal conjugate vaccine, PCV] ; Prevnar 13 ®, Synflorix ® 10")
22
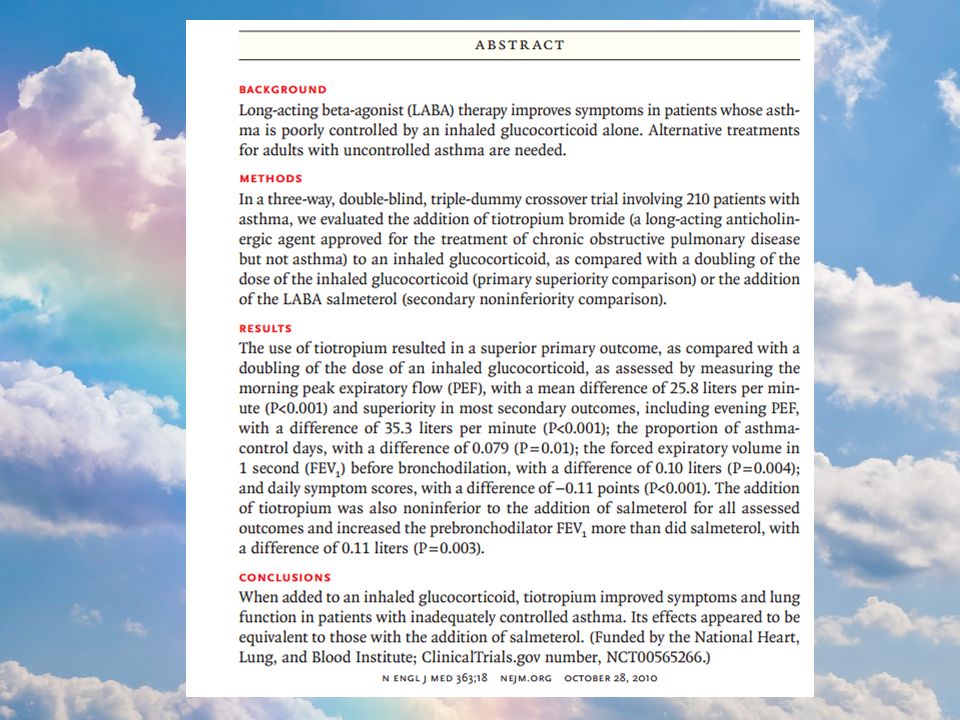
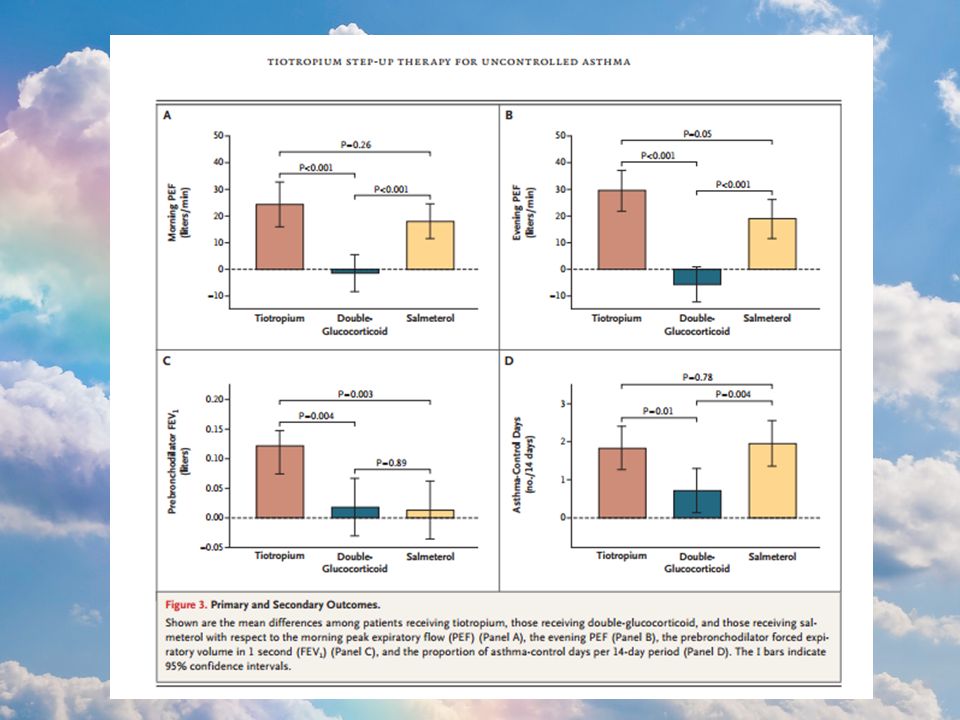
Current Role of Long-Anticholinergic in asthma? Pharmacotherapy of interesting common disease 2016 Angvara L.

23
การให้วัคซีน Pneumococcal Advisory Committee on Immunization Practices (ACIP), 2015 PCV13 ผู้ที่มีอายุ ≥65 ปี ที่ ไม่เคยได้รับวัคซีน มาก่อน PPSV23 ผู้ที่มีอายุ ≥65 ปี ที่ เคยได้ ppsv23 > 1 ครั้ง PPSV23 PCV 13
, 2015 PCV13 ผู้ที่มีอายุ ≥65 ปี ที่ ไม่เคยได้รับวัคซีน มาก่อน PPSV23 ผู้ที่มีอายุ ≥65 ปี ที่ เคยได้ ppsv23 > 1 ครั้ง PPSV23 PCV 13")
24
GOLD 2015 Guideline

25
Pathophysiology of Asthma Medications for Asthma GINA’s recommendation Mechanism of action? Short and Long acting anticholinergic Comparative Study, Clinical outcomes Current Role of Long-Anticholinergic in asthma?

26
PATHOPHYSIOLOGY

27
TYPICAL SYMPTOMS OF ASTHMA More than 1 symptom Symptoms often worse at night or in early morning. Symptoms vary over time and in intensity. Can triggered by viral infections, exercise, allergen exposure and other More than 1 symptom Symptoms often worse at night or in early morning. Symptoms vary over time and in intensity. Can triggered by viral infections, exercise, allergen exposure and other

28
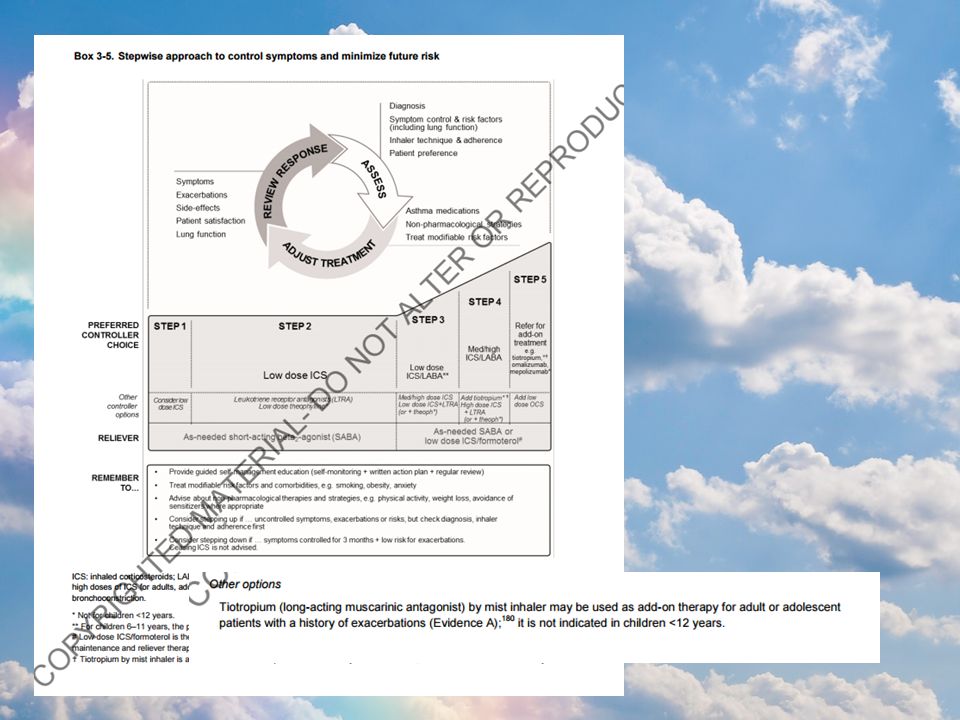
© Global Initiative for Asthma Stepwise approach to control asthma symptoms and reduce risk GINA 2015, Box 3-5 (1/8) Symptoms Exacerbations Side-effects Patient satisfaction Lung function Other controller options RELIEVER REMEMBER TO... Provide guided self-management education (self-monitoring + written action plan + regular review) Treat modifiable risk factors and comorbidities, e.g. smoking, obesity, anxiety Advise about non-pharmacological therapies and strategies e.g. physical activity, weight loss, avoidance of sensitizers where appropriate Consider stepping up if … uncontrolled symptoms, exacerbations or risks, but check diagnosis, inhaler technique and adherence first Consider stepping down if … symptoms controlled for 3 months + low risk for exacerbations. Ceasing ICS is not advised. STEP 1STEP 2 STEP 3 STEP 4 STEP 5 Low dose ICS Consider low dose ICS Leukotriene receptor antagonists (LTRA) Low dose theophylline* Med/high dose ICS Low dose ICS+LTRA (or + theoph*) As-needed short-acting beta 2 -agonist (SABA) As-needed SABA or low dose ICS/formoterol** Low dose ICS/LABA* Med/high ICS/LABA Refer for add-on treatment e.g. anti-IgE Diagnosis Symptom control & risk factors (including lung function) Inhaler technique & adherence Patient preference Asthma medications Non-pharmacological strategies Treat modifiable risk factors PREFERRED CONTROLLER CHOICE Add tiotropium# High dose ICS + LTRA (or + theoph*) Add tiotropium# Add low dose OCS
 Treat modifiable risk factors and comorbidities, e.g. smoking, obesity, anxiety Advise about non-pharmacological therapies and strategies e.g. physical activity, weight loss, avoidance of sensitizers where appropriate Consider stepping up if … uncontrolled symptoms, exacerbations or risks, but check diagnosis, inhaler technique and adherence first Consider stepping down if … symptoms controlled for 3 months + low risk for exacerbations. Ceasing ICS is not advised. STEP 1STEP 2 STEP 3 STEP 4 STEP 5 Low dose ICS Consider low dose ICS Leukotriene receptor antagonists (LTRA) Low dose theophylline* Med/high dose ICS Low dose ICS+LTRA (or + theoph*) As-needed short-acting beta 2 -agonist (SABA) As-needed SABA or low dose ICS/formoterol** Low dose ICS/LABA* Med/high ICS/LABA Refer for add-on treatment e.g. anti-IgE Diagnosis Symptom control & risk factors (including lung function) Inhaler technique & adherence Patient preference Asthma medications Non-pharmacological strategies Treat modifiable risk factors PREFERRED CONTROLLER CHOICE Add tiotropium# High dose ICS + LTRA (or + theoph*) Add tiotropium# Add low dose OCS.")
29
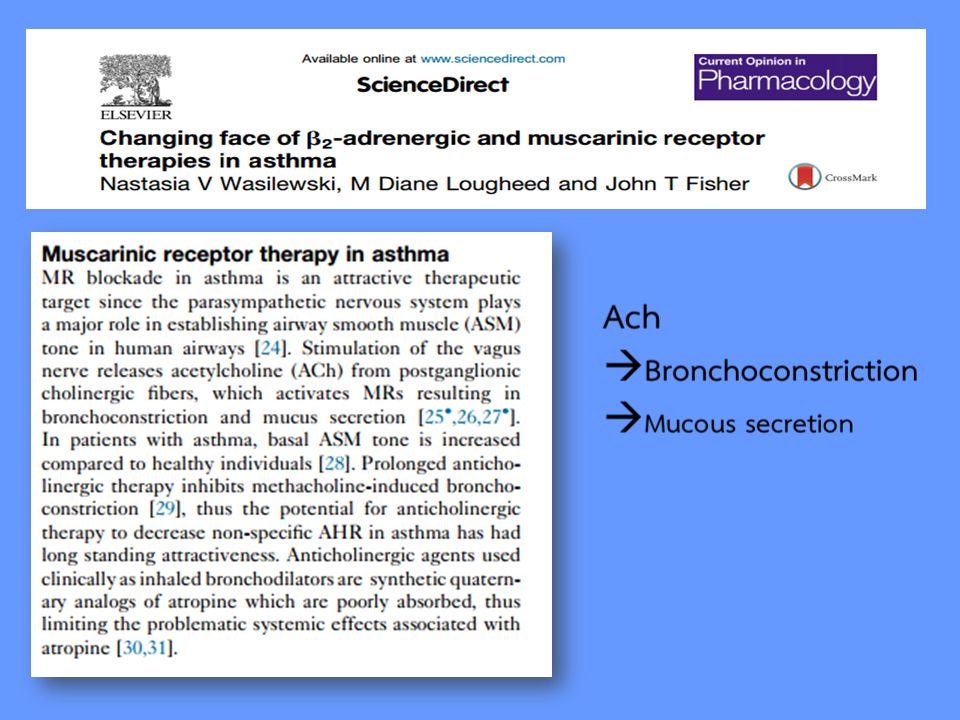
Cholinergic parasympathetic system Ach Adrenaline

31
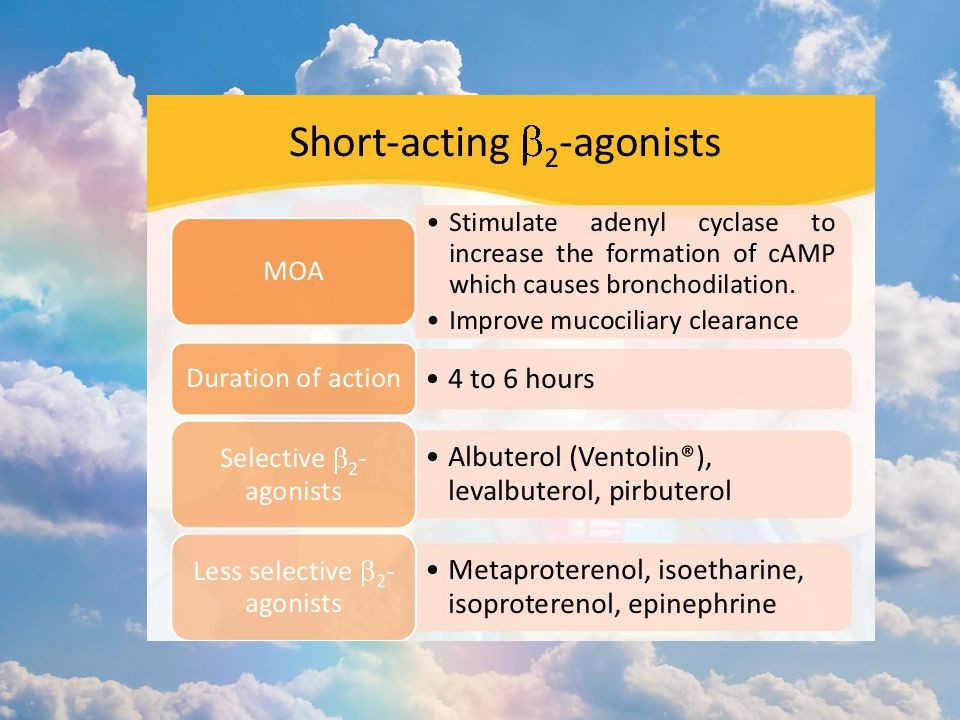
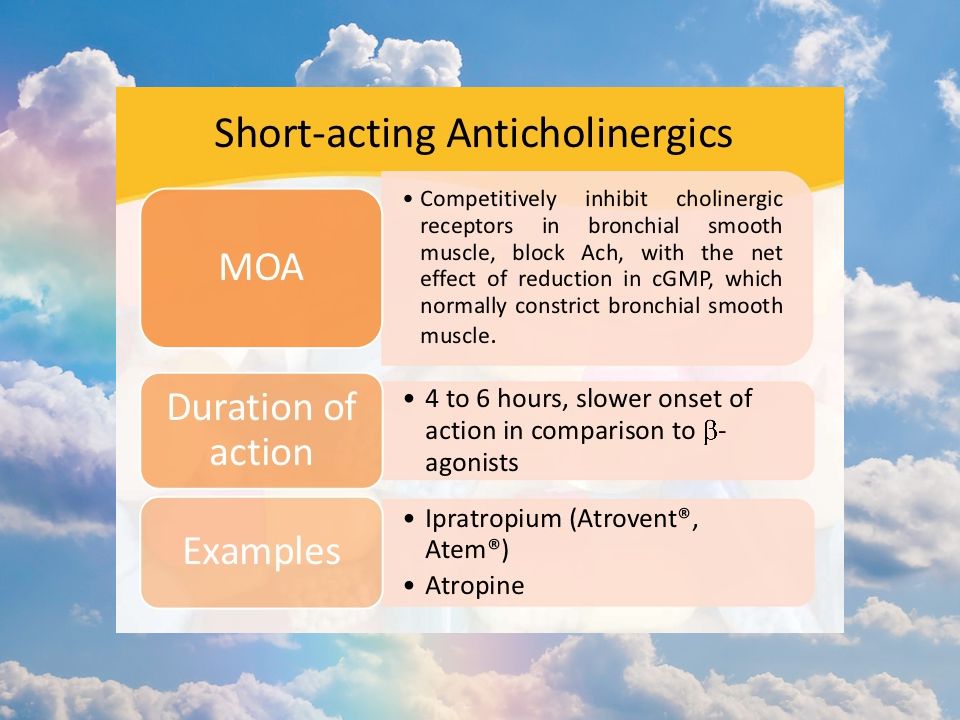
Reliever treatment SAMAs ; Alternative reliever in Pt.with S/E of SABAs ; Not effective as LABAs ; In children long term therapy not recommended for chronic asthma. ; Onset of action

32
Anticholinergics use

33
Tiotropium & Airway Remodellin g airway remodelling in animals model in asthma. mucous membrane hypertrophy ASM thickening

38
ROLE OF TIOTROPIUM IN ASTHMA

40
What is the role of Anticholinergic in asthma? Medications for Asthma. GINA’ recommendation Mechanism of action? Short and Long acting anticholinergic Comparative Study, Clinical outcomes

48
STEP 4 * Two or more controllers plus as- needed reliever medication Preferred option (adults/adolescents): -combination low dose ICS/formoterol as maintenance and reliever treatment, -OR combination medium dose ICS/LABA plus as-needed SABA Tiotropium (long-acting muscarinic antagonist) by mist inhaler may be used as add-on therapy for adult or adolescent patients with a history of exacerbations (Evidence A);180 it is not indicated in children
: -combination low dose ICS/formoterol as maintenance and reliever treatment, -OR combination medium dose ICS/LABA plus as-needed SABA Tiotropium (long-acting muscarinic antagonist) by mist inhaler may be used as add-on therapy for adult or adolescent patients with a history of exacerbations (Evidence A);180 it is not indicated in children")
49
* Higher level care and/or add-on treatment Preferred option: referral for specialist investigation and consideration of add-on treatment -Add-on tiotropium (long-acting muscarinic antagonist) in patients aged ≥12 years with a history of exacerbations despite Step 4 treatment. Add-on tiotropium by mist inhaler improves lung function and increases the time to severe exacerbation (Evidence B). STEP 5
. STEP 5.")
งานนำเสนอที่คล้ายกัน
















 trial: factorial randomised placebo controlled trial of aspirin and antioxidants.>")






