ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Karoon Ramkaroon, Resident 2 nd year

2
Patient information หญิงไทย คู่ อายุ 40 ปี อาชีพ ค้าขาย ภูมิลำเนา อ. รัษฎา จ. ตรัง Chief complaint แน่นหน้าอก 30 min PTA

3
Present illness – 30 นาทีก่อน ขณะกำลังนอนหลับ แน่นหน้าอกตรง กลางทั่วๆ หายใจไม่ออก ไม่ร้าวไปไหน เหงื่อแตก มือเท้าเย็น ใจสั่น เหนื่อยๆ คลื่นไส้อาเจียน 3 ครั้ง เป็นน้ำลายปนเศษอาหาร ถ่ายเหลว 1 ครั้งเป็นน้ำ ปริมาณไม่มาก ปวดมวนท้องเล็กน้อย

4
PMH – No U/D – No current medication – Seafood allergy

5
Physical examination GA : good consciousness, look anxious, no cyanosis V/S : BT 37 C, BP 140/90 mmHg, PR 100/min regular, RR 30/min HEENT : no injected conjunctiva, thyroid gland not enlarge CVS : tachycardia, regular rhythm, no murmur RS : minimal rhonchi both lung Abd : soft, generalized mild tender, no guarding, hyperactive BS Ext : cold palm and sole NS : E4V5M6, motor gr 4 at least all

6
Problem list Acute chest discomfort Vomit & Diarrhea Acute abdominal pain Seafood allergy

7
Differential diagnosis 1.Anaphylaxis 2.Acute gastroenteritis 3.Angina pectoris

9
Term “Anaphylaxis” first use in 1902, when Portier and Richet vaccinated their dog by sea- anemone toxin and cause it dead

10
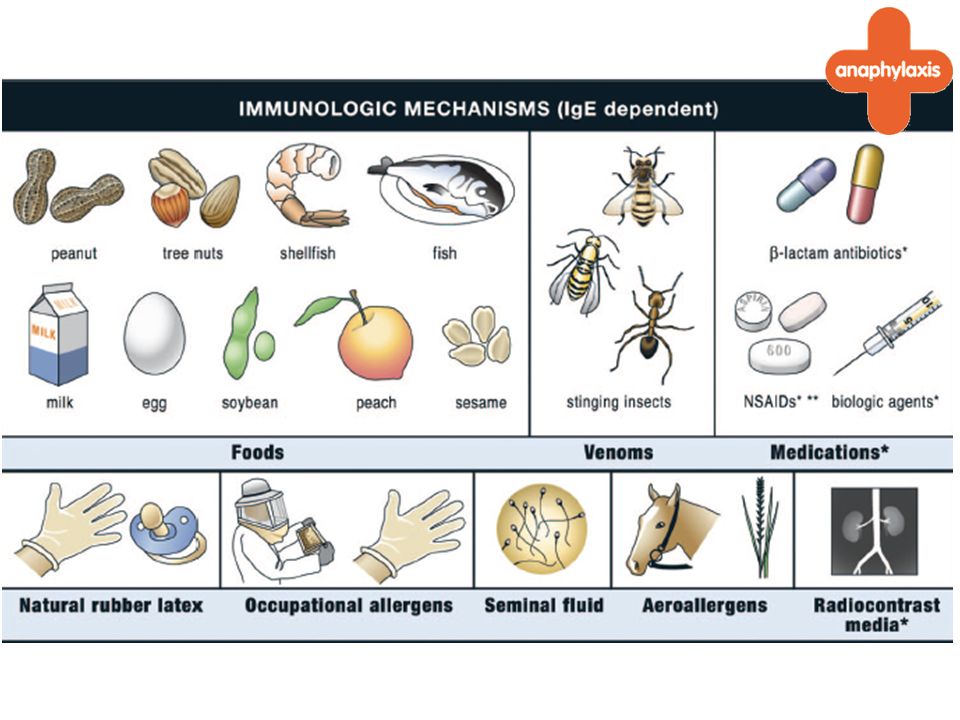
Pathophysiology – Common type is IgE-related hypersensitivity – Ag sensitize IgE-Ab that bind to mast cell and basophils cause degranulation reaction – To Release Histamine, Leukotrienes, Prostaglandin and PAF that cause smooth muscle spasm, vasodilatation, increase vascular permeability and stimulation of nerve ending

13
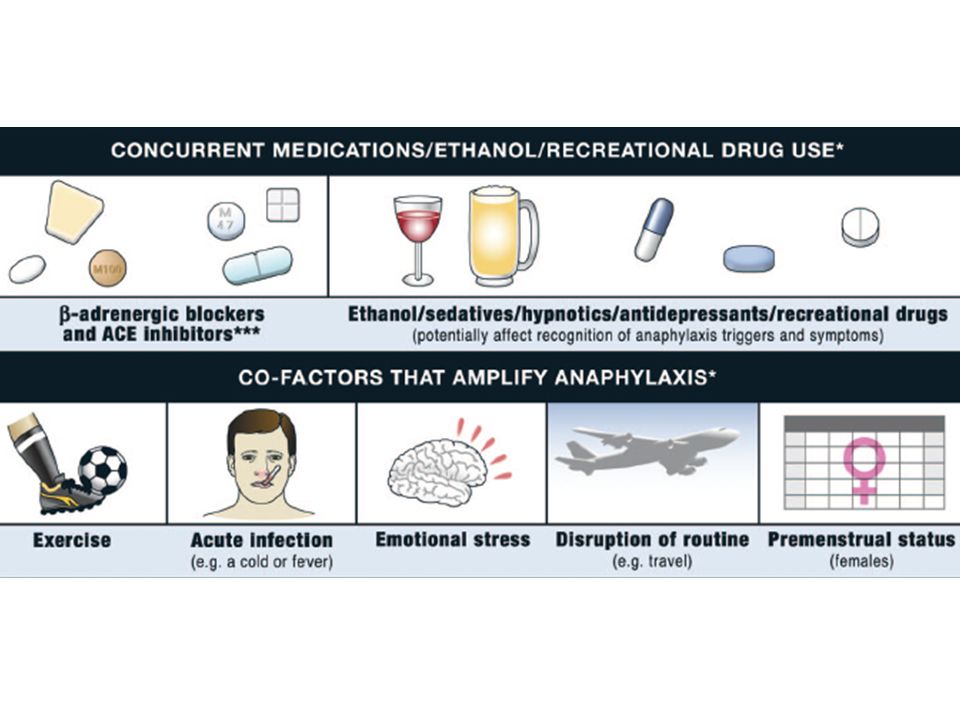
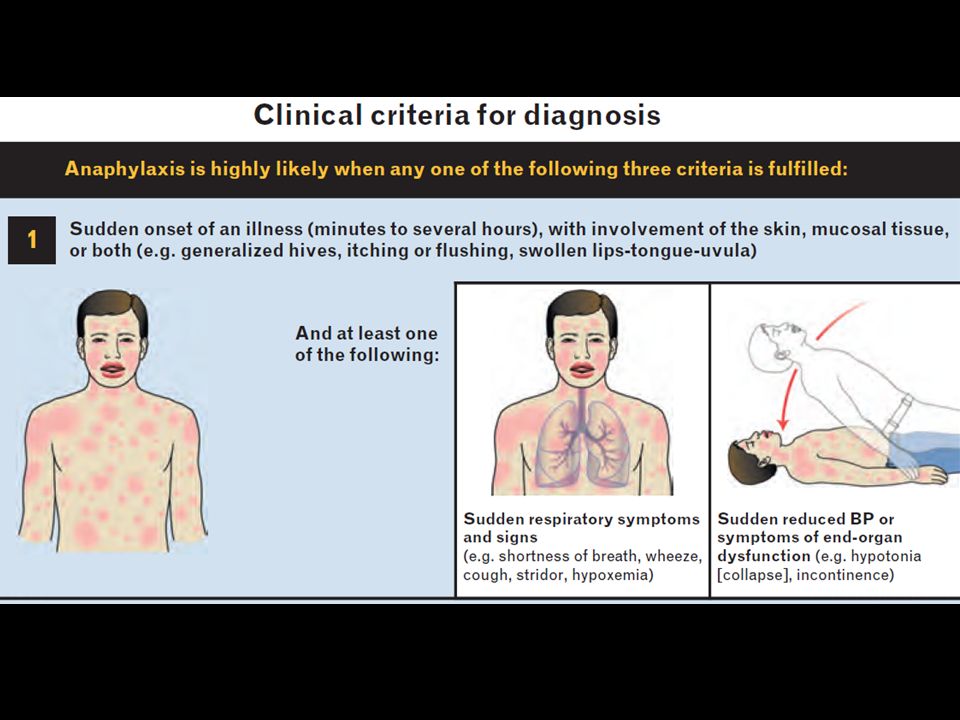
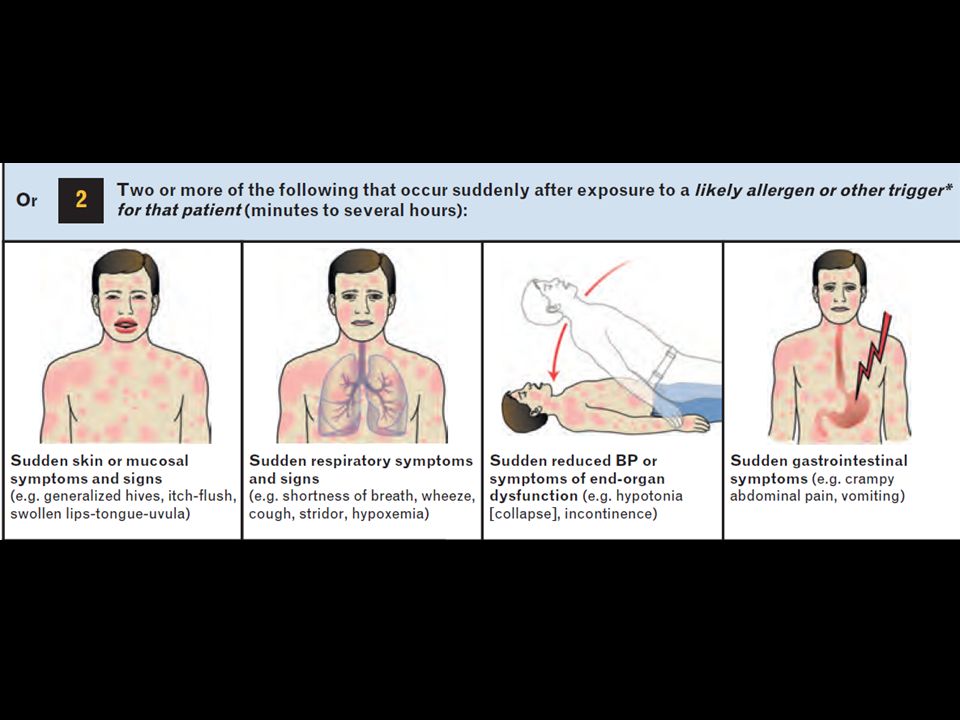
2011 World Allergy Organization Guideline

15
Clinical manifestation – Symptom start from seconds to several hours – 90% : skin & mucosa lesion – RS : nasal congestion, rhinorrhea, cough, hoarseness, shortness of breath, wheezing, stridor – CVS : Dizziness, syncope, chest pain, palpitation, hypotension – GI : Dysphagia, N/V, diarrhea, bloating – NS : Headache, dizziness, blurred vision

23
Medication First line (Priority medication) – Epinephrine 1:1000 (1mg/ml) IM 0.01 mg/kg, max 0.5 adult (0.3 child) Second line – H1-antihistamine IV, eg: Chlopheniramine 10 mg (adult), diphenhydramine (Benadryl) 25-50mg in child – B2-adrenergic agonist, eg: Salbutamol NB – Glucocorticoid IV, eg: Hydrocortisone 200mg, methylprednisolone 50-100 mg – H2-antihistamine IV, eg: ranitidine 50 mg
 – Epinephrine 1:1000 (1mg/ml) IM 0.01 mg/kg, max 0.5 adult (0.3 child) Second line – H1-antihistamine IV, eg: Chlopheniramine 10 mg (adult), diphenhydramine (Benadryl) 25-50mg in child – B2-adrenergic agonist, eg: Salbutamol NB – Glucocorticoid IV, eg: Hydrocortisone 200mg, methylprednisolone mg – H2-antihistamine IV, eg: ranitidine 50 mg")
24
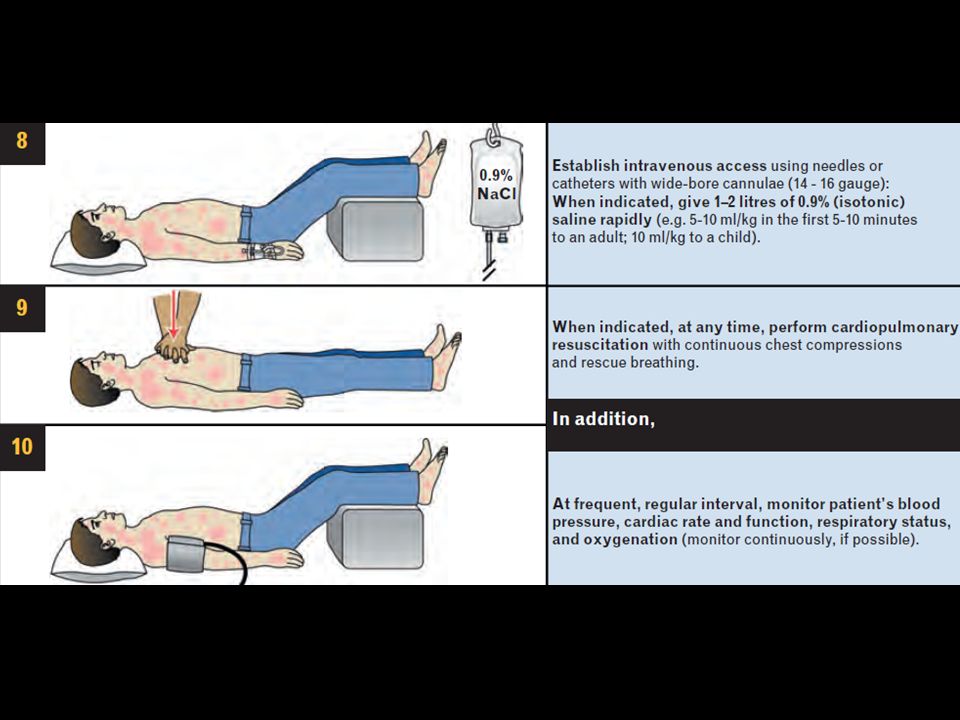
Comment Treatment – Early recognition – Epinephrine is drug of choice and must be administrated – In case of Insect stinger, apply tourniquet at proximal part of lesion and administration of 0.2 ml of Epinephrine 1:1,000 into site and remove Ag – Hypotension : Epinephrine or Dopamine infusion and volume expander such as NSS (Drug of choice is Dopamine) – Respiratory support and bronchodilator NB – Antihistamine, H1 + H2 blocker is more effective than alone – IV or PO corticosteroid is for alleviate late recurrence (equal effective) – The incidence of rebound anaphylaxis is up to 20%. Patients should be observed in the emergency department for 4 to 24 hours before discharge

25
Anaphylaxis

งานนำเสนอที่คล้ายกัน










, MSc in Pharm (Pharmacology)>")














