ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Approach to airways disease and smoke related disease
ผศ. นพ. วัชรา บุญสวัสดิ์ M.D., Ph.D. ภาควิชาอายุรศาสตร์ คณะแพทย์ศาสตร์ มหาวิทยาลัยขอนแก่น

2
Obstructive airway disease
Pressure FLOW Resistance

3
Irreversible FEV1 Δ <15%
???? Reversible FEV1 Δ>15%

4
Spirometry FEV1/ FVC <70%

5
Spirometry FEV1/ FVC <70%

6
Peak Flow meter (เครื่องวัดความเร็วสูงสุด)
")
7
Bronchodilator Test เป่าสมรรถภาพปอด หรือ Peak Flow ก่อนและหลังพ่นยาขยายหลอดลม 15 นาที FEV1 เพิ่มขึ้นมากกว่า 15 % ถือว่าเป็นโรคหืด PEFR เพิ่มขึ้นมากกว่า 20% ถือว่าเป็นโรคหืด PEFR เพิ่มขึ้น 300 = 30% Salbutamol inhaler 2 puff รอเวลา 15 นาที PEFR =300 L/min PEFR =390 L/min

8
asthma Cough Wheeze Dyspnea Reversible airway obstruction

9
Reversible airway obstruction

10
Airway Hyperresponsiveness Stimuli Reversible airway obstruction

11
การทดสอบความไวของหลอดลม

12
Methacholine dose response curve
PD20

13
Pathology of asthma Smooth muscle hypertrophy Mucosal disruption
Mucus plug Cells infiltration

14
ความรู้เกี่ยวกับโรคหืด Before 1980
Bronchospasm ความรู้เกี่ยวกับโรคหืด Before 1980 Airway hyperresponsive Smooth muscle hypertrophy

16
Normal Asthma

17
Allergen inhalation challenge
Early asthmatic response Late asthmatic response Increase AHR Increase inflammatory cells

18
ความรู้เกี่ยวกับโรคหืด 1980-1990
Bronchospasm ความรู้เกี่ยวกับโรคหืด Inflammation Airway hyperresponsive

19
Change in FEV1 in asthmatic

20
Early intervention with inhaled steroid
2 4 6 8 10 12 <2 2-3 3-5 > 5 Annual change in % predicted FEV1 p = 0.02 for correlation Children2 Adults1 6-12 <6 1-2 5-10 >10 2-5 20 30 40 years months Duration of symptoms Duration of symptoms (years) Maximum increase in PEF (%) p = for correlation 1. Selroos et al, Chest 1995 2. Agertoft and Pedersen, Respir Med 1994
 Maximum increase in. PEF (%) p = for correlation. 1. Selroos et al, Chest Agertoft and Pedersen, Respir Med")
21
Haahtela T et al. N Engl J Med 1994;331:700-5.

22
Airway remodelling Epithelium damage Normal Asthma
Sub-basement membrane thickening Smooth muscle hypertrophy and hyperplasia Mucus metaplasia Increase vascularity Normal Asthma

23
Airway remodelling 1. Persistent airway obstruction
2. Persistent airway hyperresponsiveness Normal Asthma

24
ความรู้เกี่ยวกับโรคหืด 1990-2000
Bronchospasm ความรู้เกี่ยวกับโรคหืด Inflammation Remodelling Airway hyperresponsive

25
Changing concept in asthma treatment
short-acting b2-agonists Inh corticosteroid Combination Bronchospasm Inflammation Airway Hyperresponsiveness Remodelling 1975 1980 1985 1990 1995 2000

26
1995 2002 1994 1997 2004
27
Is it Asthma? Recurrent episodes of wheezing
Troublesome cough at night Cough or wheeze after exercise Cough, wheeze or chest tightness after exposure to airborne allergens or pollutants Colds “go to the chest” or take more than 10 days to clear

28
Definition of asthma Airway inflammation Airway hyperresponsiveness
Reversible airway obstruction Symptoms (cough, wheeze, dyspnea)
")
29
Asthma Diagnosis History and patterns of symptoms Physical examination
Measurements of lung function

30
เป้าหมายของการรักษาโรคหืด
1994 เป้าหมายของการรักษาโรคหืด สามารถควบคุมอาการของโรคให้สงบลงได้ ป้องกันไม่ให้โรคกำเริบ ทำให้สมรรถภาพปอดไกล้เคียงคนปกติมากที่สุด ทำให้ผู้ป่วยดำรงชีวิตได้เหมือนคนปกติ หลีกเลี่ยงผลแทรกซ้อนจากยา ป้องกันการเสื่อมของสมรรถภาพปอดจนเกิดการอุดกลั้นอย่างถาวร ป้องกันการเสียชีวิตจากโรคหืด 2004

31
ขั้นตอนการดำเนินการในการรักษา
1994 ขั้นตอนการดำเนินการในการรักษา ให้ความรู้แก่ผู้ป่วยและญาติ หลีกเลี่ยงสิ่งที่ก่อให้เกิดการหอบ จำแนกความรุนแรงของโรค จัดแผนการรักษาที่เหมาะสม จัดแผนการรักษาเมื่อมีการหอบเฉียบพลัน ให้การดูแลรักษาต่อเนื่อง 2004

32
Pharmacological therapy
Relievers Inhaled fast-acting b2-agonists Controllers Inhaled corticosteroids Inhaled long-acting b2-agonists Oral anti-leukotrienes Oral theophyllines

33
Inhaled corticosteroids
Beclomethasone Fluticasone Budesonide

34
Classification of asthma severity: GINA 1995
Severe Persistent Moderate persistent Mild persistent Intermittent <1/wk >1/wk daily Day symptoms daily <2/mo >2/mo >1/wk frequent Night symptoms >80% >80% 60-80% <60% PEFR <20% 20-30% >30% >30% PF variability

35
GINA 2002 GINA1995 High dose ICS +other controller ICS+LABA
Level 4 ICS+LABA high dose ICS Level 3 ICS Level 2 B2 agonist prn Level 1

36
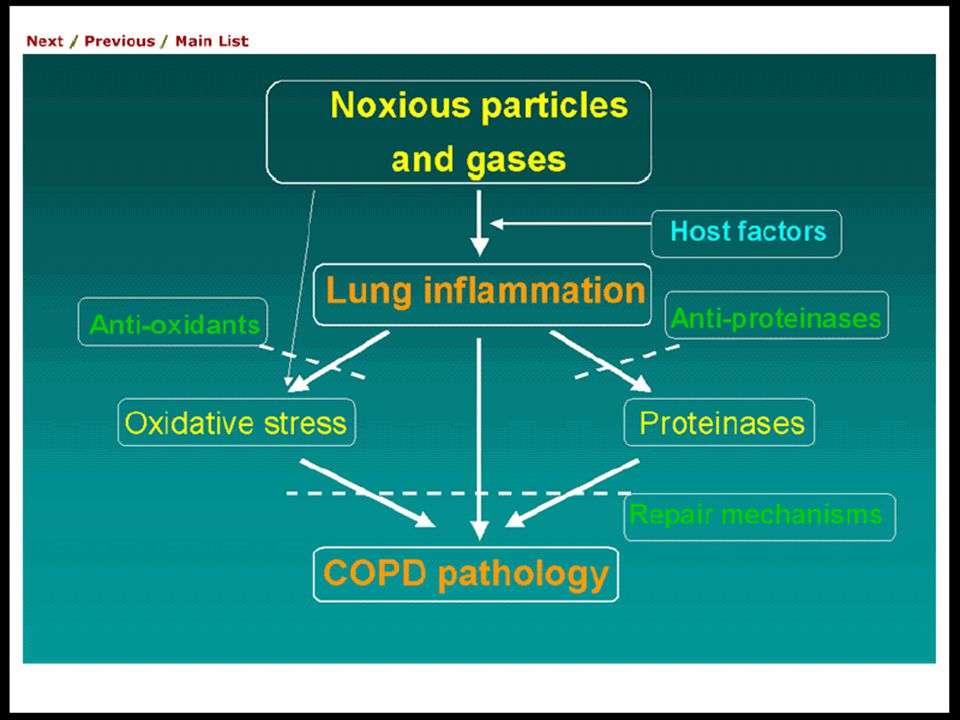
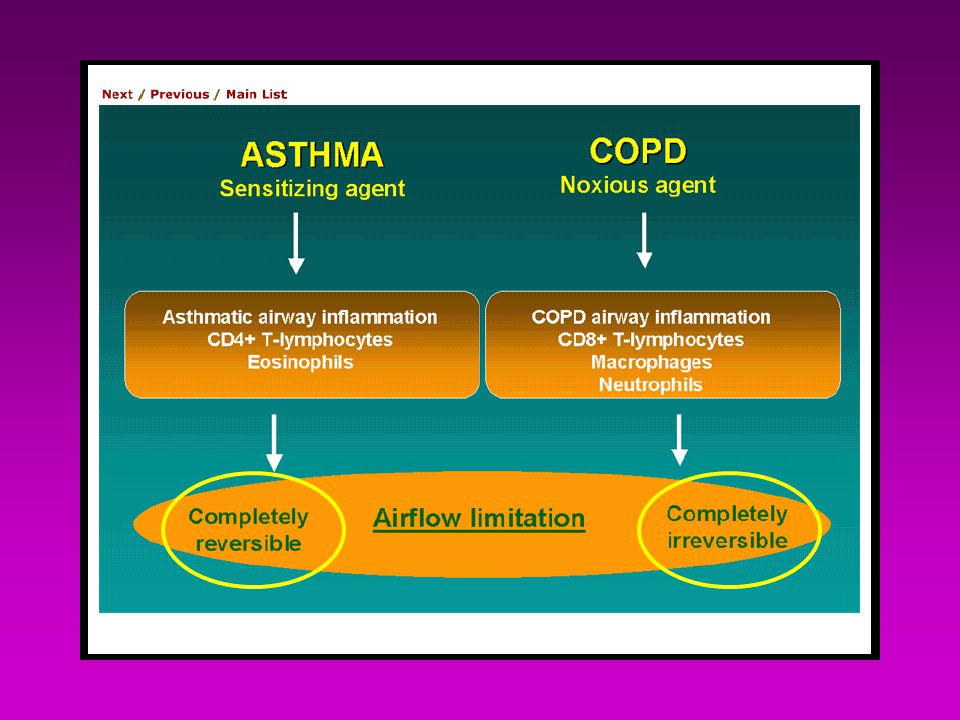
Definition of COPD COPD is a disease state characterized by airflow limitation that is not fully reversible. The airflow limitation is usually both progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases.

41
+/- Diagnosis of COPD Spirometry post bronchodilator FEV1/ FVC <70%
GOLD = Global Initiative in Obstructive Lung Disease 2001 Diagnosis of COPD Exposure to risk factors Tobacco occupation pollution Symptoms Cough Sputum dyspnea +/- Spirometry post bronchodilator FEV1/ FVC <70%

42
GOLD classification of COPD
At-Risk Stage (Stage 0) No spirometric changes Chronic symptoms (cough, sputum) Mild (Stage I ) FEV1/FVC < 70% FEV1 > 80% predicted Moderate (Stage II ) 50% < FEV1 <80% predicted Severe (Stage III ) Very Severe (Stage IV) 30% < FEV1 <50% predicted FEV1 <30% predicted or presence of respiratory insufficiency or right hart failure GOLD = Global Initiative in Obstructive Lung Disease 2003
 No spirometric changes. Chronic symptoms (cough, sputum) Mild (Stage I ) FEV1/FVC < 70% FEV1 > 80% predicted. Moderate (Stage II ) 50% < FEV1 <80% predicted. Severe (Stage III ) Very Severe (Stage IV) 30% < FEV1 <50% predicted. FEV1 <30% predicted. or presence of respiratory insufficiency or right hart failure. GOLD = Global Initiative in Obstructive Lung Disease")
43
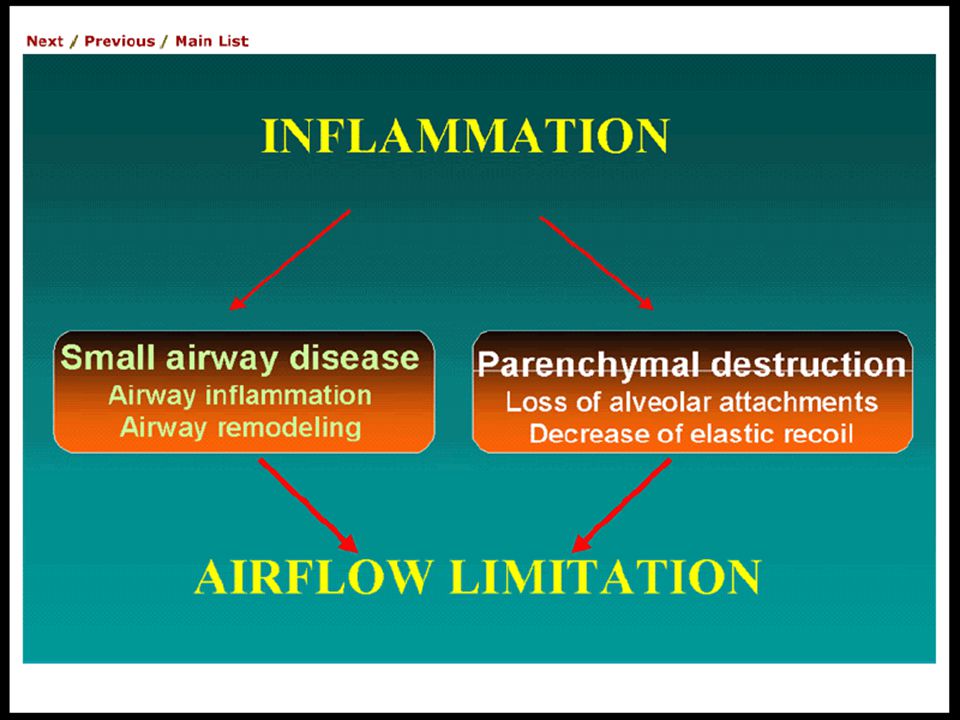
Exercise limitation (Dyspnea)
Pathophysiology COPD Airflow obstruction V/Q Mismatching Work of breathing VD/VT PaO2 Ventilatory capacity Ventialatory requirement Exercise limitation (Dyspnea)
")
45
Treatment Retard the progression of airflow obstruction
Minimizing airflow obstruction Prevent complication Optimizing functional capacity

46
Prevent disease progression

47
Minimizing airflow obstruction
Bronchodilators Anticholinergics B2 agonist Theophylline

48
Corticosteroids Oral Inhaled

49
Number of exacerbations per year stratified by baseline FEV1
ISOLDE. BMJ2000;320:

50
Corticosteroids

51
GOLD pharmacological treatment
Regular bronchodilator treatment inhaled corticosteroids Oxygen therapy FEV1 <30% Regular bronchodilator treatment Consider inhaled corticosteroids FEV % Regular bronchodilator treatment FEV % Short acting bronchodilator as needed FEV1>80%

52
GOLD pharmacological treatment
LABA ICS Oxygen therapy Regular bronchodilator treatment inhaled corticosteroids Oxygen therapy FEV1 <30% Regular bronchodilator treatment Consider inhaled corticosteroids LABA ICS FEV % Regular bronchodilator treatment FEV % Short acting bronchodilator as needed FEV1>80%

53
GINA asthma guidelines
LABA ICS prednisolone Severe persistent LABA ICS Moderate persistent ICS Mild persistent Short acting bronchodilator as needed Intermittent

56
จำนวนคนไทยที่สูบบุหรี่(อายุ 11ปีขึ้นไป)
ปี ประชากร คนสูบบุหรี่ ร้อยละ ชาย หญิง ,685,940 8,629, ,245,800 10,377, ,680,300 10,406, ,905,600 10,230, สำนักงานสถิติแห่งชาติ

57
6000 ชนิด สารพิษในควันบุหรี่ คาร์บอนมอน๊อกไซด์ นิโคติน ทาร์

58
โรคสำคัญที่เกิดจากการสูบบุหรี่
โรคหลอดเลือดตีบ มะเร็ง ถุงลมปอดโป่งพอง

59
Causes of death related to smoking
Causes of death no.of death mortality ratio CA lung * CA esophagus,larynx, mouth, toung,lip * CA bladder * CA prostrate CA liver,gall bladder N= f/u 44 months Hammond EC and Horn. JAMA 1958; 166:1172

60
Causes of death related to smoking
Causes of death no.of death mortality ratio Coronary artery disease * Cerebrovascular disease * aortic aneurysm * other vascular diseases * Pneumonia/influenza * N= f/u 44 months Hammond EC and Horn. JAMA 1958; 166:1172

61
Number of daily cigarettes and risk for lung cancer
UK doctor n =34440 Doll R BMJ 1976

62
Carcinogenic substances in cigarette smoke
Polyaromatic hydrocarbon aromatic amines aldehydes inorganic compounds N-nitrosamines

63
COPD mortality in relation to cigarette smoking
standardized mortality ratio never smoke former smoke current smoke 34440 British doctor Doll. BMJ 2: ;1976

65
Tobacco use results in true drug dependence
Effective treatment exist Treatment are cost-effective

66
5A’s for Promoting Smoking Cessation
Ask about tobacco use at every visit Advice to quit Assess readiness to quit Assist cessation by providing evidence-based aids Arrange follow-up.

67
ADVISE ASSESS ASSIST ARRANGE Follow-up ASK Commend . Congratulate.
Never Commend . Ex- smoker Congratulate. Repeat advise Not ready Motivate Current smoker Encourage cessation Ready to quit Prescribe Rxs Monitor compliance

68
Effective Treatments Are Available
Counselling / behavioural support Pharmacotherapy

69
Counselling Works Brief supportive advice to quit from doctor is effective Counselling by other health professionals is effective Group and individual both effective The greater the support, the greater the chances of success Every smoker should be offered at least brief advice

70
Pharmacotherapy Works
First-line pharmacotherapies Bupropion SR Nicotine replacement therapy Second-line pharmacotherapies Clonidine Nortriptyline

71
Treating tobacco dependence: Approximate long-term quit rates
‘Cold turkey’ 3–7% Brief clinical intervention 10% More intensive counselling 15% Medication (bupropion SR/NRT) 20–30% Medication + counselling 25–35% Source: Fiore MC, et al. Treating Tobacco use and dependence. Clinical Practice Guideline. US DHHS, 2000.
 20–30% Medication + counselling 25–35% Source: Fiore MC, et al. Treating Tobacco use and dependence. Clinical Practice Guideline. US DHHS,")
72
Who should receive pharmacotherapy?
All smokers trying to quit except for special circumstances Special considerations include: - medical contraindications - smoke < 10 cigarettes/day - pregnant/breastfeeding - adolescent smokers

73
Implementation of treatment is unsatisfactory
Smoker insufficiently aware Treatment is not easily accessible Reimbursement is limited

74
Conclusions More than 10 million smokers in Thailand.
Smoking is a major health hazard Effective treatment for tobacco use is exist but under utilized we can do better, we must do better!

งานนำเสนอที่คล้ายกัน









>")











>")

