ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

2
Bone and joint infections

3
Complication Sepsis, Toxic shock disability and deformity

4
Classification Age group Duration of symptom Neonate Childhood
Adolescent Duration of symptom Acute Sub-acute Chronic

5
Classification Route of infection Causative organisms
Hematogenous system** Direct inoculation :Open Fx, operation, skin puncture Soft tissue infection Causative organisms Pyogenic organisms** granulomatous

6
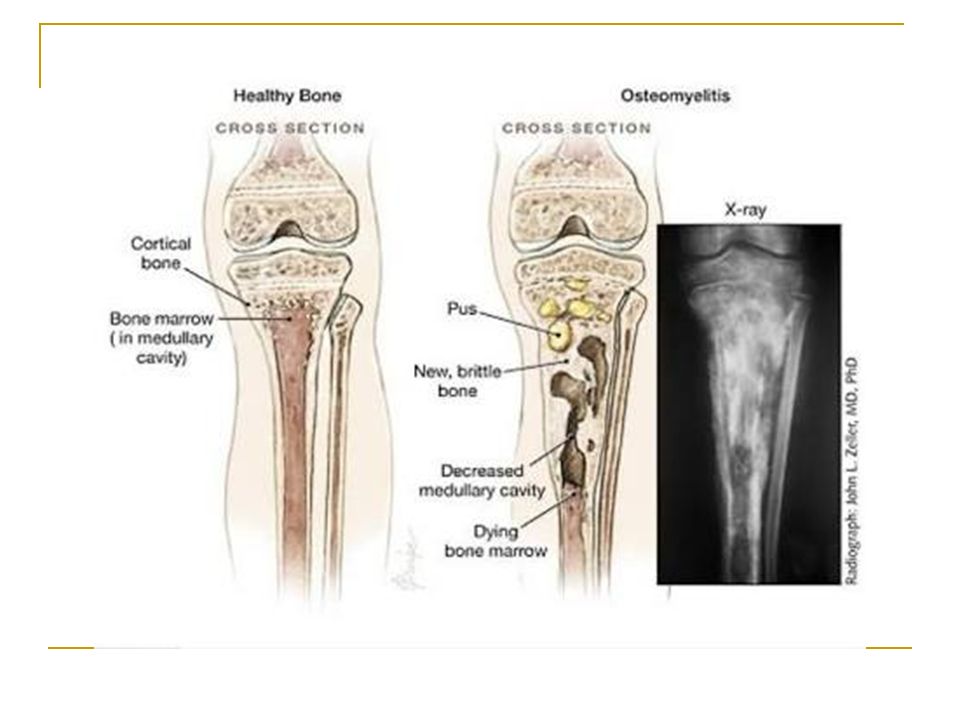
Natural history and Pathogenesis of Acute hematogenous osteomyelitis
Almost at “metaphysis” lower extremities > upper extremities 5 เท่า โดยเฉพาะที่ distal femur และ proximal tibia

7
Source of infection Blood circulation :
infection in Oral, Throat, Ear, Gastrointestinal tract, Urinary tract, Skin and soft tissue

8
Source of infection Trauma (30-50%) หกล้ม กระแทก Minor trauma
Caution : in infant < 18 month มักเกิด septic arthritis ร่วมกับ Osteomyelitis

9
Bacterial colonization
Pathogenesis Source of Infection Blood stream Metaphysis Venous stasis Bacterial colonization

11
Inflammation: acute osteomyelitis
First 24 hours Vascular congestion Polymorphonuclear leukocyte infiltration Exudation

12
Inflammation: acute osteomyelitis
2-3 day No treat with antibiotic Intraosseus pressure intense pain intravascular thrombosis ischemia เด็กจะร้องปวดมาก

13
Suppuration 4-5 days Pus formation Subperiosteal abscess Pus spreading
epiphysis joint medullary cavity soft tissue

14
Necrosis Bone death by the end of a week Bone destruction ← toxin
← ischemia Sequestrum formation small removed by macrophage,osteoclast. large remained

15
New bone formation By the end of 2nd week (10 – 14 days)
Involucrum (new bone formation from deep layer of periosteum ) surround infected tissue. If infection persist- pus discharge through sinus to skin surface Chronic osteomyelitis
 surround infected tissue. If infection persist- pus discharge through sinus to skin surface Chronic osteomyelitis.")
17
joint capsule of 4 metaphysis cause of osteomyelitis
Femoral head and neck ( hip ) Humeral head ( shoulder ) lateral side of distal tibia ( ankle joint ) radial head and neck ( elbow joint )
 Humeral head ( shoulder ) lateral side of distal tibia ( ankle joint ) radial head and neck ( elbow joint )")
18
Signs and Symptoms in infant
Drowsy Irritable history of birth difficulties History of umbilical artery catheterization Metaphyseal tenderness and resistance to joint movement

19
Signs and Symptoms in child
Severe pain Fever History of recent infection Local inflammation pus escape from bone Lymphadenopathy

23
Septic Arthritis

24
Natural History and Pathogenesis of Septic arthritis
ข้อใหญ่ๆ มากกว่าข้อเล็ก single joint pain ยกเว้นใน neonate ที่พบ มากกว่า 1 ข้อ % พบที่ HIP 20 – 25 % พบที่ Knee ที่เหลือเป็น shoulder , ankle , elbow etc

25
Source of infection Same as hematogenous osteomyelitis :
Blood circulation Post operation Skin and tissue infection etc.

26
Cartilage destruction in 5 day
Complication Synovial fluid = good culture media Within 8 hr. loss of glycosaminoglycan Wear and tear synovitis Cartilage destruction in 5 day

27
Signs and symptoms in newborn
Clinical of septicemia : fever ( %) irritable, refuses to feed, rapid pulse Joint swelling Tenderness and resistance to movement of the joint
 irritable, refuses to feed, rapid pulse. Joint swelling. Tenderness and resistance to movement of the joint.")
28
Signs and symptoms in children
acute pain in single joint Swelling and inflammation of the joint. Child looks ill. Limit movement of the joint. Look for a source of infection : toe, boil, otitis media

29
Diff. diagnosis Toxic synovitis เจ็บมากเป็นบาง direction ของการเคลื่อนไหว Toxic synovitis ( transient synovitis ) มักจะเดินได้แต่กะเผลก Rolling test ไม่เจ็บ เจ็บเฉพาะทำ internal ratation Juvenile rheumatoid arthritis จะเห็นข้อบวม แดง ร้อน ไม่ค่อยเจ็บมากเท่าไร ยังขยับข้อได้ ดีพอควร ไม่ look sick กินได้ เล่นดีอยู่
 มักจะเดินได้แต่กะเผลก Rolling test ไม่เจ็บ เจ็บเฉพาะทำ internal ratation. Juvenile rheumatoid arthritis จะเห็นข้อบวม แดง ร้อน ไม่ค่อยเจ็บมากเท่าไร ยังขยับข้อได้ ดีพอควร ไม่ look sick กินได้ เล่นดีอยู่")
30
Diff. diagnosis Cellulitis จะเจ็บที่ผิวหนังภายนอก มีบวม แดง ร้อน ให้เห็นชัด แต่ขยับเคลื่อนไหวข้อไม่เจ็บ Pyomyositis เด็กจะเจ็บตรงกล้ามเนื้อที่เป็น กล้ามเนื้อที่พบบ่อยคือกล้ามเนื้อต้นขา ทำให้ เดินไม่ค่อยไหว มีไข้ ต้นขาบวมลึกๆ อุ่นๆ Psoas abscess เจ็บที่ขาหนีบและท้องน้อย เดินได้แต่ต้องงอข้อสะโพกไว้ตลอด

31
Investigation after admit
CBC U/A ESR aspirate ข้อ หรือ bone ( metaphysis ) Gram stain of synovial fluid C/S Plain film
 Gram stain of synovial fluid. C/S. Plain film.")
32
Investigation : Plain film
พบการเปลี่ยนแปลงหลังจากการติดเชื้อนานกว่า 10 วัน เริ่มจาก periosteal new bone formation, area of lytic and sclerotic lesion, sequestrum and involucrum. ควรเริ่มให้การรักษาทันทีก่อนจะเห็นการ เปลี่ยนแปลงในภาพถ่าย X-ray

35
Investigation: ultrasound
ช่วยบอกว่ามี effusion ในข้อได้ ในบางครั้งก็ บอกได้ว่า เป็น multiecchoic ซึ่งอาจจะ หมายถึง Pus and fibrin มีการใช้ ultrasound ในการช่วยบอกตำแหน่ง ของการเจาะดูด และ follow up ดูว่า effusion ลดลงหรือไม่ หลังให้ การรักษา

37
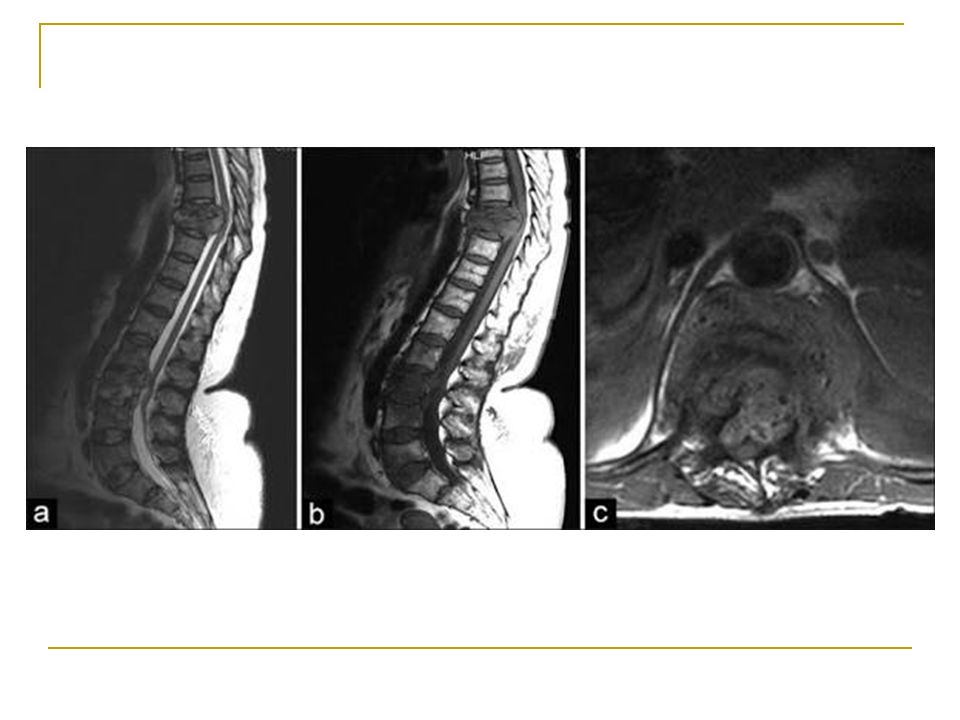
Investigation: MRI ข้อบ่งชี้ : infection ที่ spine หรือ กรณีสงสัยว่าจะเป็นโรคอย่างอื่นมากกว่า เช่น tumor MRI ใน Osteomyelitis มีการลดลงของ marrow signal intensity ใน T1 wieghted เพิ่มขึ้นของ marrow signal intensity ใน T2 weighted images สาเหตุจาก marrow fat ถูกแทนที่ด้วย inflamatory cells และedema

39
Investigation: CT scan
เห็น extent ของ bone destruction ได้ดี ช่วยในการวางแผนการผ่าตัด exposure โดยเฉพาะ Osteomyelitis ของ spine หรือ pelvis

40
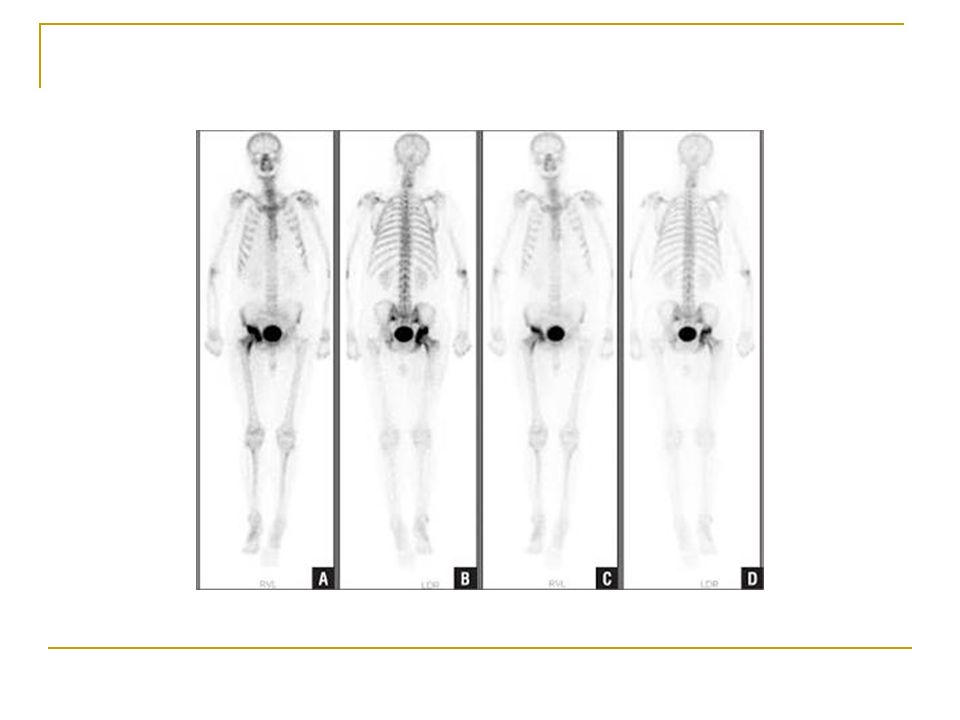
Investigation : Bone Scan
ใช้ในกรณีที่ไม่สามารถ locate lesion ใน early stage หรือมีหลายจุด(foci) 99m TC-HDP sensitive - not specific แบ่งเป็น 2 phases vascular phase warm (hot) uptake ขึ้นกับเลือดที่มาpool ตำแหน่งที่มี swelling & inflamation มาก ต่อมาเป็น osseous phase ซึ่ง warm (hot) uptake จะเห็นตรง bone ที่มี lesion การเจาะข้อหรือเจาะ bone ไม่ได้ทำให้ผล bone scan เปลี่ยนแปลง
 99m TC-HDP - sensitive. - not specific. แบ่งเป็น 2 phases. vascular phase warm (hot) uptake ขึ้นกับเลือดที่มาpool ตำแหน่งที่มี swelling & inflamation มาก. ต่อมาเป็น osseous phase ซึ่ง warm (hot) uptake จะเห็นตรง bone ที่มี lesion การเจาะข้อหรือเจาะ bone ไม่ได้ทำให้ผล bone scan เปลี่ยนแปลง.")
42
Investigation : Aspiration
confirm diagnosis ต้องเจาะก่อนให้ Antibiotic smear for cell and organism culture and sensitivity test

43
Synovial fluid cells count analysis
Early case :WBC 25,000 – 50, 000 / μL Late case : WBC count >50000 / μL (Juvenile rheumatoid arthritis พบได้ เช่นกัน) > 3 day พบ PUS ควรจะผ่าตัดล้างข้อทันที เพื่อเอา debris tissue, fibrin exudate และ enzymes ย่อยสลาย cartilage ออก + ใส่ close suction drainageไว้
 > 3 day พบ PUS ควรจะผ่าตัดล้างข้อทันที เพื่อเอา debris tissue, fibrin exudate และ enzymes ย่อยสลาย cartilage ออก. + ใส่ close suction drainageไว้")
45
Condition Organism Agent
Empirical treatment Condition Organism Agent Organism Agent Sepsis Neonate Staph A, Group A and B strep, coliforms Cloxacillin + gentamicin Infant H.flu, pneumococcus, meningococcus Cetriaxone or cefotaxime Septic Arthritis Group B strep, staph, coliforms H flu, staph A, group A and B strep Cefotaxime Child Staph. aureus Cloxacillin Osteomyelitis Group B strep, staph A, coliforms Infant / Child Nail puncture Through shoes Pseudomonas Cetaxidime + gentamicin Barefoot Discitis

46
Antibiotic treatment Age Pathogen Drugs -Neisseria gonorrhea
1.Healthy Neonate (< 1 mo) -Staphylococcal Gr. B infection - cloxcillin 50 mg/kg/day 2. Infant and children -Staph. Aureus -Gram neg. infection -Haemophilus infection -2nd generation Cephalosporins or Amoxycillin with clavulanic acid 3. Adolescent (11 – 15 years) -Neisseria gonorrhea 150 – 200 mg/kg/day IV divide q 4 – 6 hr. max 12 gm./day 4.Sickle-cell patient -Salmonella infection - Co-trimoxazole - Amoxycillin with clavulanic acid
 -Staphylococcal Gr. B infection. - cloxcillin 50 mg/kg/day. 2. Infant and children. -Staph. Aureus. -Gram neg. infection. -Haemophilus infection. -2nd generation Cephalosporins or Amoxycillin with clavulanic acid. 3. Adolescent (11 – 15 years) -Neisseria gonorrhea. 150 – 200 mg/kg/day IV divide q 4 – 6 hr. max 12 gm./day. 4.Sickle-cell patient. -Salmonella infection. - Co-trimoxazole. - Amoxycillin with clavulanic acid.")
47
Antibiotic treatment Cloxacillin dose 150 – 200 mg/kg/day IV ทุก 4 – 6 ชั่วโมง สูงสุดไม่เกิน 12 gm./day (Neonate ลด dose เป็น 50 mg/kg/day) Gentamicin ใช้กับ Gram negative rod ได้ผลดี dose ที่ให้ 2.5 mg/kg/8 to 24 hr. ปรับตามค่า Cr. Gentamicin มักจะให้ร่วมกับ Cloxacillin ในระยะแรกที่ยังไม่รู้เชื้อ และถ้าจำเป็นต้องให้นานกว่า 1 สัปดาห์ ต้องระวัง Nephrotoxicity

48
Antibiotic treatment Cefotaxime 100 – 200 mg/kg/day IV แบ่งให้ทุก 6 – 8 ชั่วโมง (Neonate ลด dose เป็น 50mg/kg/day) Ceftriaxone 50 – 100 mg/kg/day แบ่งให้ ทุก 12 ชั่วโมง ใช้ได้ผลดีกับ H.influenza , Salmonella, Neiserria gonorrhea กรณีแพ้ยากลุ่ม penicillin ให้ใช้ Clindamycin 30 – 40 mg/kg/day

49
Criteria Switch antibiotic IV to Oral
Clinical sign and symptom: Fever <38 C (>72 hr.) , reduce pain , CRP lower to normal Switch to High dose oral antibiotic : Cloxacillin , cefazolin → Cloxacillin , Cephalexin 100 – 150 mg/kg/d divided qid maximum dosage : 4 g/d
 , reduce pain , CRP lower to normal. Switch to High dose oral antibiotic : Cloxacillin , cefazolin → Cloxacillin , Cephalexin 100 – 150 mg/kg/d divided qid maximum dosage : 4 g/d.")
50
Clinical improvement Acute osteomyelitis Septic arthritis
Fever improvement Early treatment (<48 hr) 7 day 2-3 day Delay treatment 2-3 weeks Total time treatment 3-6 weeks 2-4 weeks
 7 day. 2-3 day. Delay treatment. 2-3 weeks. Total time treatment. 3-6 weeks. 2-4 weeks.")
52
Subacute osteomyelitis
อาการไข้ไม่ชัดเจน เจ็บกระดูกพอทนได้ ถ้าเป็นที่ขาจะเดินได้แต่กะเผลก สภาพทั่วไปของเด็กดีกว่า ESR สูงไม่มาก CRPไม่สูง Hemoculture ไม่ขึ้นเชื้อ Plain film จะเห็น lytic lesion with or without sclerotic border มักพบที่ metaphysis

53
Chronic osteomyelitis
เกิดจากการ delay diagnosis and treatment ของ Acute osteomyelitis ทำให้มี sequestrum,involucrum และ chronic sinus drainage โดยทั่วไป sequestrum จะเห็นได้ ชัดเจนใน plain film

55
Chronic osteomyelitis
การรักษา ผ่าตัด debridement, sequestrectomy, saucerization ร่วมกับการให้ยาปฏิชีวนะ IV pre OP และ post OP ต่ออีก 7 วันเปลี่ยนเป็นยากิน high dose ต่อจน ครบ 6 สัปดาห์ หรือจน ESR < 25

57
Chronic osteomyelitis
การรักษา สิ่งสำคัญ คือต้อง remove sequestrum ซึ่งเป็น dead bone ไม่มี blood supply ทำให้ยาและ phagocytic cells ไม่สามารถเข้าไปกำจัดเชื้อโรคที่ หลบซ่อนอยู่ได้

59
Thank you for your attention

งานนำเสนอที่คล้ายกัน





















>")




 Facilitator: Pawin Puapornpong.>")

