ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Initial Management in Trauma
Phakawat Chunthong,MD

2
Trimodal distribution of death

3
Timing of Death Resulting from Trauma
The first peak 50% Death at the time of injury Primary injury to major organs such as brain,heart,great vessels The injuries are irrecoverable, rapid treatment and transfer may salvage some patients Primary prevention

4
Timing of Death Resulting from Trauma
The second peak 30% From the end of the first peak to several hours GOLDEN HOUR Morbidity and mortality are prevented by avoidance of a secondary injury due to hypoxia,hemorrhage,inadequate tissue perfusion Intracranial hematoma,major hemorrhage from viscera,bones and vessels or hemothorax ATLS [Advanced Trauma Life Support] % Prehospital and in hospital

5
Timing of Death Resulting from Trauma
The third peak 20% Death occurs days or weeks after the injury Sepsis and multiple organ failure Advances in intensive care reduce deaths Improvements in initial management on admission reduce morbidity and mortality

6
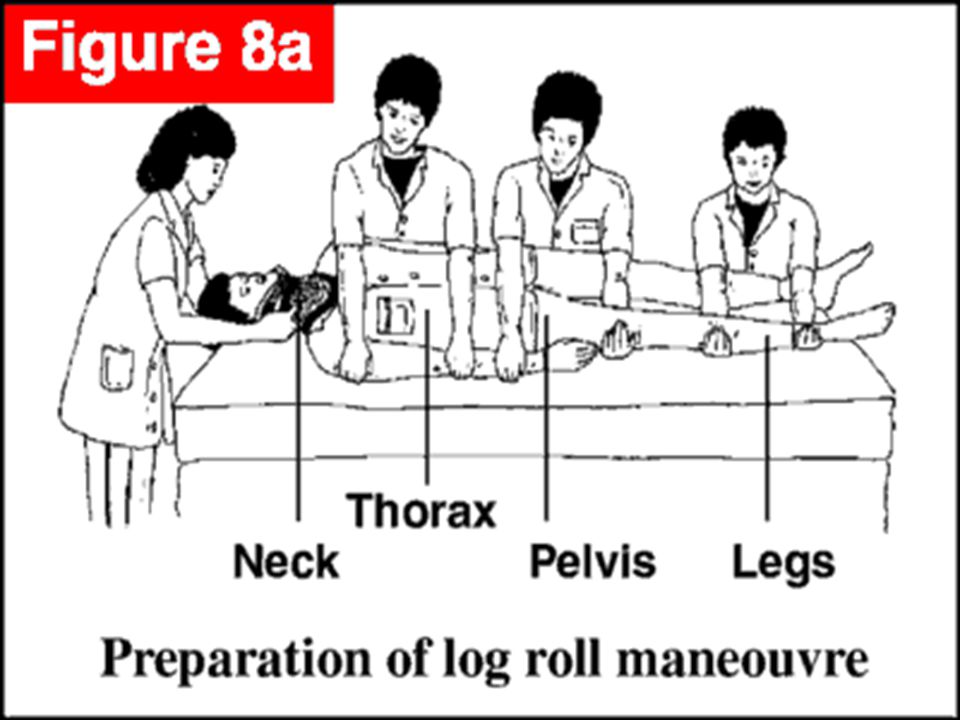
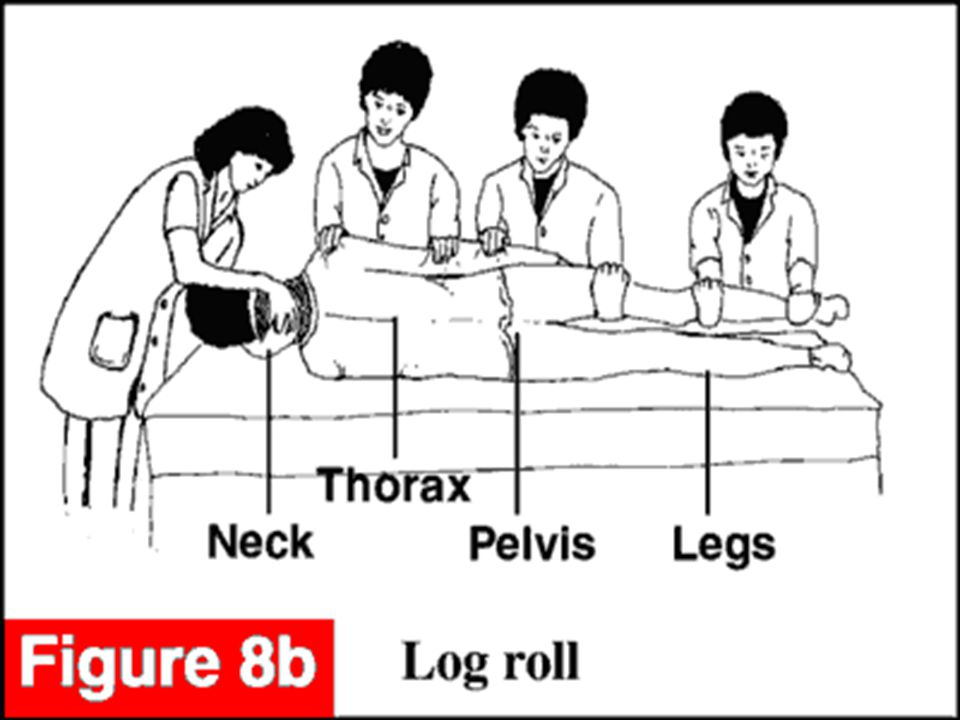
ATLS guideline 1. preparation 2. triage 3. primary survey[ABCDE]
4. resuscitation 5. adjuncts to primary survey and resuscitation 6. secondary survey 7. adjuncts to secondary survey 8. continued post resuscitation monitoring and reevaluation 9. definitive care
![ATLS guideline 1. preparation 2. triage 3. primary survey[ABCDE]](http://slideplayer.in.th/slide/2228693/9/images/6/ATLS+guideline+1.+preparation+2.+triage+3.+primary+survey%5BABCDE%5D.jpg "4. resuscitation. 5. adjuncts to primary survey and resuscitation. 6. secondary survey. 7. adjuncts to secondary survey. 8. continued post resuscitation monitoring and reevaluation. 9. definitive care.")
7
Preparation 1.Prehospital phase [EMS] 2.Inhospital phase
Notify receiving hospital Airway maintenance, control of external bleeding and shock, immobilization of the patient 2.Inhospital phase Resuscitation area Equipment, monitor,warmed fluid Trauma team Protective communicable disease
![Preparation 1.Prehospital phase [EMS] 2.Inhospital phase](http://slideplayer.in.th/slide/2228693/9/images/7/Preparation+1.Prehospital+phase+%5BEMS%5D+2.Inhospital+phase.jpg "Notify receiving hospital. Airway maintenance, control of external bleeding and shock, immobilization of the patient. 2.Inhospital phase. Resuscitation area. Equipment, monitor,warmed fluid. Trauma team. Protective communicable disease.")
8
Cap Gown Gloves Mask Shoe Covers Goggles / face shield

9
Triage Sorting of patients according to ABCDEs Available resources
Mass Multiple

10
Primary survey and resuscitation
identify immediately treatable life threatening injury with initial resuscitation A airway maintenance with cervical spine control B breathing and ventilation C circulation and bleeding control D disability:neurologic status E exposure/environmental control:complete undress the patient but prevent hypothermia

11
A airway maintenance with cervical spine control
Talk to the patient Check the airway patency: secretion, blood, stridor C-spine protection

12
A airway maintenance with cervical spine control
Basic airway management 1.remove of foreign material from mouth and pharynx 2.Chin lift and jaw thrust 3.Oropharyngeal or nasopharyngeal airway

13
A airway maintenance with cervical spine control
Definitive airway 1.orotracheal intubation 2.nasotracheal intubation 3.surgical airway 3.1 cricothyroidotomy 3.2 tracheostomy

14
A airway maintenance with cervical spine control
orotracheal intubation ทำได้ง่าย เร็ว เกิดภาวะแทรกซ้อนน้อยที่สุด ในผู้ป่วยที่มีหรือสงสัยว่ามี cervical spine injury ให้ทำ in-line stabilization nasotracheal intubtion ใส่ยาก ต้องใช้ประสบการณ์ ผู้ป่วยต้องหายใจเองได้ ไม่ควรใส่ในผู้ป่วยที่มีกระดูกหน้าหัก

15
A airway maintenance with cervical spine control

16
A airway maintenance with cervical spine control
surgical airway failure endotracheal intubation maxillofacial injury,blunt or penetrating neck injury ที่ทำให้ไม่สามารถ intubate ได้ตามปกติ Cricothyroidotomy 1.Needle cricothyroidotomy 2.Surgical cricothyroidotomy Tracheostomy

17
A airway maintenance with cervical spine control
1.Needle cricothyroidotomy 2.Surgical cricothyroidotomy

18
A airway maintenance with cervical spine control
C-spine protection unconscious GCS 8 Neck pain Quadriplegia, paraplegia, hemiplegia

19
B breathing and ventilation
Respiration Chest movement RR Tracheal position Breath sound Subcutaneous emphysema Inspection of neck vein and wound

20
B breathing and ventilation
Tension pneumothorax Flail chest Open chest wound Massive hemothorax

21
Tension pneumothorax

22
Tension pneumothorax Chest pain Air hunger Respiratory distress
Tachycardia hypotension Tracheal deviation Unilateral absence of breath sound Neck vein distention Cyanosis

23
Tension pneumothorax

24
Tension pneumothorax Management
Immediate decompression: needle thoracocentesis (Rapidly inserting a large-bore needle into the 2nd intercostal space , midclavicular line of the affected side) Definitive treatment: chest tube
 Definitive treatment: chest tube.")
25
Flail chest กระดูกซี่โครงหัก 2 ตำแหน่งใน 1 ซี่เป็นจำนวน 3 ซี่ขึ้นไปที่อยู่ตำแหน่งติดกัน หรือ มีกระดูกซี่โครงหัก อย่างน้อย1 ซี่ร่วมกับมี costochondral separation หรือ fracture ของ sternum lung contusion,pneumothorax,hemothorax paradoxical respiration การรักษาจะมุ่งแก้ไขภาวะ hypoventilation (จาก pain)และ hypoxia(จาก pulmonary contusion หรือ hemo-pneumothorax)
และ hypoxia(จาก pulmonary contusion หรือ hemo-pneumothorax)")
26
Flail chest

27
Flail chest

28
Open chest wound “sucking chest wound”
บาดแผลของผนังทรวงอกขนาดใหญ่กว่า 2/3 ของเส้นผ่าศูนย์กลางของ trachea เมื่อหายใจเข้าลมภายนอกจะเข้าสู่ช่องอก ทำให้เกิด respiratory distress การรักษาทำโดยปิดบาดแผลด้วย sterile occlusive dressing ปิด plaster ไว้ 3 ด้าน ใส่ chest tube เย็บปิดบาดแผลในห้องผ่าตัด ถ้ามีปัญหาการหายใจมาก ควรใส่ endotracheal tube และช่วยหายใจ

29
Open chest wound

30
Open chest wound

31
Massive hemothorax ภาวะที่มีเลือดออกในช่องปอดมากกว่า 1,500 ml
อาจมีอาการคล้ายกับ tension pneumothorax การรักษาทำโดยการใส่ chest drain และ fluid resuscitation indication for thoracotomy เวลาที่ได้รับบาดเจ็บไม่นานและเลือดออกจาก chest tube มากกว่า 1,500 ml เลือดออกจาก chest tube มากกว่าชั่วโมงละ ml. เป็นเวลาหลายชั่วโมง (4-6 ชม.)
")
32
Massive hemothorax

33
C circulation and bleeding control
BP, PR, LOC Skin color, capillary refill External bleeding site Internal bleeding site: thorax, abdomen, pelvis, extremities

34
Class 1 Class 2 Class 3 Class 4 Blood loss (ml) 750 750-1,500
1,500-2,000 > 2,000 Blood loss (% ) 15 15-30 30-40 >40 Pulse <100 >100 >120 >140 BP normal Pulse pressure Capillary refill Slow (>2s) undetectable RR 14-20 20-30 >35 Urine output(ml/hr) >30 5-15 negligible Mental status slightly anxious mildly anxious anxious/confused confused/ lethargic Fluid replacement crystalloid plus blood Crystalloid
 >40. Pulse. <100. >100. >120. >140. BP. normal. Pulse pressure. Capillary refill. Slow (>2s) undetectable. RR >35. Urine output(ml/hr) > negligible. Mental status. slightly anxious. mildly anxious. anxious/confused. confused/ lethargic. Fluid replacement. crystalloid. plus blood. Crystalloid.")
35
C circulation and bleeding control
Warmed Balnced salt solution 2 large bore 2 liters in mins, child bolus 20 ml/kg G/M

36
C circulation and bleeding control
Hemorrhagic shock Cardiogenic shock neurogenic shock

37
Hemorrhagic shock Rapid response Transient response
Initial fluid therapy ในผู้ใหญ่ที่มี hypotension สามารถให้ bolus ปริมาตร 2 ลิตร ภายใน นาที ในเด็กให้ bolus 20 ml/kg Rapid response Transient response Minimal or no response

38
Hemorrhagic shock Rapid response
หลังให้สารน้ำไปแล้วในตอนแรก ผู้ป่วยจะมีความดันโลหิต ชีพจรและปริมาณปัสสาวะกลับมาเป็นปกติ ลด fluid ลงมาช้าๆเพื่อ maintenance เสียเลือดน้อยกว่า 20%

39
Hemorrhagic shock Transient response
หลังจากได้ initial fluid bolus แล้วมีอาการดีขึ้นชั่วคราว เทื่อลดปริมาณ fluid ที่ให้ลงกลับมีอาการแย่ลงอีก จำเป็นต้องให้ fluid ต่อไปและควรให้เลือด เสียเลือด 20-40% ผู้ป่วยกลุ่มนี้ถ้ายังมีเลือดออกต้องผ่าตัดห้ามเลือด

40
Hemorrhagic shock Minimal or no response
ผู้ป่วยไม่ตอบสนองต่อ fluid หรือเลือดเลย มีความดันโลหิตต่ำตลอด ต้องจำเป็นผ่าตัดแก้ไขและห้ามเลือดโดยด่วน แต่ต้องระมัดระวังจากสาเหตุอื่นเช่น pump failure จาก cardiac injury หรือ cardiac tamponade ต้องทำ CVP,EKG

41
Cardiogenic shock Myocardial dysfunction อาจจะเกิดจาก tension pneumothorax, myocardial contusion, cardiac tamponade, air embolism, myocardial infarction Cardiac tamponade มักเกิดจาก penetrating injury ผู้ป่วยจะมี Beck’s triad คือ venous pressure elevation, hypotension, distance heart sound ซึ่งอาการคล้ายกับ tension pneumothorax myocardial contusion พบใน blunt chest injury เช่นหน้าอกกระแทกพวงมาลัย

42
Cardiogenic shock

43
neurogenic shock มีสาเหตุจาก spinal cord injury ระดับ mid thoracic ขึ้นไป ไม่ได้เกิดจาก head injury ถ้ามีมักเป็น hypovolemic shock หรือ severe brain injury ผู้ป่วย loss symphathetic tone เกิด vasodilatation

44
neurogenic shock ผู้ป่วยจะมี hypotension แต่ heart rate ไม่เร็ว
initial treatment ยังเป็น fluid resuscitation ถ้าให้ adequate resuscitation แล้วแต่ยังมี hypotension ควรพิจารณาให้ vasopressor drug ต้องมี CVP monitoring เพื่อช่วยปรับปริมาณการให้ fluid resuscitation

45
D disability:neurologic status
GCS Pupils size and light reaction

46
GLASGOW COMA SCALE Variables Score Eye opening Spontaneous To speech
To pain None 4 3 2 1 Verbal response Oriented Confused conversation Inappropriate words Incomprehensible sounds 5 Best motor response Obeys commands Localizes pain Normal flexion Abnormal flexion Extension 6

47
E exposure/environmental control
Undressed Exam back region All entry and exit wound Prevent hypothermia(warming light, warm blankets, warm resuscitation fluid, warm inspired air) Patient’s right, closed area
 Patient’s right, closed area.")
50
adjuncts to primary survey and resuscitation
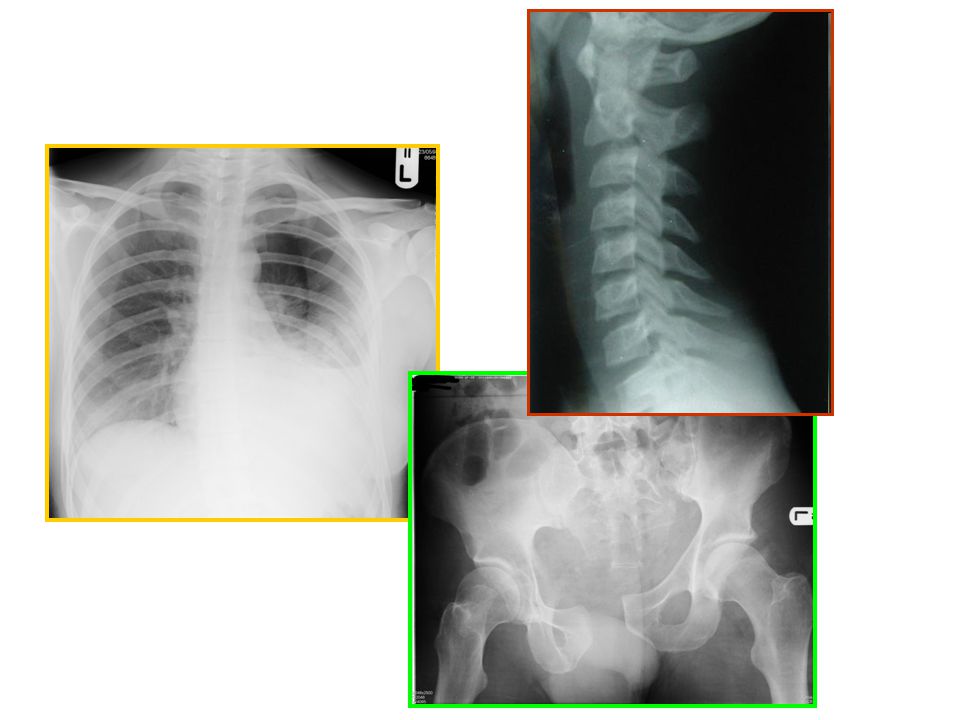
Vital signs ECG O2 sat,pulse oximeter Uinary and gastric catheter Urine out put Trauma film:lateral c-spine,CXR,pelvis DPL/FAST

52
Primary survey and resuscitation
Protect and secure airway Ventilate and oxygenate Stop the bleeding! Vigorous shock therapy Protect from hypothermia

53
secondary survey The complete history and physical examination

54
Secondary survey History Physical exam: head to toe
“tubes and fingers in every orifice” Complete neurological exam Special diagnosis tests reevaluation

55
Secondary survey History “AMPLE” A:Allergies
M:Medication currently being taken by the patient P:Past illness and operations,pregnancy L:Last meal E:Event/Environment related to the injury

56
Secondary survey Mechanism of injury

57
Secondary survey HEAD Signs of skull base fracture Pupillary size
Hemorrhages of conjunctiva/fundi Visual acuity Penetrating injury Contact lens Dislocation of lens Hyphaema Ocular movement Posterior scalp laceration

58
Secondary survey MAXILLOFACIAL
Associated with airway obstruction or major bleeding Fracture cribriform plate No NG tube [performed oral route]

59
Secondary survey NECK Cervical tenderness, subcutaneous emphysema
Oesophageal injury Tracheal/laryngeal injury Carotid injury (penetrating/blunt)
")
60
Secondary survey Inspect Palpate Percuss Auscultate Obtain x-rays
CHEST Inspect Palpate Percuss Auscultate Obtain x-rays

61
Secondary survey Inspect Auscultate Palpate Percuss Reevaluate
ABDOMEN Inspect Auscultate Palpate Percuss Reevaluate Special studies

62
Secondary survey Perineum:contusion,hematoma, laceration,urethral blood Rectum:sphincter tone,high riding prostate,pelvic fracture,rectal wall integrity,blood Vagina:blood,laceration

63
Secondary survey Musculoskeletal Contusion, deformity Pain Perfusion
Peripheral neurovascular status X-ray

64
Secondary survey Neurologic: brain GCS Score Lateralizing signs
Frequent reevaluation Prevent secondary brain injury

65
Secondary survey Neurologic: spine and cord
Complete motor and sensory exams Imaging as indicated Reflexes

66
Adjuncts to secondary survey
Special diagnostic tests as indicate CT Contrast x-ray studies Extremity x-ray Endoscopy Ultrasound

67
Monitoring and revaluation
Minimize missed injury High index of suspicion Adult urine output 0.5ml/kg/hr Pediatric urine output 1ml/kg/hr Pain relief -- IM should be avoid

68
Definitive care OR ICU Refer

69
?

งานนำเสนอที่คล้ายกัน


![คำสั่ง DISPLAY รูปแบบที่ 1 DISPLAY identifier-1, identifier-2 … literal-1 literal-2 [ UPON mnemonic-name ] ตัวอย่าง DISPLAY STUDENT-NAME. DISPLAY.](/7/1925791/big_thumb.jpg "คำสั่ง DISPLAY รูปแบบที่ 1 DISPLAY identifier-1, identifier-2 … literal-1 literal-2 [ UPON mnemonic-name ] ตัวอย่าง DISPLAY STUDENT-NAME. DISPLAY.>")
















 MICU 68% CCU 32%>")