ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Facilitator: Pawin Puapornpong
Case study 46 Facilitator: Pawin Puapornpong

2
CASE 1 หญิงตั้งครรภ์ไทย อายุ 27 ปี ทราบว่าตั้งครรภ์ 2 วันก่อนมารพ. จึงมาฝากครรภ์ครั้งแรกที่รพ. ท่านเป็นแพทย์ท่านแรกที่พบผู้ป่วย ท่านจะซักประวัติและตรวจร่างกายอะไรบ้าง

3
หญิงตั้งครรภ์ไทย อายุ 27 ปี G1P0A0 ทราบว่าตั้งครรภ์จาก การตรวจ UPT 2 วันก่อนมารพ. ไม่มีคลื่นไส้ อาเจียน รับประทานอาการได้ตามปกติ ไม่ปัสสาวะแสบขัด ไม่มีปวดท้อง ไม่มีท้องเสียถ่ายเหลวหรือท้องผูก ไม่มีไข้ ไม่มีเลือดออกผิดปกติหรือตกขาวทางช่องคลอด underlying disease HIV (Diagnosis 2 yr PTA ที่ศกพ. ) Medication : Zidovodine (300 mg) + Lamivodine (150 mg) 1 เม็ด ทุก 12 ชั่วโมง Lopinavir (200 mg) 2 เม็ด ทุก 12 ชั่วโมง No drug/food allergy No smoking or alcohol taking and drug used Current medication No surgical history
 Medication : Zidovodine (300 mg) + Lamivodine (150 mg) 1 เม็ด ทุก 12 ชั่วโมง. Lopinavir (200 mg) 2 เม็ด ทุก 12 ชั่วโมง. No drug/food allergy. No smoking or alcohol taking and drug used. Current medication. No surgical history.")
4
Family history มารดาเป็นโรคเบาหวาน ไม่มีคนในครอบครัวเป็นโรคมะเร็ง โรคเลือด โรคถ่ายทอดทางพันธุกรรม ไม่มีประวัติคนในครอบครัวเป็นโรคความดันโลหิตสูง ไขมันในเลือดสูง

5
OB-GYN G1P0A0 LMP : ประมานกลางเดือนธันวาคมปีที่แล้ว ( 15 ธันวาคม 2557) GA by LMP 10+2 wk , EDC 22/9/58 First ANC ประวัติการคุมกำเนิด : ไม่ได้คุมกำเนิด ไม่มีประวัติตกขาวผิดปกติหรือเลือดออกทางช่องคลอด ประวัติการฉีด tetanus vaccine : ครบ 3 เข็ม 2 yr PTA

6
Physical examination Vital sign BT 37.2 C PR 70 bpm RR 14 /min BP 110/75 mmHg BW 55 kg, Ht 165 cm, BMI 20.20 GA : A Thai pregnancy, good consciousness, co-operated, not pale , no jaundice HEENT : not pale conjuctiva, anicteric sclearae, No lymphadenopathy Neck : No thyroid enlargement CVS : normal s1s2, no murmur, regular pulse RS : normal breath sound, clear both lungs

7
Breast : symmetrical shape and size, no ulcer, no skin dimple
Abdomen : No superficial vein dilatation, no surgical scar, normoactive bowel sound Leopold’s maneuver : can’t be evaluated Uterine contraction : can’t be evaluated Extremity : no pitting edema, no deformity, no rash, capillary refill < 2 sec

8
Problem lists 1. Frist ANC : G1P0A0 GA 10 wk by LMP 2. ANC risk
Uncertain LMP Risk for GDM HIV infection

9
Prenatal care

10
Maternal prenatal care
Fetal prenatal care

11
Maternal Prenatal care
Aim Define maternal and fetal health status Estimate gestational age Initiate a plan for continuing obstetrics care Maternal health status and Gestational risk Normal, At Risk, have some conditon or complication Screening and Detect history taking, Physical exam and Laboratory screening Treatment and advice Follow up and Plans

12
Maternal Prenatal care
Maternal history taking Basic information: Age, race, occuptation etc Previous pregnancy history and complication LMP (+/- prev 3mo) and previous contraception to confirm GA and EDC Underlying disease and Current medication Patient and couple family history Abnormal symptoms 1st trimester : nausea/vomit, abnormal vaginal bleeding, abdominal pain 2nd trimester : fetal quickening 3rd triemester : Labor pain, abnormal bleeding, quickening
 and previous contraception to confirm GA and EDC. Underlying disease and Current medication. Patient and couple family history. Abnormal symptoms 1st trimester : nausea/vomit, abnormal vaginal bleeding, abdominal pain 2nd trimester : fetal quickening 3rd triemester : Labor pain, abnormal bleeding, quickening.")
13
Maternal Prenatal care
Physical examination Height, Body weight in every visit Vital signs : Blood pressure General physical examination Fundal height(cm), Leopold’ maneuver Gynecological examination (in some case)
, Leopold’ maneuver. Gynecological examination (in some case)")
14
Fetal Prenatal care Fetal movement Fetal heart rates : CTG (NST)
Fetal Biophysical profile Ultrasonography and Doppler sonography

15
Fetal Prenatal care Fetal movement (FM) Usually present at GA 16-20wk
Diurnal rhythm Factor effect to FM : amniotic fluid amount, maternal serum glucose, smoking, external stimuli(sound, light, vibration), maternal position, maternal attention to count Method :
, maternal position, maternal attention to count. Method :")
16
Fetal Prenatal care Fetal heart rates : CTG (NST)
NST : Non stress test NST should perform at GA>32 wk in low risk case, earlier in high risk Results : Reactive, Nonreactive, Suspicious, Uninterpretable Factor effect to NST results : Gestational age, Maternal drug use, Fetal sleep status, test duration CST : Contraction stress test

17
Common symptoms in pregnancy

18
Nausea and vomiting Backache Varicose and hemorrhoid Heart burn Sleeping and fatigue Leukorrhea

19
จากประวัติและตรวจร่างกายดังกล่าว ท่านจะส่งตรวจทางห้องปฏิบัติการอะไรบ้าง

20
Lab investigation Ultrasound confirm GA : 10+2 wk
CBC : Hb 12.6 g/dL, Hct 36.4 %, MCV 82 fL DCIP : negative OF test : negative Blood group O , Rh + Serology : VDRL > non reactive, Anti-HIV > reactive, HBsAg > negative 50 gram Glucose challenge test : 120 mg% Urine protein : negative, Urine sugar : negative

21
การคำนวณครรภ์อายุครรภ์
Ultrasonography Should be perform at least 1 time trend of number of perform are more increasing Aim : correct gestational age and estimate fetal weight(EFW) fetal anatomy , growth and diagnosis of IUGR Anomaly detection Amniotic fluid evaluation Placental grading and location Fetal biophysical profile evaluation
 fetal anatomy , growth and diagnosis of IUGR Anomaly detection Amniotic fluid evaluation Placental grading and location Fetal biophysical profile evaluation.")
22
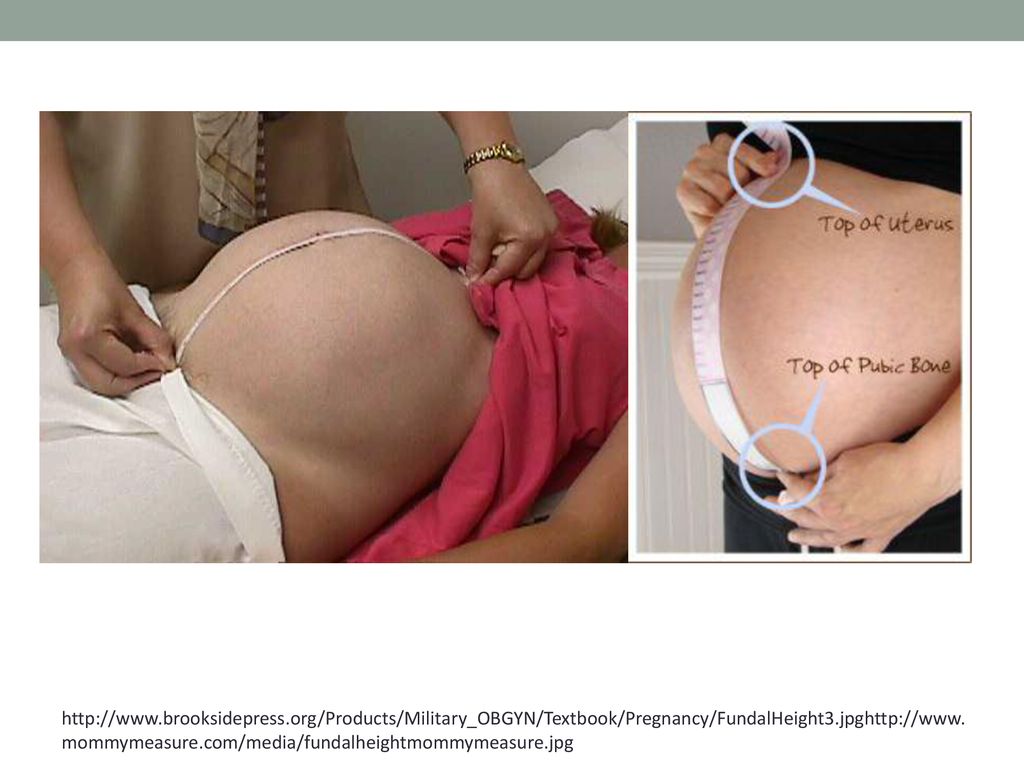
Fundal height Uterine fundus measured in cm. : GA 20-34 wk
Empty bladder Grossly monitor fetal growth and amniotic fluid volume - Obesity or the presence of uterine masses such as leiomyomata may also limit fundal height accuracy. - 17 to 20 weeks, fundal height was 3 cm higher with a full bladder.
23
http://www. brooksidepress
24
ตาราง ANC รายการ ครั้งที่ 1 วันที่ตรวจ สถานที่ตรวจ 2/03/2558 การนัด -
อาการนำ ฝากครรภ์ครั้งแรก น้ำหนัก 55 kg BP 110/75 mmHg Urine protein และ Sugar Negative/negative อายุครรภ์ 10 wk Fundal height

25
รายการ ครั้งที่ 1 Presentation - Fetal heart sound Fatal movement Abnormal symptom Edema การสืบค้นและหัถตการ CBC, DCIP, OF test, Blood group O, Rh VDRL, Anti HIV, HBsAg 50 gm GCT Follow up and plan 4 wk

26
แปลผล ANC มารดามาฝากครรภ์ครั้งแรก GA 10 wk by LMP , GA 10+2 wk ultrasound : GA จาก LMP และ Ultrasound สอดคล้องกัน ความดันโลหิตอยู่ในเกณฑ์ปกติ ไม่พบ protein/ sugar ในปัสสาวะ ไม่คลื่นไส้อาเจียน รับประทานอาหารได้ตามปกติ ผลทางห้องปฏิบัติการ มี Anti HIV positive แต่ CBC, VDRL, HBsAg, 50 gram GCT ไม่พบความผิดปกติ

27
ผู้ป่วยรายนี้มาฝากครรภ์ครั้งที่ 5
GA 26 wk by LMP น้ำหนัก 63 กิโลกรัม (จาก 55 กิโลกรัม) ตรวจ 50 gram GCT : 170 mg/dl 100 gram OGTT : FBS : 80 mg/dl 1hr : 190 mg/dl 2hr : 170 mg/dl 3hr : 145 mg/dl GDM A1
 ตรวจ 50 gram GCT : 170 mg/dl. 100 gram OGTT : FBS : 80 mg/dl. 1hr : 190 mg/dl. 2hr : 170 mg/dl. 3hr : 145 mg/dl. GDM A1.")
28
Management Follow up GDM HIV infection

29
Management ANC : การตรวจครรภ์ครั้งถัดไป ตรวจ urine protein / sugar
VRDL ครั้งที่ 2 เมื่อ GA 32 weeks Follow up Routine ANC visit - 4 weeks intervals until 28 weeks - 2 weeks intervals until 36 weeks - weekly after 36 weeks

30
Four visit ANC model from WHO (in low risk patient) - first visit at
Four visit ANC model from WHO (in low risk patient) - first visit at weeks -second visit at weeks - third visit at 32 weeks -fourth visit at weeks
 - first visit at 8-12 weeks -second visit at weeks - third visit at 32 weeks -fourth visit at weeks.")
31
Risk for GDM ประเมิน risk for GDM

32
Gestational diabetes Two step screening รอตรวจ
50 gram GCT at GA 24 – 28 wk 100 gram OGGT หลังรับประทาน glucose 100 gram ที่ 1st, 2nd, 3rd ชั่วโมง All should be screened for GDM At wk most sensitive but if low risk.. Less benefit from testing Chap57 page1136

33
การแปลผล 100 กรัม OGTT GDM positive diagnosis : ผิดปกติ ≥ 2 ค่า GDM A1 : normal fasting plasma glucose GDM A2 : abnormal fasting plasma glucose

34
การดูแลรักษา GDM การควบคุม เบาหวาน class A1 อาศัยการควบคุมอาหารอย่างเดียว วัด FBS และ/หรือ 2hr PPPG q 1-2wk การควบคุมเบาหวาน class A2 ควบติดตามระดับน้ำตาลเหมือน Overt DM การออกกำลังกายอย่างเหมาะสมจะช่วยควบคุมน้ำตาลมากขึ้น Class A1 ไม่จำเป็นต้องตรวจสอบสุขภาพในครรภ์เพิ่มเติมเป็นพิเศษ แนะนำ check 75 gram OGGT หลังคลอด 2-3 เดือน

35
HIV in pregnancy

36
สตรีตั้งครรภ์ไม่เคยได้รับยาต้านไวรัสและ CD4+ ต่ำกว่า 350
ระยะก่อนคลอด ให้เริ่ม HAART therapy หลีกเลี่ยง Efavarenz ใน ไตรมาสแรก ให้สูตรที่มี ziduvodine ร่วมด้วย หลีกเลี่ยง nervirapine กรณี CD4+ มากกว่า 250 ระยะเจ็บครรภ์คลอด ให้ continue HAART สูตรเดิมและเพิ่ม ziduvudine ระยะหลังคลอด มารดา ให้ continue สูตรเดิมและ consult med เพื่อปรับยา ทารก GA>35 GA30-35 GA<30

37
สตรีตั้งครรภ์ไม่เคยได้รับยาต้านไวรัสและ CD4+ มากกว่า 350
ระยะก่อนคลอด เริ่ม HAART ตอนไตรมาสที่ 2 ให้สูตรที่มี zidovudine หลีกเลี่ยง nervirapine ในกรณี CD4+ > 250 ระยะเจ็บครรภ์ ให้ continue HAART สูตรเดิมและเพิ่ม ziduvudine ระยะหลังคลอด มารดา หยุดยาทุกตัว ยกเว้นกรณีที่ได้ nervirapine เพิ่ม ทารก GA>35 GA30-35 GA<30

38
สตรีตั้งครรภ์ติดเชื้อ HIV ที่รับยาตั้งแต่ก่อนตั้งครรภ์(หรือเคยได้รับยาก่อนตั้งครรภ์แต่ปัจจุบันไม่ได้รับแล้ว) ระยะก่อนคลอด ให้ยาต้านไวรัสสูตรเดิมที่เคยได้รับมา ตรวจ HIV antiretroviral drug resistance testing หากสูตรเดิมไม่มี zidovudine ให้เปลี่ยนเป็นสูตรที่มี ยกเว้นเคยดื้อยาหรือมีผลข้างเคียง หลีกเลี่ยง Efarverine ในไตรมาสแรก หากหยุดยาในไตรมาสแรก ให้หยุดยาทุกตัวแล้วเริ่มต้นใหม่ในไตรมาสที่สอง ระยะเจ็บครรภ์ ให้ continue HAART สูตรเดิมและเพิ่ม ziduvudine ระยะหลังคลอด มารดา ให้ยาสูตรเดิมก่อนเปลี่ยน หรือ consult med เพื่อปรับยา ทารก GA>35 GA30-35 GA<30

39
สตรีตั้งครรภ์ที่ไม่เคยได้รับยาต้านไวรัสมาก่อนและอยู่ในระยะเจ็บครรภ์คลอด
ให้ zidovudine ร่วมกับ nervirapine หากคาดว่าจะคลอดใน 2 ชั่วโมง ไม่ควรให้ nervirapine ระยะหลังคลอด มารดา ให้ zidovudine + Lamivudine + Lopinavir/Ritonavir แล้วรอผล CD4+ count ทารก Zidovudine + Lamivudine นาน 4-6 สัปดาห์ ร่วมกับ nervirapine 2-4 สัปดาห์ หยุดยา ziduvudine + Lamivudine หลังจากหยุด NVP แล้ว 2 สัปดาห์

40
แนวทางการตรวจทางห้องปฏิบัติการ
CD4 ตรวจก่อนเริ่มยาทุกราย ตรวจซ้ำหลังได้ยา 6 เดือน Viral load ตรวจเมื่ออายุครรภ์ 36 สัปดาห์ CBC ตรวจซ้ำหลังได้รับยา 4-8 สัปดาห์ AST,ALT GCT ตรวจก่อนเริ่มยาทุกราย (Lopinavir/Ritonavir) ตรวจซ่ำอนอายุครรภ์ สัปดาห์ หรือหลังได้รับยา 4 สัปดาห์
 ตรวจซ่ำอนอายุครรภ์ สัปดาห์ หรือหลังได้รับยา 4 สัปดาห์")
41
การดูแลในระยะคลอด หลีกเลี่ยงการเจาะถุงน้ำคร่ำ หรือ ติด internal fetal monitoring Labor augmentation ควรทำเมื่อต้องการลดระยะคลอดเพื่อลดความเสี่งในการถ่ายทอดเชื้อจากมารดาไปยังทารก หลีกเลี่ยงการใช้หัตถการช่วยคลอด ยากลุ่ม metergine หรือ ergot alkaloid อาจมีปฏิกริยากับ reverse transcriptase และ protease inhibitors การนัดผ่าตัดคลอด ควรแนะนำในสตรีตั้งครรภ์ที่ติดเชื้อที่มีระดับ HIV-1 RNA มากกว่า 1000 copies/ml ที่อายุครรภ์ 38 สัปดาห์เพื่อลดโอกาสเกิดภาะน้ำเดินก่อนคลอด ในกรณีที่ระดับ HIV-1 RNA น้อยกว่า 1000 copies/ml การนัดผ่าตัดคลอดไม่ช่วยลดอัตรการถ่ายทอดเชื้อจากมารดไปยังทารกลงจากเดิม

42
Thank you

งานนำเสนอที่คล้ายกัน



















