ดาวน์โหลดงานนำเสนอ
1
Interhospital Conference
Ramathibodi hospital 20 March 2012

2
Patient profile ผู้ป่วยเด็กหญิงไทย อายุ 2 ปี 11 เดือน
ภูมิลำเนา จังหวัด นนทบุรี ส่งตัวมารักษา รพ.รามาธิบดี เมื่อวันที่ 2 กันยายน 2554

3
Chief complaint แขนขาข้างขวาอ่อนแรง 2 เดือนก่อนมารพ.

4
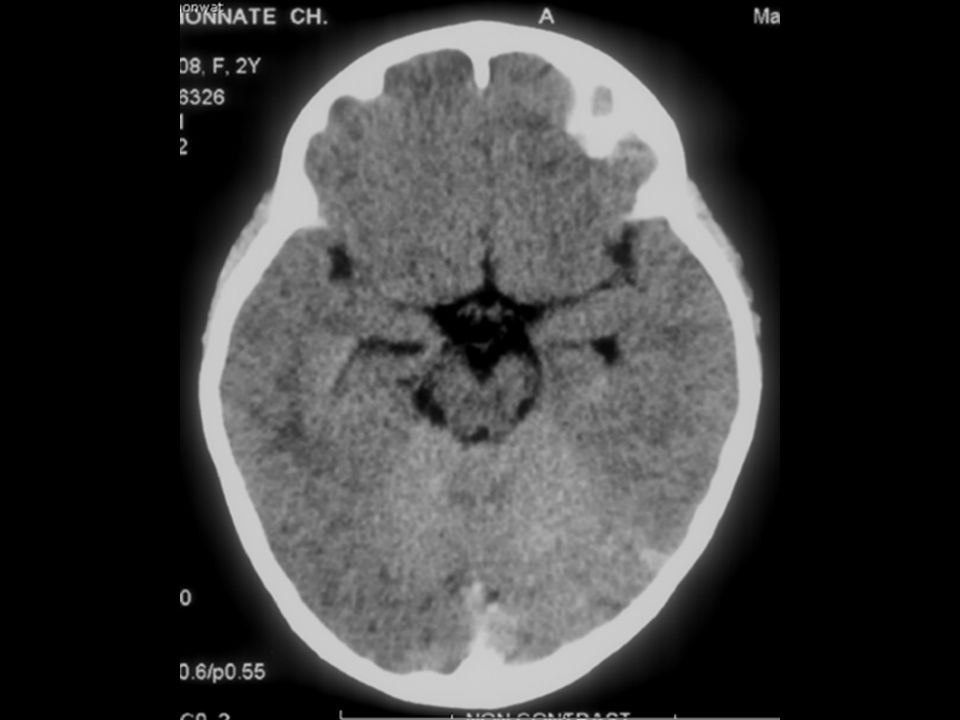
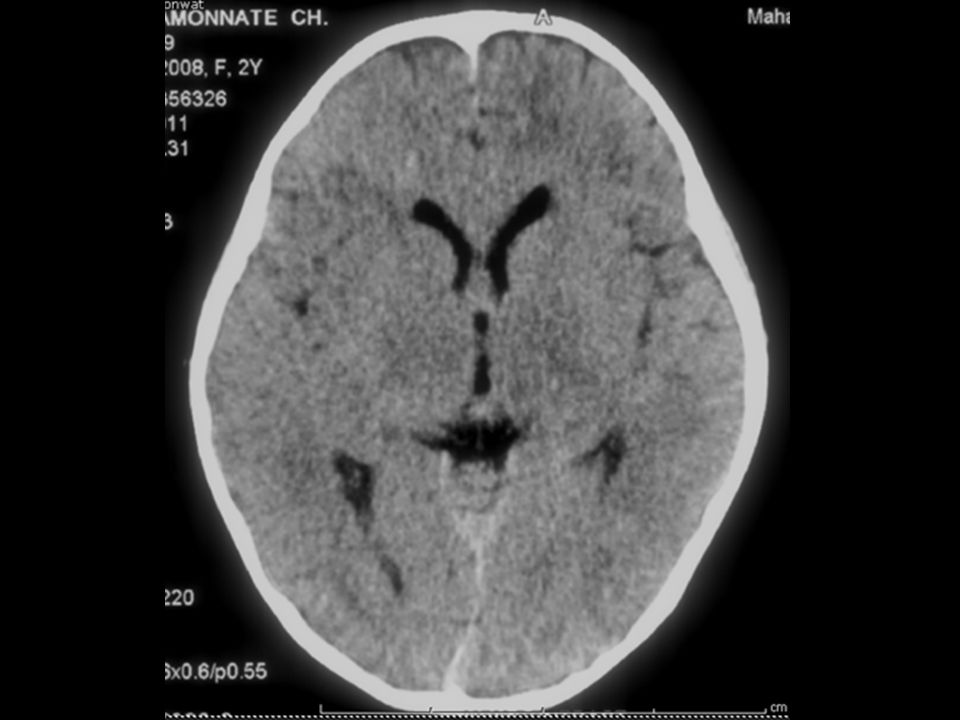
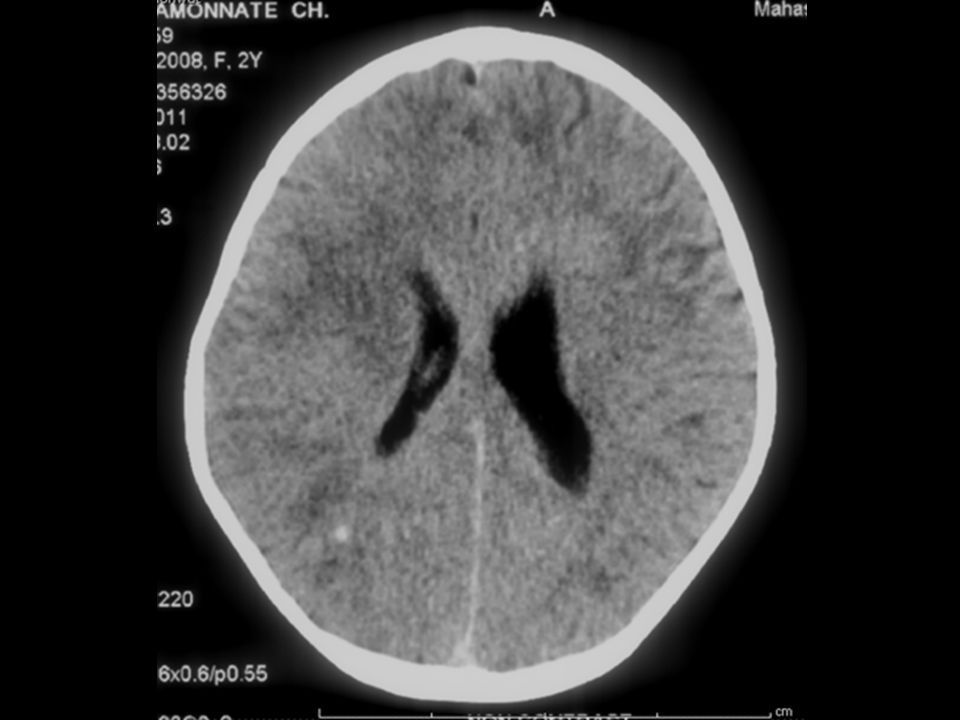
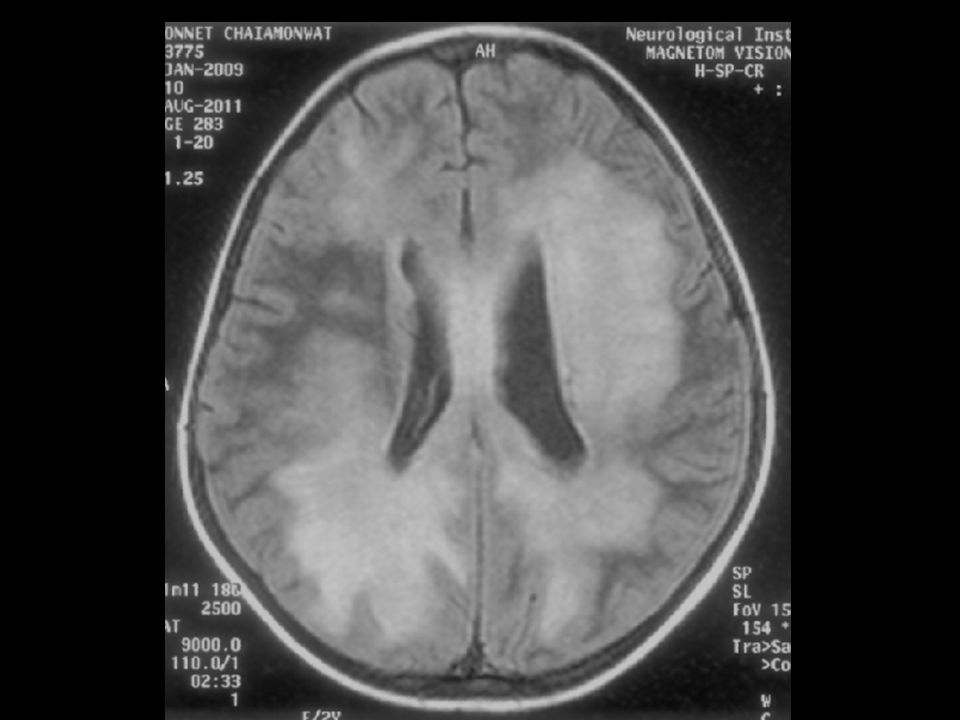
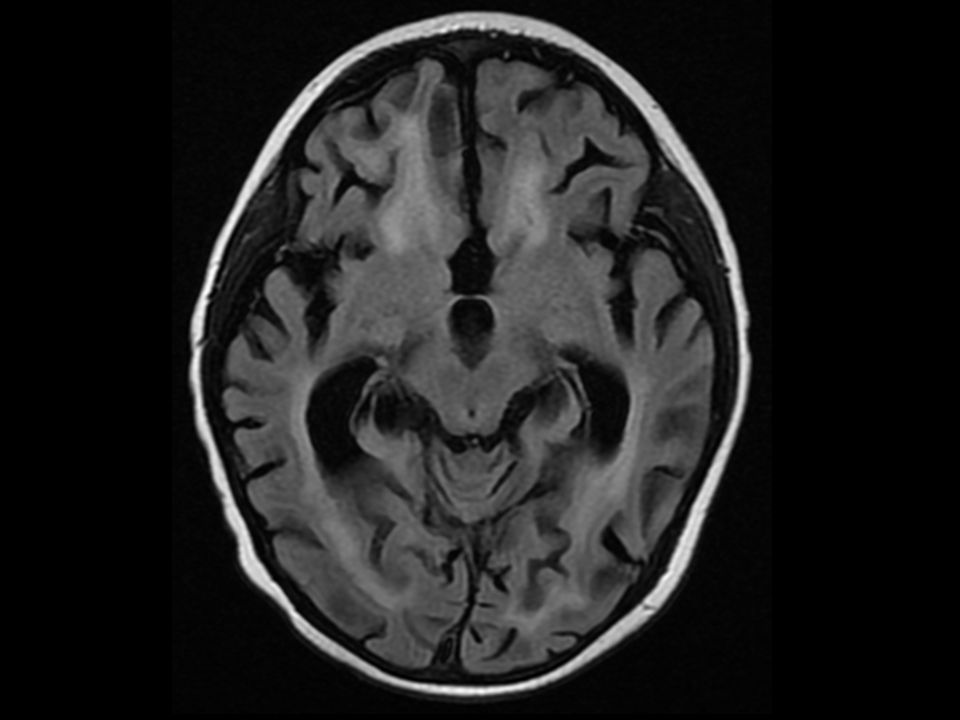
Present illness 2 เดือนก่อนมารพ. มารดาสังเกตว่าผู้ป่วยร้องงอแงบ่อย แขนขวาอ่อนแรง ขยับน้อยลง ต่อมาขาขวาอ่อนแรง ไม่ยอมเดิน ไม่มีไข้ ไปตรวจที่ รพ. ได้รับการตรวจ CT brain พบเป็น subacute hemorrhage Lt parieto-occipital lobe จึงได้รับการรักษาโดยทำกายภาพบำบัด

9
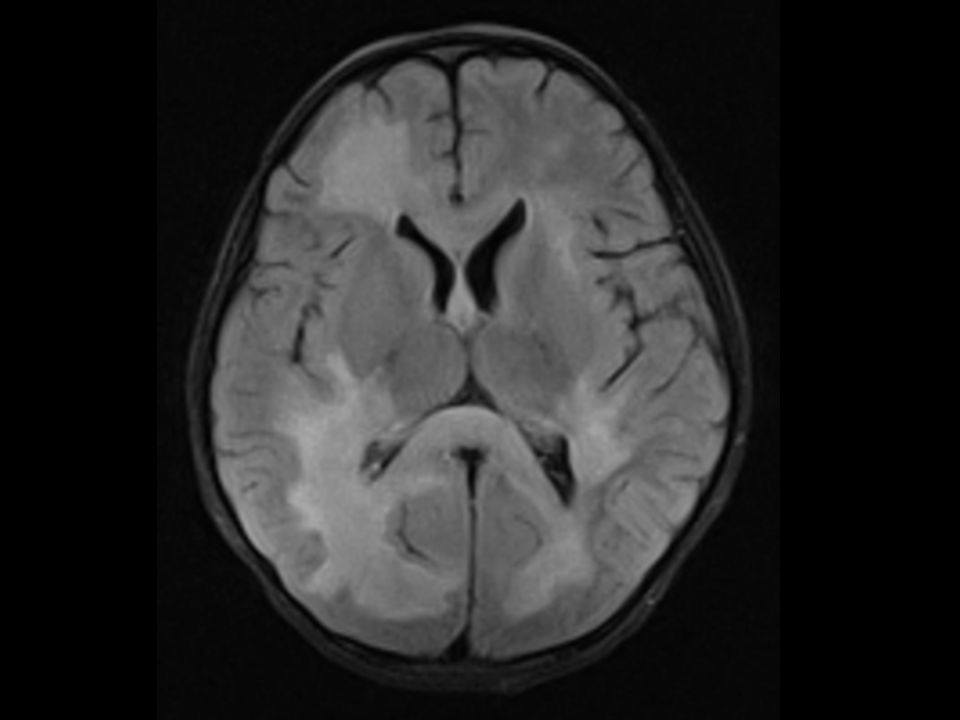
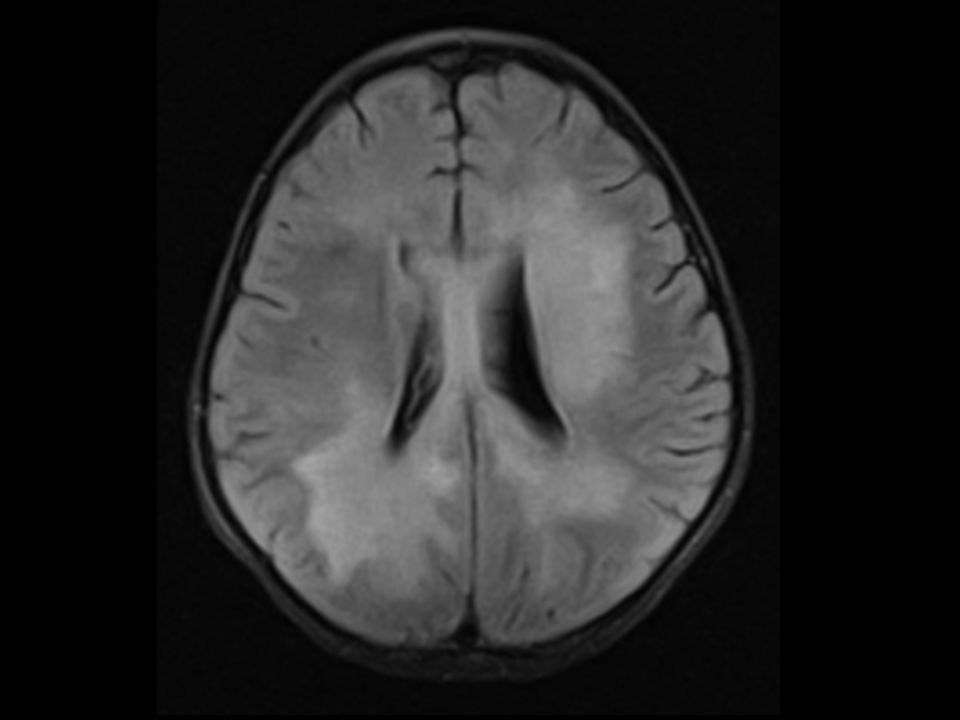
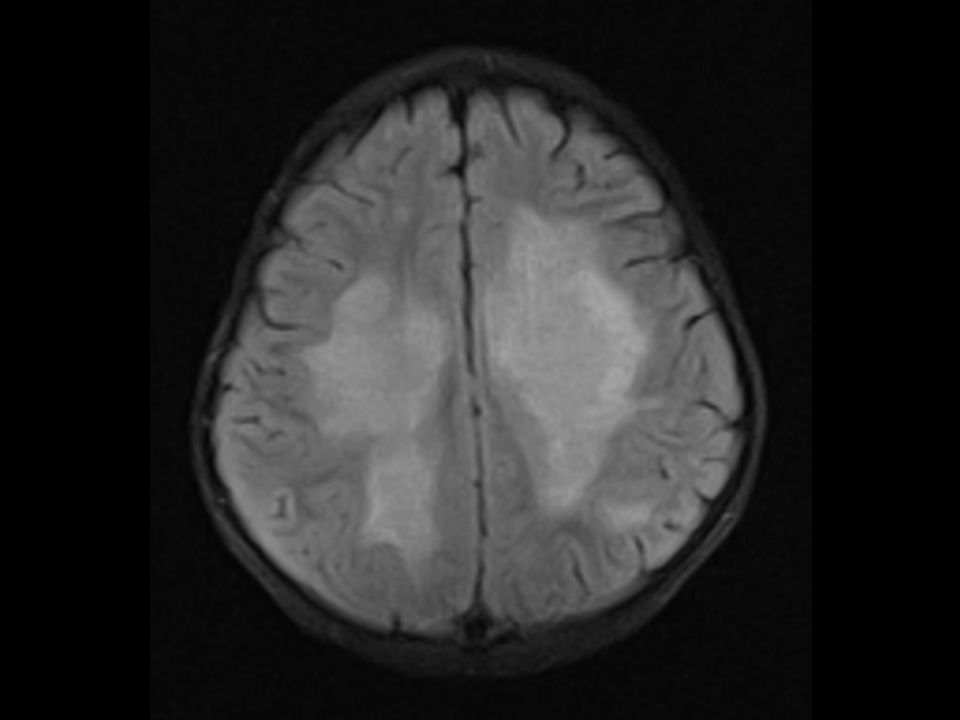
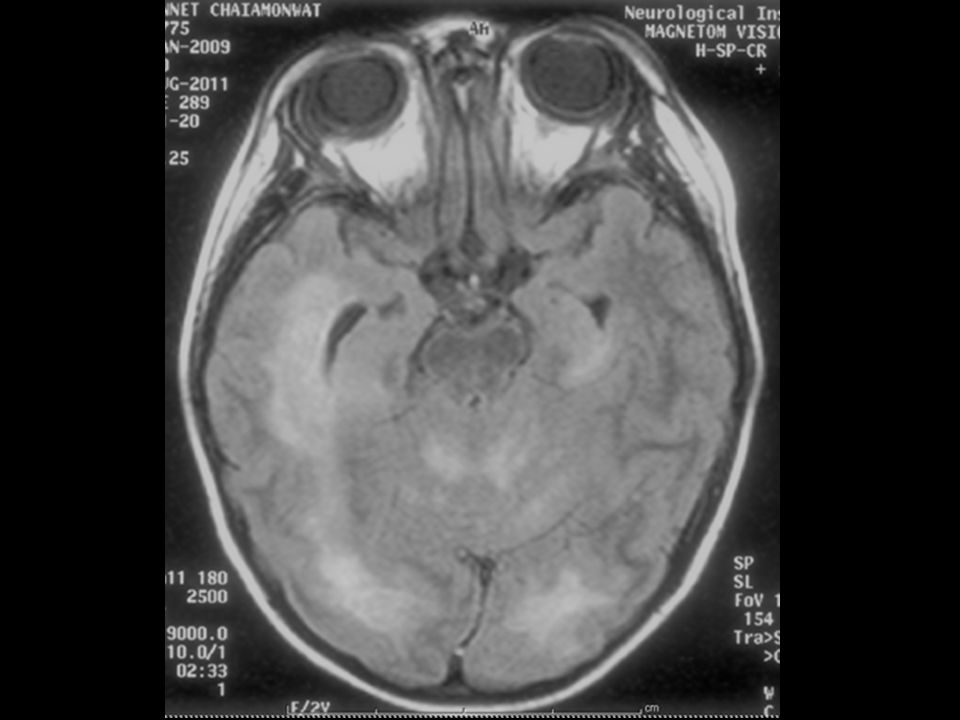
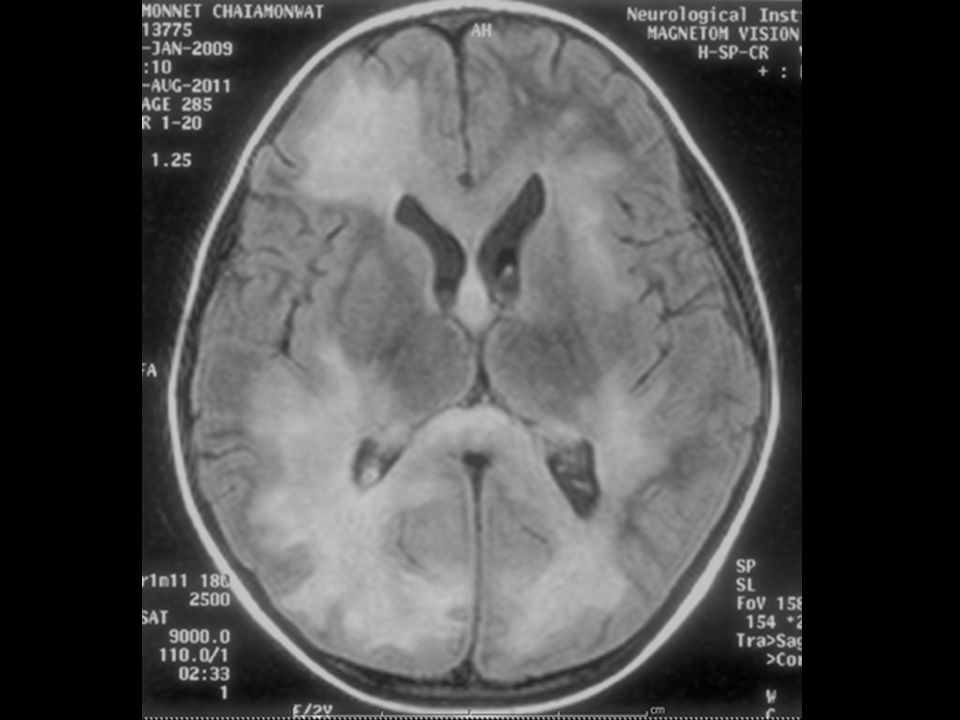
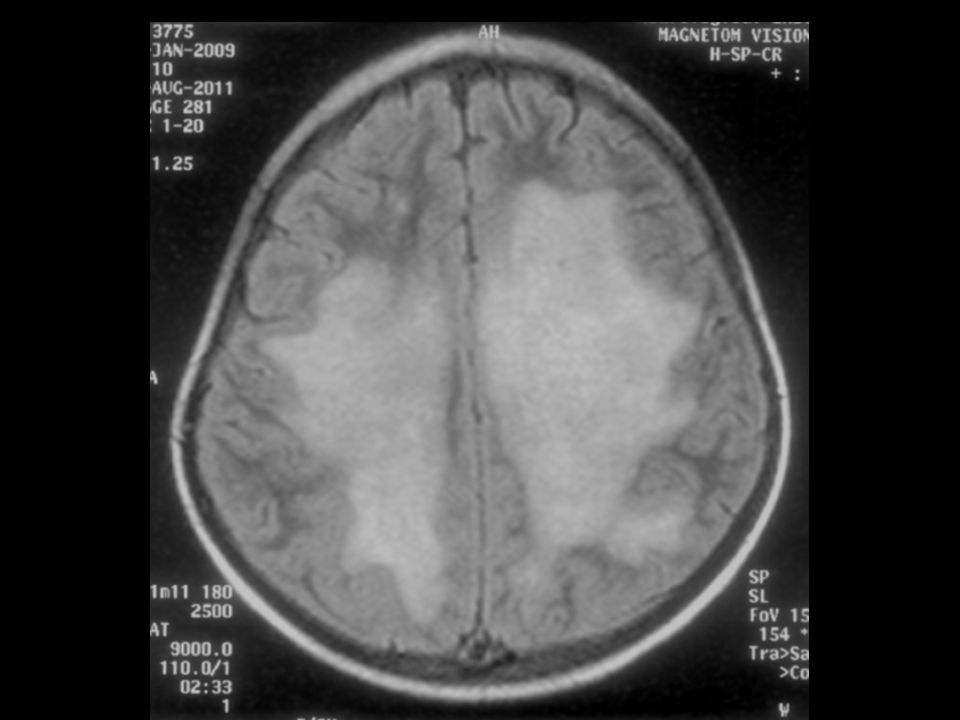
Present illness 2 สัปดาห์ก่อนมารพ. ผู้ป่วยมีแขนและขาข้างขวาอ่อนแรงมากขึ้น และเริ่มมีอาการอ่อนแรงแขนขาข้างซ้ายร่วมด้วย อาการอ่อนแรงเป็นมากขึ้นเรื่อยๆ ไม่พลิกคว่ำ ไม่พูด ลืมตาเป็นพักๆ ต่อมามีอาการเกร็งแขนขาทั้ง 2 ข้าง ไม่มีกระตุก มีไข้ต่ำๆ มารดาได้พาไปรพ.อีกแห่งหนึ่งและได้รับการตรวจ MRI brain พบเป็น white matter lesion และได้รับการตรวจเพิ่มเติมพบมีการติดเชื้อทางเดินปัสสาวะ จึงได้รับการรักษาโดยให้ยาฆ่าเชื้อ อาการอ่อนแรงยังไม่ดีขึ้น

14
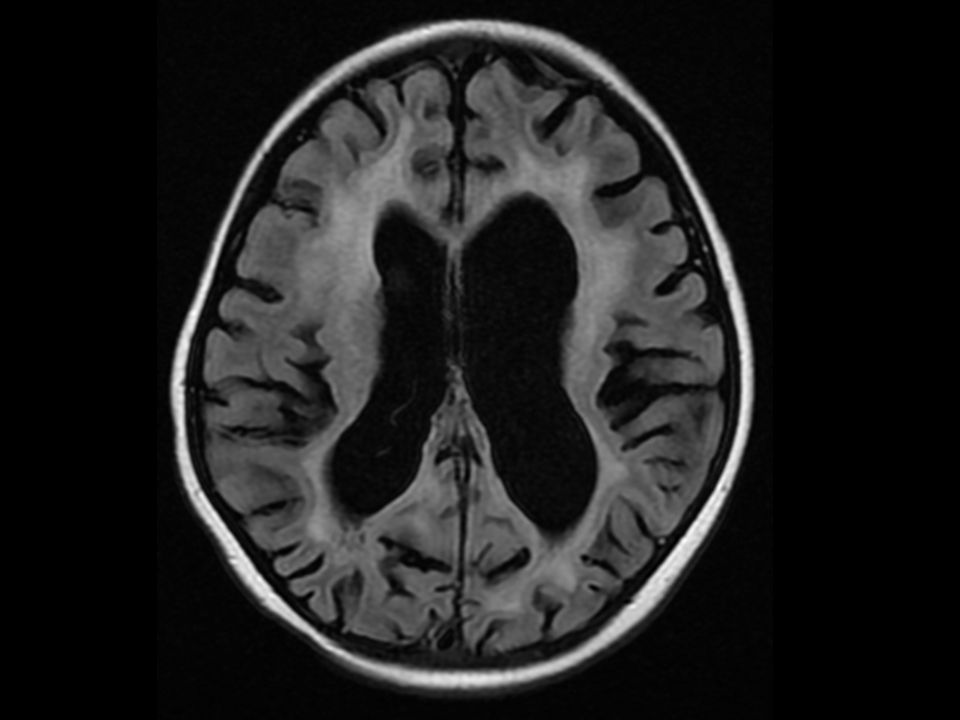
Present illness 3 วันก่อนมารพ. ได้รับการส่งตัวมารักษาต่อที่รพ.ประสาท อาการเกร็งเป็นมากขึ้น ซึมลง ไม่ค่อยลืมตา MRI brain พบว่ามี progression of white matter lesion ผู้ป่วยได้รับการรักษาด้วย methylprednisolone 2 วัน แพทย์ตรวจร่างกายพบตับม้ามโตขึ้น CBC: Hct 28%, WBC 3,550/cumm (N 25%, L 43%, M 27%), platelets 52,000/cumm จึงส่งตัวมารักษาต่อที่ รพ.รามาธิบดี
, platelets 52,000/cumm. จึงส่งตัวมารักษาต่อที่ รพ.รามาธิบดี")
21
Personal history บุตรคนที่ 4/4, V/E due to poor maternal effort, BW 3600 g, no perinatal complication ไม่มีโรคประจำตัว แข็งแรงดีตลอด ไม่มีประวัติแพ้ยาอาหาร พัฒนาการปกติ พูดเป็นประโยค วาดวงกลมได้ ขึ้นบันไดสลับขา วัคซีนครบตามเกณฑ์

22
Family history ปฏิเสธการแต่งงานในเครือญาติ
บุตรชายคนที่ 1 เสียชีวิต อายุ 1 ปี 9 เดือน มีไข้สูง ก้อนที่คอ ตับม้ามโต บุตรชายคนที่ 2 แข็งแรงดี ปัจจุบันอายุ 14 ปี บุตรคนที่ 3 induced abortion GA 3 months

23
Physical Examination V/S: T 37.8°C, PR 120 bpm, RR 40 bpm, BP 96/44 mmHg, BW 14 kg (P50-75th), Ht 95 cm (P50-75th), HC 49 cm (P 50th) GA: a Thai girl, drowsiness, mild pallor, no jaundice, no dysmorphic feature, capillary refill 3 sec HEENT: bilateral cervical LN 0.5 cm, no neck mass, pharynx and tonsil not injected
, Ht 95 cm (P50-75th), HC 49 cm (P 50th) GA: a Thai girl, drowsiness, mild pallor, no jaundice, no dysmorphic feature, capillary refill 3 sec HEENT: bilateral cervical LN 0.5 cm, no neck mass, pharynx and tonsil not injected")
24
Physical Examination CVS: normal S1 S2, no murmur Lung: clear, no adventitious sound, no retraction Abdomen: soft, no distension, liver 3 cm below RCM, liver span 9 cm, spleen 4 cm below LCM Skin : no lesion

25
Physical Examination Nervous system :
drowsiness, pupils 3 mm RTLBE, no stiffness of neck, full EOM by observe, no nystagmus, no facial palsy, corneal reflex positive, gag reflex negative, tongue and uvula in midline, spastic all extremities, motor power: Rt side gr I, Lt side gr II, DTR 3+, BKK: present both sides

26
Investigation 1 2 3 5 4 6 7 8 9 11 12 13 14 10

27
CBC Hb 9.5 g/dL Hct 28.2% WBC 2,930/cumm. PMN 40% Lymph 51% Mono 5%
Atyp L 4% Plt 34,000/cumm. RDW 16.9% MCV 70.5 fL MCH 23.7 pg MCHC 33.7 g/dL Anisocytosis 1+ Microcyte 1+ Hypochromia 1+

28
Coagulogram aPTT 27 sec PT 13 sec INR 1.13 TT 11 sec
Fibrinogen 248 mg/dL

29
Blood chemistry Na 129 mmol/L K 3.2 mmol/L Cl 94 mmol/L
CO mmol/L Inorganic phosphate 3.5 mg/dL Calcium 7.6 mg/dL (correct 8.8) Mg 1.8 mg/dL BUN 10 mg/dL Cr 0.51 mg/dL
 Mg 1.8 mg/dL. BUN 10 mg/dL. Cr 0.51 mg/dL.")
30
Liver function test AST 25 U/L ALT 29 U/L GGT 20 U/L TP 62.6 g/L
Albumin 25.6 g/L ALP 63 U/L TB 0.2 mg/dL DB 0.1 mg/dL

31
CXR

32
Ferritin Ferritin 2,248 ng/mL

33
Viral studies EBV IgG : Positive EBV IgM : Negative
EBV viral load < 100 copies

34
Bone marrow aspiration
Hypercellularity 1+ Adequate in number of megakaryocyte, erythroid, myeloid series No blast No abnormal cell No hemophagocytic activity

35
Bone marrow biopsy Active trilinear hematopoiesis with increase histiocytes with hemaphagocytosis activity No immunophenotypic evidence of increased blasts or non-Hodgkin lymphoma CD68-positive histiocytes are increased

36
Lipid profile TG 328 mg/dL Chol 112 mg/dL LDL 38 mg/dL

37
LDH LDH 164 U/L

38
CSF profile CSF WBC 3 cell/cumm RBC not seen Monocyte 100%
Glucose 58 mg/dL Protein 93.8 mg/dL Blood glucose 104 mg/dL

39
Brain biopsy Dense perivascular lymphohistiocytic infiltration with demyelination CD1a : negative CD3, CD4, CD8, CD20 : Positive CD68 : Positive in reactive histiocytic cell

40
Brain biopsy (1) Perivascular cuffs of mononuclear inflammatory cells
 Perivascular cuffs of mononuclear inflammatory cells")
41
Microglial activation
Brain biopsy (2) Microglial activation
 Microglial activation.")
42
Brain biopsy (3) Infiltrate of foamy histiocytes with reaction astrocytes
 Infiltrate of foamy histiocytes with reaction astrocytes")
43
PRF1 gene mutation analysis
PCR amplification and sequencing analysis of PRF1 gene (exon 2 and 3) Interpretation : The mutation of PRF1 exon 2 or 3 was not identified The PRF1 c.822C>T and c.900C>T which synonymous SNPs
 Interpretation : The mutation of PRF1 exon 2 or 3 was not identified. The PRF1 c.822C>T and c.900C>T which synonymous SNPs.")
44
UNC 13 D (Munc 13-4) Polymorphism or Mutation of UNC13D IVS4-1 or IVS9-1 was not identified c.756_757insAC cause a shift in the reading frame UNC13D c.756_757insAC

45
Post-treatment 1 -week 1-month 3-month Hb (g/dL) 9.4 10.9 12.5 Hct (%) 29 30.9 37.9 WBC (cumm) 2410 9020 9190 Neutrophil (%) 21 13 51 Platelets (cumm) 118000 500000 257000
 Neutrophil (%) Platelets (cumm)")
46
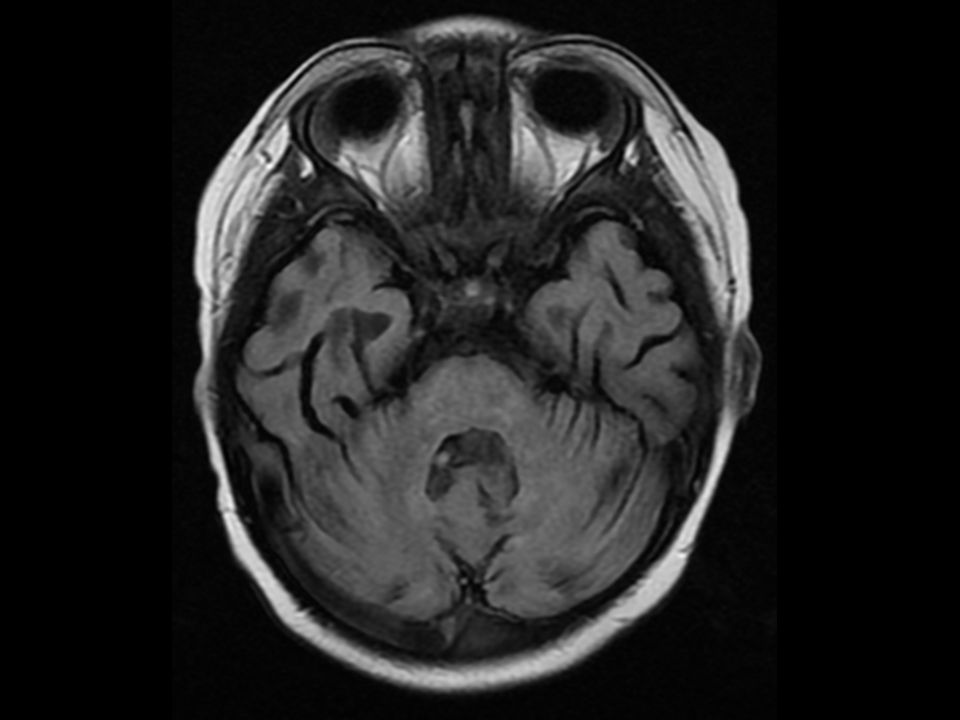
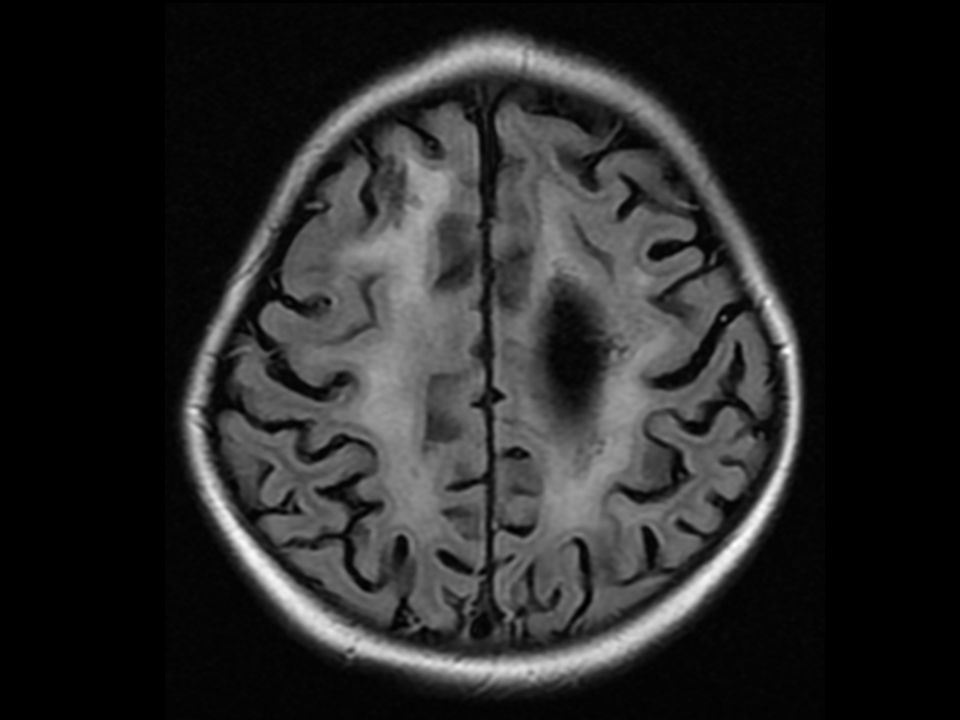
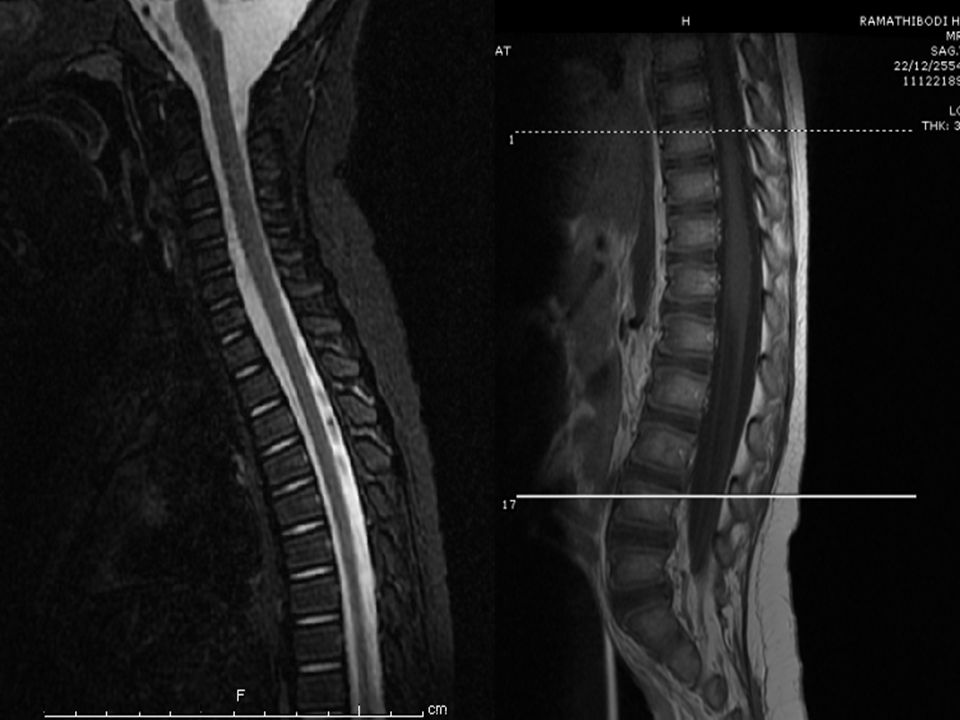
MRI post treatment 3-month
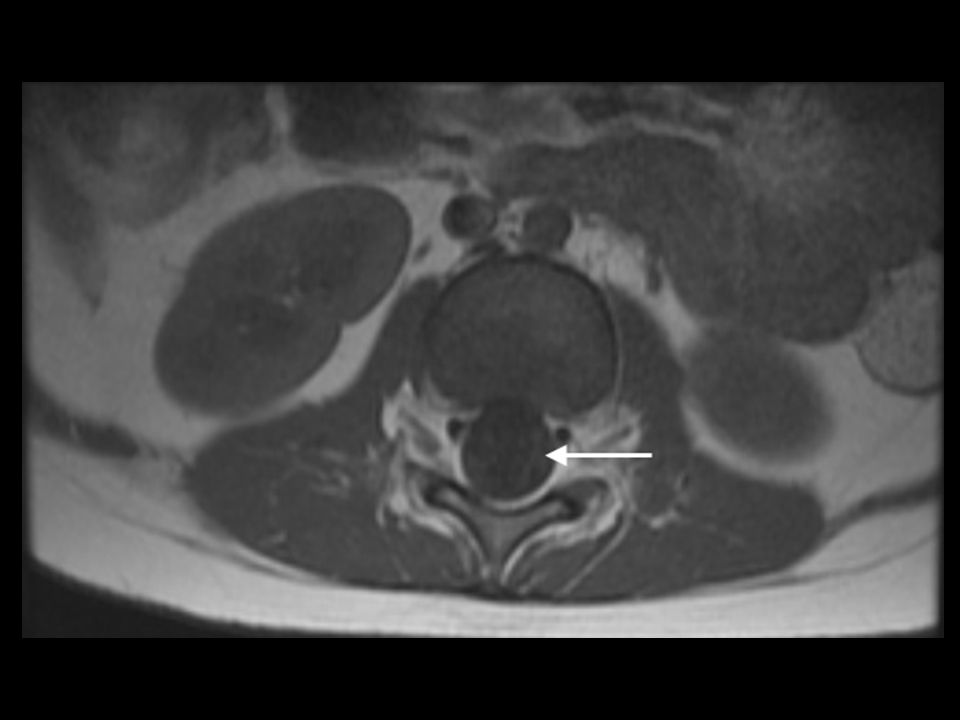
MRI brain Marked decrease white matter lesions which severe white matter volume loss with bilateral ventricles dilatation Increase choline with decrease NAA at residual periventricular lesions without relative hyperperfusion MRI whole spine Remaining intramedullary lesions entire spinal cord but not enhancement Clumping with faint enhancing cauda equina nerve root

53
Method Single center (France) retrospective1981 to 1993
34 patients (19 girls, 15 boys) with HLH 25 patients with family history (consanguinity or siblings affected same syndrome 9 patients without family history, no concomitant infection-induced, recurrence of hemophagocytic syndrome Evaluate : clinical, CSF, neuroradiolological studies E.Haddad, et al. blood Feb;89:
 with HLH. 25 patients with family history (consanguinity or siblings affected same syndrome. 9 patients without family history, no concomitant infection-induced, recurrence of hemophagocytic syndrome. Evaluate : clinical, CSF, neuroradiolological studies. E.Haddad, et al. blood Feb;89:")
54
Results E.Haddad, et al. blood Feb;89:

55
20-80 lymphocytes/µL with protein 50-100 mg/dL
Meningitis 20-80 lymphocytes/µL with protein mg/dL 20 with meningitis (mean age 6.9 months) 9 with neurological symptoms (mean age 16 months) E.Haddad, et al. blood Feb;89:
 9 with neurological symptoms (mean age 16 months) E.Haddad, et al. blood Feb;89:")
56
8/9 with neurological symptoms
Brain imaging 9/20 with meningitis 4 had abnormal : 2 with pericerebral diffuse subdural dilataion, 2 with white matter lesions 8/9 with neurological symptoms Most frequent focal necrosis with parenchyma volume loss and white matter lesions E.Haddad, et al. blood Feb;89:

57
19 patients had severe CNS progression 4 patients repeat imaging
3 with severe brain atrophy 1 with enhance cerebellar white matter and parenchyma loss E.Haddad, et al. blood Feb;89:

58
E.Haddad, et al. blood. 1997 Feb;89:794-800.

59
3 cases perform MRI before and after BMT
7 alive with normal neurological examination, CSF, cognitive development 3 cases perform MRI before and after BMT 2 had normal MRI (pre/post BMT) 1 had white matter lesion before BMT and remain 2 years after BMT E.Haddad, et al. blood Feb;89:
 1 had white matter lesion before BMT and remain 2 years after BMT. E.Haddad, et al. blood Feb;89:")
61
Large cohort of children (n = 193) Originated from 25 countries
Median age at diagnosis 9 months 106 (55%) less than 1 year of age at diagnosis 43/192 (22%) (no data = 1) familial disease Consanguinity 37/186 (20%) cases (no data = 7) 11 patients studied specified viral infections at diagnosis A. Horne, et al. BJH Dec;140:327–335.
 less than 1 year of age at diagnosis. 43/192 (22%) (no data = 1) familial disease. Consanguinity 37/186 (20%) cases (no data = 7) 11 patients studied specified viral infections at diagnosis. A. Horne, et al. BJH Dec;140:327–335.")
62
A. Horne, et al. BJH Dec;140:327–335.

63
Neurological symptoms and relation to abnormal CSF
A. Horne, et al. BJH Dec;140:327–335.

64
CSF 101 patients (52%) abnormal CSF Elevated CSF protein 76/188 (40%)
Elevated cell counts in 79/189 (42%) Abnormal CSF at onset had sequelae compared to 5/61 (8%) patients with normal CSF (P = 0.024) A. Horne, et al. BJH Dec;140:327–335.
 Abnormal CSF at onset had sequelae compared to 5/61 (8%) patients with normal CSF (P = 0.024) A. Horne, et al. BJH Dec;140:327–335.")
65
A. Horne, et al. BJH Dec;140:327–335.

66
Neuroradiology Performed 115/193 patients (60%)
35/115 patients (30%) reported abnormal Generalized cerebral atrophy (n = 16) White matter lesions and demyelination (n = 5) Non-specific inflammatory changes (n = 4), Intracerebral bleeding (n = 2) and brain edema (n = 1) Cerebellar involvement (n=5) A. Horne, et al. BJH Dec;140:327–335.
 reported abnormal. Generalized cerebral atrophy (n = 16) White matter lesions and demyelination (n = 5) Non-specific inflammatory changes (n = 4), Intracerebral bleeding (n = 2) and brain edema (n = 1) Cerebellar involvement (n=5) A. Horne, et al. BJH Dec;140:327–335.")
67
Mortality and CNS involvement
3-year probability of was 56% 67 (61%) transplanted 37 (34%) ‘off-therapy’ 49 patients died before SCT 18 of these (37%) CNS involvement No neurological symptom but abnormal CSF (CNS group 3) A. Horne, et al. BJH Dec;140:327–335.
 transplanted. 37 (34%) ‘off-therapy’ 49 patients died before SCT. 18 of these (37%) CNS involvement. No neurological symptom but abnormal CSF (CNS group 3) A. Horne, et al. BJH Dec;140:327–335.")
68
A. Horne, et al. BJH Dec;140:327–335.

69
Neurological symptoms at follow-up
Transplanted patients 102 patients undergone SCT, 67 (66%) were alive Most common sequelae Neurodevelopmental retardation (n = 7) Epilepsy (n = 4) ADHD (n = 2) Hearing loss (n = 2) minimal cerebral palsy and hemiplegia (n = 1 each) A. Horne, et al. BJH Dec;140:327–335.
 were alive. Most common sequelae. Neurodevelopmental retardation (n = 7) Epilepsy (n = 4) ADHD (n = 2) Hearing loss (n = 2) minimal cerebral palsy and hemiplegia (n = 1 each) A. Horne, et al. BJH Dec;140:327–335.")
71
92 patients with HLH January 2004 to August 2008
82 patients (89%) active viral infection 69/82 patients (75%) EBV infection 9 patients not find any underlying disease None of the patients were offspring of consanguineous marriages or history of siblings affected by same syndrome 82 were only child in the family S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.
 active viral infection. 69/82 patients (75%) EBV infection. 9 patients not find any underlying disease. None of the patients were offspring of consanguineous marriages or history of siblings affected by same syndrome. 82 were only child in the family. S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.")
72
Methods Prior to start therapy, all patients underwent
CSF cytology and biochemical assays Brain CT and/or MRI examination CSF analysis repeated weekly until normalize CT or MRI examinations Repeated at 8-week intervals until treatment stopped Completed therapy every 6 months for at least 1 year

73
RESULTS 43 patients CNS involvement, either clinical, MRI/CT or CSF abnormalities 36 (84%) patients had EBV-HLH No underlying disease found in 5 patients S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.

74
RESULTS 4 : S+R+C 4 : S+R 2 : S+C 6 : R+C 2 : S 3 : C 22 : R
S, symptoms R, neuroradiology C, CSF S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.

75
Neuroradiological Examinations
CT 46 patients, 8 showed abnormalities Calcifications (n=2), atrophy (n=2), demyelination (n=2), edema (n=1), and hemorrhage (n=1) MRI 64 patients, 34 showed abnormalities High signal intensity lesions on T2-weighted and FLAIR MRI images (n=29), atrophy (n=9), hemorrhage (n=5), cerebromalacia (n=4), and calcifications (n=2) S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.
, atrophy (n=2), demyelination (n=2), edema (n=1), and hemorrhage (n=1) MRI 64 patients, 34 showed abnormalities. High signal intensity lesions on T2-weighted and FLAIR MRI images (n=29), atrophy (n=9), hemorrhage (n=5), cerebromalacia (n=4), and calcifications (n=2) S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.")
76
Clinical Manifestations
12 patients neurological symptoms at diagnosis Eleven of these EBV-HLH Seizures (n=10), hemiplegia (n=3), ataxia (n=3), coma (n=2), cranial nerve palsy (n=2) 8 pathological changes in CT/MRI images 6 abnormal CSF S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.
, hemiplegia (n=3), ataxia (n=3), coma (n=2), cranial nerve palsy (n=2) 8 pathological changes in CT/MRI images. 6 abnormal CSF. S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.")
77
Cerebrospinal Fluid Tests
15 patients (16%) CSF abnormalities at onset 11 patients elevated spinal fluid protein 10 patients elevated spinal fluid leukocyte counts S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.
 CSF abnormalities at onset. 11 patients elevated spinal fluid protein. 10 patients elevated spinal fluid leukocyte counts. S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.")
78
CNS Involvement After Start of Therapy
12 patients with neurological symptoms had improved 3 discontinued therapy due to progressive systemic symptoms One patient, presenting with CNS dysfunction preceding systemic HLH disease, improved initially but repeated relapses and progressive CNS symptoms 6 months later 15 patients with CSF abnormalities at diagnosis Normal within 6 weeks of therapy S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.

79
CNS Involvement After Start of Therapy
Neuroradiological abnormalities showed slow recovery rate, Neurological symptoms resolved quickly 36 patients with neuroradiological abnormalities 2 patients showed any improvement 15 patients lost to follow-up, 5 patients still undergoing treatment at the end of study S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.

80
CNS Involvement After Start of Therapy
16 patients followed post-therapy 12 showed some improvement of imaging after 3–12 months 5 completely normal CT/MRI scans at follow-up One progressive changes in the CT/MRI images and relapsed 3 patients CT/MRI findings unchanged S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.

81
CNS Involvement After Start of Therapy
42 patients followed after discontinuation of therapy 21/42 had at least one manifestation of CNS involvement at diagnosis 10/42 recovered completely from CNS involvement 3 patients not improve with radiological findings while CSF analysis and clinical examination normalized S. Yang, et al. Pediatr Blood Cancer 2010;54:408–415.

82
THANK YOU FOR YOUR ATTENTION























 98.08% 100.02% จังหวัด.>")


