ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
PEDIATRIC HEMATOLOGY/ONCOLOGY INTER-HOSPITAL CONFERENCE
16 NOV 2010 King Chulalongkorn Memorial Hospital

2
History 2 ผู้ป่วยเด็กชายไทย อายุ 2 เดือน ภูมิลำเนาเดิมและปัจจุบัน สมุทรปราการ รับไว้ในโรงพยาบาลครั้งที่1 เมื่อ15 มีนาคม 53 ประวัติได้จากใบส่งตัว และมารดา เชื่อถือได้ Chief complaint : ไอ 2 สัปดาห์ก่อนมาร.พ. Present illness : 2 สัปดาห์ก่อนมาร.พ. มีอาการไอแห้ง ไม่ หอบเหนื่อย ไม่มีไข้ ไม่ซึม ปัสสาวะอุจจาระปกติ ไม่มีจ้ำเลือดตามตัว ผิดปกติ ไม่มีสำลัก มีอาการนาน 1 สัปดาห์จึงไปพบแพทย์ที่คลินิกได้ยาแก้ ไอ ยาฆ่าเชื้อไม่ทราบชนิด มารับประทาน 2 วันก่อนมาร.พ. อาการไม่ดีขึ้น ไอมาก แม่สังเกตเวลาทานนมไอ มากขึ้น จึงไป พบแพทย์ที่โรงพยาบาล

3
History แรกรับที่โรงพยาบาล จังหวัดสมุทรปราการ
3 Physical exam: pale, tachypnea. Lungs: crepitation both lungs with subcostal retraction both lungs. Abdomen: Liver1 cm. BRCM , spleen not enlarge Investigation CBC: Hb. 5.9 g/dL Hct. 18.7% MCV 89 fL WBC 15,790/mm3 N50% L37% Mo7% Eo 5% Ba1% Platelet 27,000 /mm3 PBS: anisocytosis 1+, poikilocytosis 1+, microcyte 1+ , tear drop few, decrease platelet. CXR : RUL LUL patchy infiltration Impression : pneumonia and anemia with thrombocytopenia Rx : Ampicillin100 mg/kg/day , erythromycin, PRC10 ml/kg จึงส่งตัวมารักษาต่อที่โรงพยาบาลจุฬา

4
14/3/53

5
Past history ไม่เคยเจ็บป่วยเข้าโรงพยาบาลก่อนหน้านี้
5 Past history ไม่เคยเจ็บป่วยเข้าโรงพยาบาลก่อนหน้านี้ ปฏิเสธประวัติการแต่งงานในเครือญาติ ปฏิเสธสมาชิกในครอบครัวป่วยเป็นโรคเลือด/มะเร็ง ขณะอายุ 4 วัน แม่พาไปกวาดลิ้น หลังจากนั้นลิ้นเป็นแผล ไปคลินิก ได้ยาฆ่า เชื้อมาทานไม่ทราบชนิด หลังจากไม่มีอาการอีก อายุ7วัน มีผื่นแดงที่ขาหนีบ ไปคลินิกบอกว่าเป็นผื่นผ้าอ้อมได้ยามาทา

6
Pediatrics history : Prenatal : มารดาผลเลือดปกติ , serology neg. all
6 Pediatrics history : Prenatal : มารดาผลเลือดปกติ , serology neg. all ระหว่างตั้งครรภ์ ไม่มีไข้ หรือเจ็บป่วย Perinatal : บุตร1/1, birth weight 2,970 gm., term NL ,no complication แรกเกิดมีปัญหา microcephaly head circumference 30 cm (< P3) Postnatal : กินนมแม่ 3 มื้อ/วัน ร่วมกับนมผสม 2 oz. x 8 feeds Immunization : แรกเกิดได้รับ BCG, HBV G&D : ชันคอได้ จ้องมองตา
 Postnatal : กินนมแม่ 3 มื้อ/วัน ร่วมกับนมผสม 2 oz. x 8 feeds. Immunization : แรกเกิดได้รับ BCG, HBV. G&D : ชันคอได้ จ้องมองตา.")
7
Pedigree I II III 72 ปี 63 ปี 42 ปี 47 ปี 21ปี 19ปี 22ปี 42 ปี 40ปี
ไม่ได้ทำงาน ไม่มีโรคประจำตัว อยู่จ.กำแพงเพชร พนง.บบริษัทเครื่องดื่ม ไม่มีโรคประจำตัว อยู่กทม. พนง.บริษัทเครื่องดื่ม ไม่มีโรคประจำตัว อยู่กทม. ไม่ได้ทำงาน ไม่มีโรคประจำตัว อยู่จ.กำแพงเพชร I II 21ปี 19ปี 22ปี 42 ปี 40ปี 38ปี 36ปี 35ปี 34ปี 32ปี ทหาร ไม่มีโรคประจำตัว ไม่ได้ทำงาน ไม่มีโรคประจำตัว อยู่กทม. III ผู้ป่วย 2 mo.

8
Physical examination GA: A Thai male infant active , tachypnea
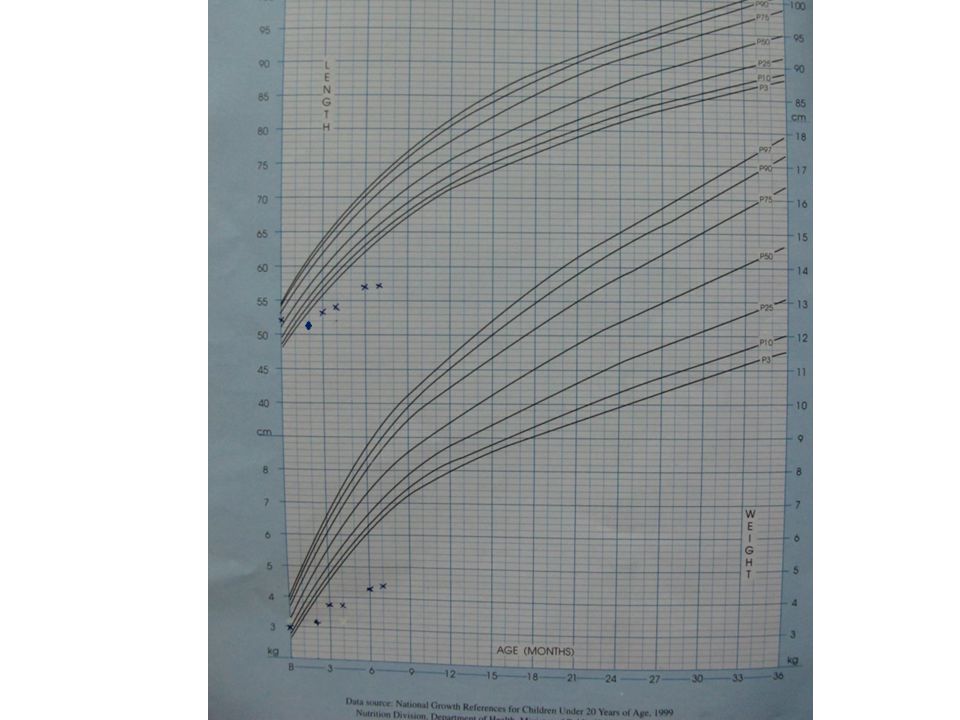
8 GA: A Thai male infant active , tachypnea Measurement : Weight 3.22kg (<P3) ,Length 52 cm (<P3), HC 33cm (<P3) V/S: BT 37.2 ◦c PR110/min BP 86/50 mmHg RR 38/min SpO2 97% Skin: no rash, no petechiae, no ecchymosis BCG scar positive HEENT: AF: 2x2cm., not bulging, not depress ,PF: FT Eye: not pale conjunctiva ,anicteric sclera Ears: intact both TM.
 ,Length 52 cm (<P3), HC 33cm (<P3) V/S: BT 37.2 ◦c PR110/min BP 86/50 mmHg. RR 38/min SpO2 97% Skin: no rash, no petechiae, no ecchymosis. BCG scar positive. HEENT: AF: 2x2cm., not bulging, not depress ,PF: FT. Eye: not pale conjunctiva ,anicteric sclera. Ears: intact both TM.")
9
Physical examination 9 RS : subcostal retraction, medium crepitation both lungs, occasional rhonchi, inspiratory stridor CVS : normal S1S2 ,no murmur Abd : not distension, soft, liver 1 cm BRCM span 6cm, no splenomegaly Musculoskeletal : no edema, capillary refill time<2 sec NS : active, pupil 3 mmRTLBE, equal movement , Brudzinski sign negative, DTR 1+ all extremities.

11
Head circumference 11

12
Problem lists Thrombocytopenia with anemia
12 Thrombocytopenia with anemia Failure to thrive with microcephaly Pneumonia

13
Differential diagnosis
13 Infection Pneumonia Septicemia Congenital infection: ToRCH infection HIV infection Bone marrow disease Congenital bone marrow failure Infiltrative disease

14
Initial investigation (15 มีนาคม 53)
14 CBC post PRC transfusion Hb 9.6 g/dL, Hct 30.2%, MCV 89 fL., RDW 16% WBC 10,610 /mm3 (N 61% L 23.3% Mo 6.1% Eo 3.9% Ba 0.6%) Platelet 39,000/mm3 Reticulocyte count 3.1% Absolute neutrophil count = 6,472/mm3 Absolute lymphocyte count = 2,493/mm3
 Platelet 39,000/mm3. Reticulocyte count 3.1% Absolute neutrophil count = 6,472/mm3 Absolute lymphocyte count = 2,493/mm3.")
15
15

16
16

17
Initial investigation (15 มีนาคม 53)
17 BUN 5 g/dl Cr 0.2 d/dl Electrolyte Na 134 mmol/L K 3.1 mmol/L Cl 105 mmol/L HCO3 26 mmol/L LFT : TB 0.56 mg/dL DB 0.24 mg/dL SGOT 69 U/L, SGPT 49 U/L Alp 117 U/L Alb 2.7 g/L globulin 2.6 g/L TP 5.3 g/L Calcium 9.3 mmol/L

18
CXR 18 15/3/53

19
Investigation 19 KOH preparation at groin : pseudo hyphae and budding yeast cells H/C: no growth Stool occult blood: negative

20
Investigation TORCH titer (15/3/53) Rubella IgG negative
20 TORCH titer (15/3/53) Rubella IgG negative Rubella IgM negative Anti CMV IgG positive ( unit) (cut off 40 unit ) Anti CMV IgM negative Anti HSV IgG negative Anti HSV IgM negative CMV viral load: pending
 Rubella IgG negative. Rubella IgM negative. Anti CMV IgG positive ( unit) (cut off 40 unit ) Anti CMV IgM negative. Anti HSV IgG negative. Anti HSV IgM negative. CMV viral load: pending.")
21
Investigation 21 Anti-HIV : negative

22
Bone marrow aspiration
22 BMA (16/3/2553) The specimen shows hypercellular marrow with mild erythroid and myeloid hyperplasia and normal maturation. Megakaryocytes were increased. Mildly increased mature histiocytes were observed. Conclusions : Increase peripheral destruction of platelet and erythroid series.
 The specimen shows hypercellular marrow with mild erythroid and myeloid hyperplasia and normal maturation. Megakaryocytes were increased. Mildly increased mature histiocytes were observed. Conclusions : Increase peripheral destruction of platelet and erythroid series.")
23
23

24
24

25
25

26
U/S abdomen (18/3/53) 26 Mild splenomegaly size ~ 6.2 cm , normal size of liver , unremarkable otherwise.

27
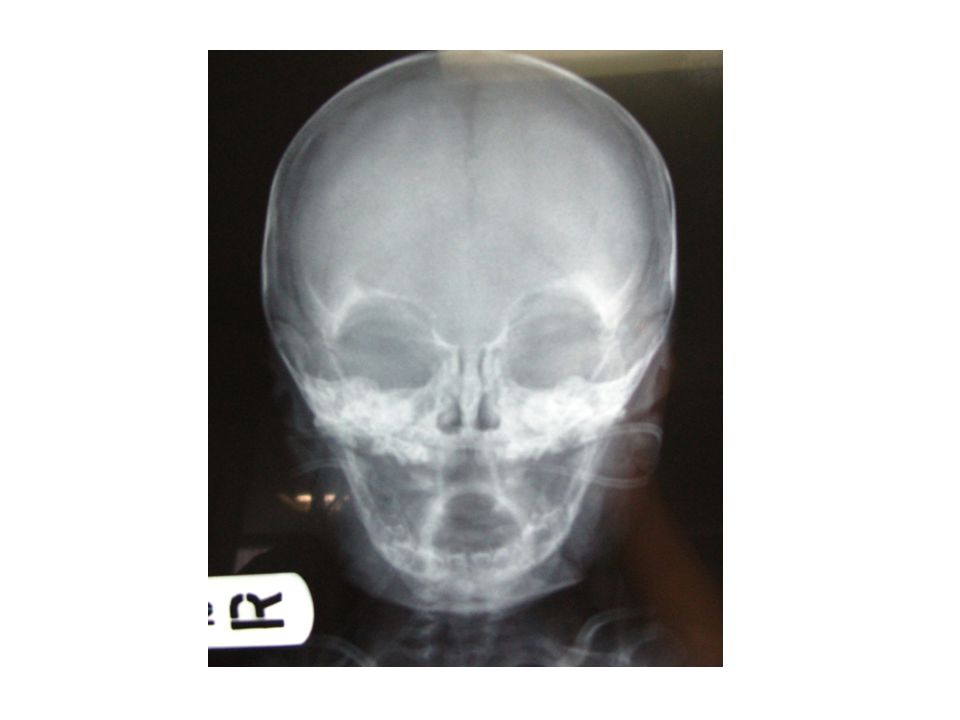
Film lateral + AP skull 27

29
Diagnosis Infection Bone marrow disease x Pneumonia √ Candidiasis √
29 Infection Pneumonia √ Candidiasis √ CMV infection ? Septicemia x HIV infection x Bone marrow disease x Congenital bone marrow failure Infiltrative disease Anemia with thrombocytopenia due to peripheral destruction

30
Treatment Antibiotics: ampicillin 100 mg/kg/day
30 Antibiotics: ampicillin 100 mg/kg/day Platelet transfusion: 1 unit Topical cotrimazole Oxygen support: canula 0.5 LPM

31
Progress note 31

32
Admission day 4 (19/3/53) ผู้ป่วยไข้สูง หายใจเร็วเหนื่อย กินนมลดลง ซึม
32 ผู้ป่วยไข้สูง หายใจเร็วเหนื่อย กินนมลดลง ซึม Diagnosis: pneumonia, respiratory failure with septic shock CBC: Hb 7.9 g/dl Hct25.1% WBC15,790/mm3 (N91% ,L 1%, Mo 3%) Plt 50,000/mm3 ALC 1,579 H/C: E. coli TSC, stool C/S, urine C/S :candida albicans Treatment ETT 5 days Antibiotics: meropenam + fluconazole PLT and LPRC transfusion
 Plt 50,000/mm3 ALC 1,579. H/C: E. coli. TSC, stool C/S, urine C/S :candida albicans. Treatment. ETT 5 days. Antibiotics: meropenam + fluconazole. PLT and LPRC transfusion.")
33
CBC มีนาคม 2553 Date 15 /3 17 /3 19 / 3 20/ 3 WBC (/mm3) 10,610 9,820
15,790 22,590 N (%) 61 84 91 54 L(%) 23.3 8 1 36.9 M(%) 6.1 5 3 E(%) 3.9 Hb (g/dl) 9.6 6 7.9 ▲ 9.2 Hct (%) 30.7 28.2 25 28 Plt (/mm3) 39,000 6,000 50,000 38,000 33
 L(%) M(%) E(%) 3.9. Hb (g/dl) ▲ 9.2. Hct (%) Plt (/mm3) 39,000. 6, , ,")
34
Admission day 10 (25/3/53) Extubation ยังมีไข้ต่ำ ๆ หายใจหอบเท่าเดิม
34 Extubation ยังมีไข้ต่ำ ๆ หายใจหอบเท่าเดิม CBC : Hb 10.7 g/dl Hct 32.8% WBC 6,240/mm3 (N 62% ,L 14% , Mo 5%) Plt 74,000/mm3 CMV viral load 52,800 copies/ml Treatment: O2 Box 10 LPM Gangcyclovir 5 mg/kg/dose q12hr(25/3-12/5) LPRC 10 ml/kg. Plt. Conc. 1unit
 Plt 74,000/mm3. CMV viral load 52,800 copies/ml. Treatment: O2 Box 10 LPM. Gangcyclovir 5 mg/kg/dose q12hr(25/3-12/5) LPRC 10 ml/kg. Plt. Conc. 1unit.")
35
CBC มีนาคม 2553 Date 15 /3 17 /3 19 / 3 20/ 3 21/ 3 22/ 3 24/ 3 25/ 3
WBC (/mm3) 10,610 9,820 15,790 22,590 7,700 5,460 5,800 6,290 N (%) 61 84 91 54 74 56.7 60 62 L(%) 23.3 8 1 36.9 17 27.8 27 14 M(%) 6.1 5 3 4 10 E(%) 3.9 5.5 Hb (g/dl) 9.6 6 7.9 ▲ 9.2 11.5 10.7 Hct (%) 30.7 28.2 25 28 30.4 30.6 34.8 32.8 Plt (/mm3) 39,000 6,000 50,000 38,000 98,000 (CCI 21,000) 28,000 53,000 11,000 74,000 35
 10,610. 9, , ,590. 7,700. 5,460. 5,800. 6,290. N (%) L(%) M(%) E(%) Hb (g/dl) ▲ Hct (%) Plt (/mm3) 39,000. 6, , , ,000. (CCI 21,000) 28, , , ,")
36
Problem lists Thrombocytopenia and anemia Failure to thrive
36 Thrombocytopenia and anemia Failure to thrive Microcephaly Pneumonia Systemic candida infection Infection : CMV

37
progress Date PE investigation Management
31/3/53 (day 16) มีไข้ต่ำ ๆ เหนื่อยมากขึ้น ต่อมาถ่ายเหลวเป็น Melena ปริมาณมาก V/S: BT 37.5 C RR 60 /min BP 64/37 mmHg PR 150/min Lung: subcostal retraction, coarse crepitation CBC : Hb 7.1 g/dl Hct 21.3% WBC 8,250 /mm3 (N 58 , L 34.3 , Mo 3) Plt 117,000/mm3 Central line pus c/s : A. baumanii Stool Rota virus antigen : Positive TSC :S. maltophilia H/C : NG Anti CMV IgG positive Anti CMV IgM positive CMV viral load 79,800 Transfer to PICU on ETT* 3 days - Vancomycin - Ciprofloxin Gangcyclovir - LPRC 10 ml/kg - Platelet 1U progress 37 Rota diarrhea with central line infection with hypovolemic and septic shock
 มีไข้ต่ำ ๆ เหนื่อยมากขึ้น ต่อมาถ่ายเหลวเป็น Melena ปริมาณมาก. V/S: BT 37.5 C RR 60 /min. BP 64/37 mmHg. PR 150/min. Lung: subcostal retraction, coarse crepitation. CBC : Hb 7.1 g/dl Hct 21.3% WBC 8,250 /mm3. (N 58 , L 34.3 , Mo 3) Plt 117,000/mm3. Central line pus c/s : A. baumanii. Stool Rota virus antigen : Positive. TSC :S. maltophilia. H/C : NG. Anti CMV IgG positive. Anti CMV IgM positive. CMV viral load 79,800. Transfer to PICU. on ETT* 3 days. - Vancomycin. - Ciprofloxin. Gangcyclovir. - LPRC 10 ml/kg. - Platelet 1U. progress. 37. Rota diarrhea with central line infection with hypovolemic and septic shock.")
38
CBC มีนาคม 2553 Date 15 /3 17 /3 19 / 3 20/ 3 21/ 3 22/ 3 24/ 3 25/ 3
29/ 3 30/ 3 31/ 3 WBC (/mm3) 10,610 9,820 15,790 22,590 7,700 5,460 5,800 6,290 9,520 7,890 8,250 N (%) 61 84 91 54 74 56.7 60 62 71 48 58.7 L(%) 23.3 8 1 36.9 17 27.8 27 14 22 42 34.3 M(%) 6.1 5 3 4 10 E(%) 3.9 5.5 2 Hb (g/dl) 9.6 6 7.9 ▲ 9.2 11.5 10.7 9 7.6 7 Hct (%) 30.7 28.2 25 28 30.4 30.6 34.8 32.8 26.8 24.4 21 Plt (/mm3) 39,000 6,000 50,000 38,000 28,000 53,000 11,000 74,000 24,000 21,000 77,000 38
 10,610. 9, , ,590. 7,700. 5,460. 5,800. 6,290. 9,520. 7,890. 8,250. N (%) L(%) M(%) E(%) Hb (g/dl) ▲ Hct (%) Plt (/mm3) 39,000. 6, , , , , , , , , ,")
39
31 /3/53

40
progress Date PE investigation Management 2-27/4/53
Extubationได้ ถ่ายลดลงเหนื่อยน้อยลง V/S: stable Lungs : crepitation both lungs Abd : soft , mild distension , active bowel sound Skin : petechial CBC Continue ganciclovir Oxygen canular 0.5 LPM PLT and PRC transfusion progress 40

41
Ganciclovir start 25/3/53 Date 15/3/53 23/3/53 29/3/53 31/3/53 19/4/53
41 Date 15/3/53 23/3/53 29/3/53 31/3/53 19/4/53 20/4/53 CMV viral load 52,800 79,800 13,300 4,680 CMV IgM neg pos CMV IgG Platelet 44,000 24,000 77,000 57,000 Ganciclovir start 25/3/53

42
Date 1 /4 2 /4 3 /4 4 /4 5 /4 6 /4 7 /4 10 /4 11 /4 16 /4 18 /4 22 /4 26 /4 WBC (/mm3) 5,430 6,040 10,840 8,140 7,420 5,230 5,280 5,550 7,910 11,870 7,710 4,310 5,860 N (%) 46 47 62 57.3 52 43 40 51 64 53 85 48.9 L(%) 45 30 32 37 26 50 10 36.9 M(%) 8 6 4 4.5 5 3 2 10.5 E(%) 1 Hb (g/dl) 8.8 9 7.7 7.4 ▲ 8.6 7.8 7 9.8 9.7 7.3 8.7 Hct (%) 25.7 27.5 28 24.2 23.3 25.4 24.6 22 29.8 21.3 24.7 Plt /mm3 177,000 93,000 54,000 27,000 19,000 109,000 80,000 12,000 59,000 11,000 57,000 26,000 22,000
 5,430. 6, ,840. 8,140. 7,420. 5,230. 5,280. 5,550. 7, ,870. 7,710. 4,310. 5,860. N (%) L(%) M(%) E(%) 1. Hb (g/dl) ▲ Hct (%) Plt /mm3. 177, , , , , , , , , , , , ,000.")
43
2nd Bone marrow aspiration 19/4/53
43 Hypercellular marrow ,increase of megakaryocyte peripheral destruction

44
progress Thrombocytopenia from immune process Date PE investigation
Management 1-27 พ.ค. 53 ที่รพ.แห่งหนึ่ง : อาการทั่วไปดีขึ้น กินได้ ไม่มีไข้ ไม่เหนื่อย Skin : erythematous papule at both cheeks , generalized petechiae at face , extremities , buccal mucosa Abd : soft , liver 3 cm BRCM , spleen 2cmBLCM 3/5/53: CMV viral load 1650 copies/ml 12/5/53 = 3120 copies/ml eye and hearing exam: normal 3/5/53 BMA: Normal cellular for age, increased megakaryocyte, normal myeloid and erythroid series, no blast, no histiocyte เคยได้เกร็ดเลือด -> CCI at 1 hr. =1,840 Continue Ganciclovir รวม 7 wks. off -IVIG 5 gm (4,6/5/53) no response -Platelet and PRC transfusion -Prednisolone 1MKday(start 17/5/53) progress 44 Thrombocytopenia from immune process
 no response. -Platelet and PRC transfusion. -Prednisolone 1MKday(start 17/5/53) progress. 44. Thrombocytopenia from immune process.")
45
progress Date PE investigation Management
CBC ก่อน refer กลับโรงพยาบาลจุฬา (23/5/53) Hb 11.2 g/dl Hct 30.7% MCV 81 fL WBC 10,500 /mm3 (N 42% L43% Mo 13% E 2%) Platelet 33,000/mm3 MPV 8 fL 27/5/53 รับ refer กลับมาโรงพยาบาลจุฬา CMV viral load: 57,600 copies/ml. 14/6/53 CMV viral load 5, 850 copies/ml Re-start Gangcyclovir Prednisolone 1.5 mg/kg/day progress 45
 Hb 11.2 g/dl Hct 30.7% MCV 81 fL. WBC 10,500 /mm3 (N 42% L43% Mo 13% E 2%) Platelet 33,000/mm3 MPV 8 fL. 27/5/53. รับ refer กลับมาโรงพยาบาลจุฬา. CMV viral load: 57,600 copies/ml. 14/6/53. CMV viral load 5, 850 copies/ml. Re-start Gangcyclovir. Prednisolone 1.5 mg/kg/day. progress. 45.")
46
46

47
progress ฝ้าขาวที่ลิ้น และผื่นที่ก้น มีไข้ หอบเหนื่อย
Date PE investigation Management 3/6/53 28/6/53 ฝ้าขาวที่ลิ้น และผื่นที่ก้น มีไข้ หอบเหนื่อย Lungs :tachypnea, mild subcostal retraction KOH: positive CBC : Hb 8 g/dl Hct 24% WBC8,770/ mm3 (N29% L 60% Mo3.5% Eo7.5%) Plt 48,000/mm3 H/C : NG CXR Nystatin oral qid Cotrimazole cream Start Fluconazole 6 MKday x 7day -IVIG 2.5 gm. (3/6/53) -On O2 box 5 LPM -Meropenam - LPRC progress 47 Oral candidiasis and skin candidiasis Pneumonia
 Plt 48,000/mm3. H/C : NG. CXR. Nystatin oral qid. Cotrimazole cream. Start Fluconazole. 6 MKday x 7day. -IVIG 2.5 gm. (3/6/53) -On O2 box 5 LPM. -Meropenam. - LPRC. progress. 47. Oral candidiasis and skin candidiasis. Pneumonia.")
48
CXR 48

49
CBC เดือน พ.ค.-มิ.ย. 49 IVIG 2.5 gm. 3/6/53 Date 27/5 31/5 7/6 12/6
20/6 26/6 28/6 1/7 8/7 9/7 WBC (/mm3) 14,500 7,760 8,730 6,610 7,120 6,900 8,870 4,730 7,780 6,370 N (%) 78 71 65 53 48 48.4 29 57 60 47 L(%) 15 5 38 43 42 27 30 M(%) 3 13 4 6 3.5 E(%) 11 7.5 10 Hb (g/dl) 10.2 10.4 9 8 ▲ 6.6 10.5 9.4 Hct (%) 26.8 25 19 24 31 28.2 27.3 Plt /mm3 13,000 21,000 22,000 9,000 11,000 91,000 48,000 8,000 122,000 70,000 IVIG 2.5 gm. 3/6/53
 14,500. 7,760. 8,730. 6,610. 7,120. 6,900. 8,870. 4,730. 7,780. 6,370. N (%) L(%) M(%) E(%) Hb (g/dl) ▲ Hct (%) Plt /mm3. 13, , ,000. 9, , , ,000. 8, , ,000. IVIG 2.5 gm. 3/6/53.")
50
CMV viral load and platelet count
50 23/3 29/3 31/3 19/4 20/4 3/5 12/5 31/5 14/6 28/6 CMV viral load 52,800 79,800 13,300 4,680 1,650 3,120 57,600 5,850 688 Anti-CMV IgG pos Anti-CMV IgM neg Pos (0.4) (0.6) Platelet 11,000 24,000 77,000 57,000 26,000 - 13,000 48,000 Ganciclovir (23/3-12/5) Re-start 31/5
 (0.6) Platelet. 11, , , , , , ,000. Ganciclovir (23/3-12/5) Re-start 31/5 ")
51
CMV viral load and platelet count
51 12/7 22/7 2/8 16/8 8/10 19/10 27/10 CMV viral load 2,160 1,380 833 1,120 900 5,320 5,190 Anti-CMV IgG Anti-CMV IgM Platelet 25,000 22,000 13,000 5,000 33,000 6,000 Ganciclovir (31/5-25/8)
")
52
15/3/ /3/ /3/53 Pneumonia Respiratory failure Systemic fungal with septic shock infection 25/3/ /3/ /4/53 CMV infection Rota diarrhea +Pneumonia Phlebitis lt.foot 27/5/ /6/ /6/53 CMV infection Oral candidiasis Pneumonia Skin candidiasis

53
Problem lists Multiple infection CMV infection
53 Multiple infection CMV infection Recurrent pneumonia with respiratory failure with sepsis Systemic candida infection Persistent Thrombocytopenia Eczema

54
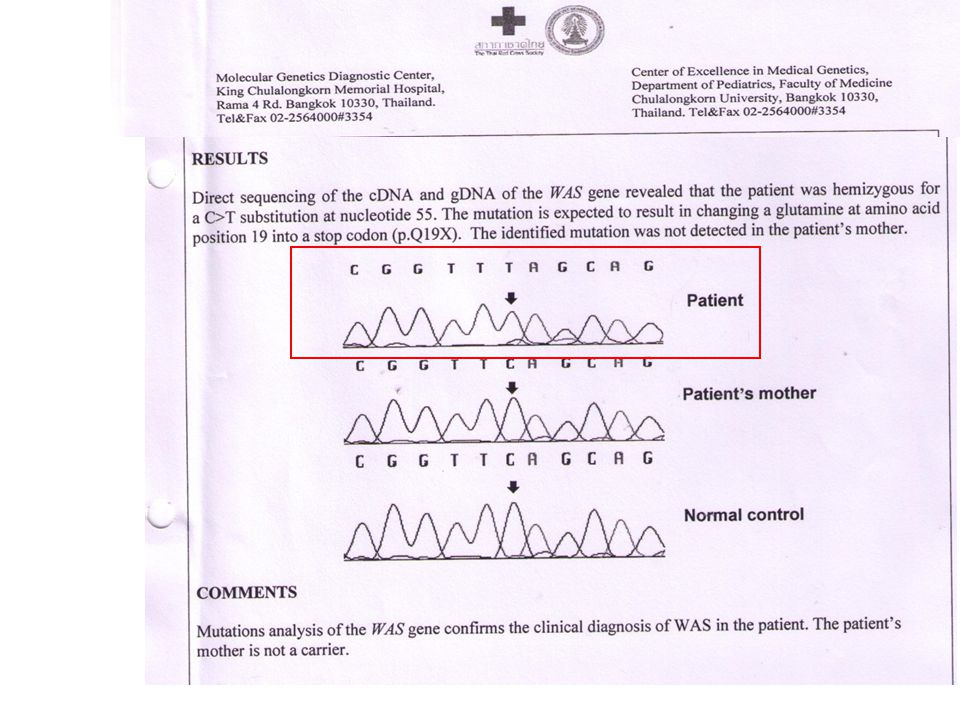
IMMUNODEFICIENCY ∞ WISKOTT-ALDRICH SYNDROME

55
Investigation Complete blood count
55 Complete blood count Absolute lymphocyte count = 2,493 /mm3 Absolute neutrophil count = 6,472 /mm3 Platelet count =39,000 MPV = 7 fL

56
Screening test for B-cell defects
56 Screening test for B-cell defects IgG 1140 (normal 340 +/- 119) IgM 59.1 (normal 30 +/- 11) IgA 113 (normal 21 +/- 13) Total IgE 3,750 (<15)
 IgM 59.1 (normal 30 +/- 11) IgA 113 (normal 21 +/- 13) Total IgE 3,750 (<15)")
57
Screening test for T-Cell defect
57 Screening test for T-Cell defect Absolute lymphocyte count = 2,493 /mm3 Candida albican intradermal skin test positive PHA : impair T-cell function Screening test for phagocytic cell defects Absolute neutrophil count = 6,472 Respiratory burst assay : DHR assay normal Screening test for complement deficiency CH50 =14.6 (19-40 U/ml)
")
58
Flow cytometry %CD3 (Total T lymphocyte) 79% (55-78%)
58 Flow cytometry %CD3 (Total T lymphocyte) 79% (55-78%) %CD4 (Helper/inducer T lymphocyte)11% (21-64 %) %CD8 (Suppressor/cytotoxic T lymphocyte) 57% (16-35%) %CD 19 (B cell) 2% ( ) %CD 56 (NK cell) 18% (10.6 +/- 5.4)
 79% (55-78%) %CD4 (Helper/inducer T lymphocyte)11% (21-64 %) %CD8 (Suppressor/cytotoxic T lymphocyte) 57% (16-35%) %CD 19 (B cell) 2% ( ) %CD 56 (NK cell) 18% (10.6 +/- 5.4)")
59
Combine T-cell and B-cell defect

60
Combine T-cell and B-cell defect
60 Combine T-cell and B-cell defect Primary immune defect Severe combined immunodeficiency (SCID) Ataxia-Telangiectasia syndrome (AT) Wiskott-Aldrich syndrome (WAS) Reticular dysgenesis Secondary immune defect CMV infection
 Ataxia-Telangiectasia syndrome (AT) Wiskott-Aldrich syndrome (WAS) Reticular dysgenesis. Secondary immune defect. CMV infection.")
61
Suspected combine T-Cell and B-Cell defect Persistent thrombocytopenia
61 Suspected combine T-Cell and B-Cell defect Persistent thrombocytopenia Eczema Wiskott-Aldrich syndrome (WAS)
")
63
63

64
Wiskott-Aldrich syndrome
64 1st described by Wiskott in 1937 and was further characterized by Aldrich in 1954. 1 in 250,000 live male births X-linked recessive immunodeficiency disorder characterized by the triad of recurrent bacterial sinopulmonary infections eczema (atopic like dermatitis) bleeding diathesis caused by thrombocytopenia and platelet dysfunction. Pediatr. Dec 1994;125(6 Pt 1):876-85
 bleeding diathesis caused by thrombocytopenia and platelet dysfunction. Pediatr. Dec 1994;125(6 Pt 1):")
65
Wiskott-Aldrich syndrome
65 only 30% of patients with the syndrome have the classic triad 90% of patients have manifestations of thrombocytopenia at presentation 20% have only hematologic abnormalities 5% have only infectious manifestations, Mol There. May 2008;16(5):
:")
66
Wiskott-Aldrich syndrome
66 Wiskott-Aldrich syndrome gene localized to Xp consists of 12 exons encode a 502 amino acid (53 kD) protein Wiskott– Aldrich syndrome protein (WASP) WASP signal transduction and regulates actin filament assembly explains the abnormalities in platelet and lymphocyte cytoskeleton and signaling. J Leukoc Biol. Jun 2005;77(6):993-8.
 protein Wiskott– Aldrich syndrome protein (WASP) WASP. signal transduction and regulates actin filament assembly. explains the abnormalities in platelet and lymphocyte cytoskeleton and signaling. J Leukoc Biol. Jun 2005;77(6):")
67
Clinical manifestations
67 The first clinical signs are petechiae and ecchymosis of the skin and oral mucosa and bloody diarrhea. One series of 154 patients found petechiae or purpura in 78% serious GI bleeding (hematemesis or melena) in 28% epistaxis in 16% intracranial bleeding in 2% of patients. J Pediatr. Dec 1994;125(6 Pt 1):
 in 28% epistaxis in 16% intracranial bleeding in 2% of patients. J Pediatr. Dec 1994;125(6 Pt 1):")
68
Hematologic Findings in WAS
68 Thrombocytopenia (platelet count 10,000–100,000/mm3); Microthrombocytes; low mean platelet volume (MPV).(This is not obvious in the newborn and the MPV is unreliable when the platelet count is low.) Platelets have abnormal aggregation in response to agonists such as ADP, epinephrine and collagen. Platelets have reduced platelet survival to half normal. Ineffective megakaryocytopoiesis reflected by a platelet turnover 25% that of normal megakaryocyte mass.
; Microthrombocytes; low mean platelet volume (MPV).(This is not obvious in the newborn and the MPV is unreliable when the platelet count is low.) Platelets have abnormal aggregation in response to agonists such as ADP, epinephrine and collagen. Platelets have reduced platelet survival to half normal. Ineffective megakaryocytopoiesis reflected by a platelet turnover 25% that of normal megakaryocyte mass.")
69
Hematologic Findings in WAS
69 Anemia (due to blood loss). Leukocytosis (due to infection). Normal or increased megakaryocytes.
. Leukocytosis (due to infection). Normal or increased megakaryocytes.")
70
70 Normal platelets Small platelets

71
Other Manifestations Autoimmune manifestations Hemolytic anemia
71 Autoimmune manifestations Hemolytic anemia Vasculitis Inflammatory bowel disease Glomerulonephritis Arthritis Malignancies: adolescents, young adults The most common malignancy is non- Hodgkin lymphoma.

72
Diagnostic tests; immunologic
72 Decrease CD3, CD4, CD8 T-cell Normal B-cell and NK cell Markedly decreased/ Absent isohemagglutinins (PHA) Decreased IgM Normal/ slightly low IgG Normal/ Elevated IgA, IgE Defective production of pneumococcal Ab Depressed lymphocyte response to mitogens
 Decreased IgM. Normal/ slightly low IgG. Normal/ Elevated IgA, IgE. Defective production of pneumococcal Ab. Depressed lymphocyte response to mitogens.")
73
Treatment 73 Allogeneic SCT is treatment of choice when matched donor available. If no matched donor is available the patient should be managed as follows: Aggressive treatment of infections Platelet transfusions for hemorrhagic episodes Steroid cream for eczema Splenectomy, reserved only for severe case with usual pre- and post-splenectomy precautions pertain Thrombopoietic agents are being explored.

74
Thank you for your attention
74

งานนำเสนอที่คล้ายกัน









>")









