ดาวน์โหลดงานนำเสนอ
1
Interesting case 17/05/07 Naree Panamonta, MD.

2
CC: ปวดศีรษะตามัว 2 เดือนก่อนมารพ.
ผู้ป่วยหญิงอายุ 20 ปี อาชีพนักศึกษาปวส. CC: ปวดศีรษะตามัว 2 เดือนก่อนมารพ. PI: 6 เดือนPTA ปวดศีรษะเป็นๆหายๆ กินยา paracetamol ทุเลาลง ไม่ได้ไปพบแพทย์ 2 เดือนPTA ปวดศีรษะตื้อๆที่ขมับสองข้าง มีคลื่นไส้ แต่ไม่อาเจียนเป็นเกือบตลอดเวลา เวลาปวดมาก pain score 10/10 ต้องกินยา paracetamol 2 tab/ครั้ง ประมาณ 3-4 tab/วัน อาการ progress มากขึ้นเรื่อยๆ ไม่มีผื่น ไม่มีผมร่วงหรือปวดข้อ ไม่ได้ไปพบแพทย์

3
1 เดือน PTA เริ่มมีตามัวสองข้าง เห็นจุดสีดำกลางตา คลื่นไส้มากขึ้น ไม่อาเจียน ไม่มีแขนขาอ่อนแรง
3 wk. PTA ตามัวมองเห็นไม่ชัดมากขึ้นทั้งสองข้าง ปวดศีรษะเท่าๆเดิม ไม่มีขี้ร้อน/ใจสั่น/มือสั่น ปัสสาวะออกเท่าเดิม มีนน.ลด 10 kg. ไปรพช.2 ครั้งบอกเป็น neuroretinitis both eyes refer มารพ.ศรีนครินทร์ ไม่ได้ check BP, VDRL-neg

4
5 day PTA มาตรวจที่ OPD eye ตรวจพบ
eye ground- Disc swelling, dot hemorrhage, cotton wool spot, flame shape hemorrhage, mild vvs. tortuosity both eyes, macula edema ไม่ได้วัด BP เจาะ lab ไว้แล้วนัด F/U 2 day PTA หอบเหนื่อยมากขึ้น หายใจไม่อิ่มนอนราบไม่สะดวก ปัสสาวะยังออกดี วันมารพ. มาตรวจ OPD eye ตามนัด วัดBPได้ 220/140 mmHg ส่งมา OPD 8

5
Physical exam GA- A young female, looked pale, fatigue, cachexia.
V/S- BP 214/150 mmHg, PR 124/min, RR 22 /min BP 4 extremities: / /143 255/ /141 HEENT- Marked pale, no jaundice, CLN-ve No engorged neck vein. Thyroid gland not enlarged.

6
Heart- Active precordium. LV heaving- positive. PMI at 6th ICS, 2 cm
Heart- Active precordium. LV heaving- positive. PMI at 6th ICS, 2 cm. lateral to MCL. Tachycardia, regular HR. No murmur. Lungs- Crepitation both basal lungs. Abdomen- Soft, liver and spleen not palpable. No renal bruit. Ext.- No edema. Equal pulses, no bounding pulse. No tremor, no moist skin.

7
Neuro- E4M6V5. Pupils 3 mm RTL, BE.
Eye ground- Blur disc with cotton wool spot with flame shape hemorrhage.Copper wire changes of vvs. CN intact all. Motor gr.V all. DTR 2+. BBK- plantar flexion both. Clonus- neg.

9
Problems Hypertensive emergency ( malignant HT)
with Target organ damaged - CNS: hypertensive retinopathy + encephalopathy - Acute pulmonary edema 2. Suspected secondary hypertension

10
CBC: Hb 11.3, Hct 33, WBC 11,800 ( N 68,L 19.1, Mo 10.1, Eo 1.4) Plt 136,000, MCV 82 UA: Sp , pH 7.0, Alb 4+, Glu –ve, RBC 5-10, WBC 10-20, Hyaline cast 10-20, Granular cast 10-20, Epi 1-2 BUN 14.8, Cr 1.8 Elyte: Na 137, K 3.3, HCO3 25.6, Cl 106 Ca 8.6, PO4 4.1, Mg 2.2 LFT- Chol 201, Alb 3.7, Glob 3.6, TB 1.9, DB 0.2, ALT 16, AST 40, ALP 74

11
Chest X-ray: LV hypertrophy, cephalization of pulmonary vein, Kerley’s B line. EKG- Sinus tachycardia, LVH by voltage, No LV strain pattern Film KUB- Not seen stone Urine Elyte- Na 10, K 41.1, Cl 22 Urine 24 hr- Cr 0.6, Prot 2,409 mg/vol, Vol= 760 ml. GFR= 23

12
Serum osmole 287, Urine osm. 573 TTKG = 6.2 ANA – negative Anti- HIV: Non reactive TFT- FT ( pg/ml) FT ( ng/dL) TSH ( mIU/ml)
 TSH 5.21 ( mIU/ml)")
13
Ultrasound KUB Increase parenchymal echogenicity with loss of corticomedullary differentiation. Kidney size: Rt.9.15 cm., Lt cm. Cortical thickness: Rt cm., Lt cm. No hydronephrosis.

14
Problem lists Hypertensive emergency ( malignant HT)
with Target organ damaged - CNS: hypertensive retinopathy - Acute pulmonary edema - R/O Hypertensive nephropathy 2. Secondary hypertension 3. Hypokalemic metabolic alkalosis

15
Differential Dx of 2ry HT cause
1. Renal parenchymatous disease - Chronic glomerulonephritis : Chronic- Hx of prolong symptoms, eye ground changes : Impaired renal function, nephritic ranged proteinuria, active urinary sediments 2. Hyperaldosteronism : Hypokalemia, metabolic alkalosis

16
Differential Dx of 2ry HT cause
3. Renovascular hypertension 4. Pheochromocytoma 5. Other endocrine HT: hyperthyroidism (TFT- WNL)
")
17
Management (this case)
Diltiazem IV drip NTG IV drip Add oral hypertensive medications: - Nifecard retard, Prazocin, Hydralazine, Methyldopa, Metoprolol Collect urine VMA 24 hr. Kidney biopsy CT adrenal gland

18
Kidney biopsy patho (H&E stain):
Arteriolar medial thickening. Increased mesangial matrix. Tubulointerstitial change. Imp: Malignant hypertensive nephrosclerosis

19
Urine 24 hr. VMA 27/04/ ug/mg Cr ( ) 28/04/ ug/mg Cr 29/04/ ug/mg Cr CT adrenal gland - Non enhancing posterior Lt. pararenal mass contains fat density. - Normal both adrenal glands. - Small liver nodule at segment 7 about 1 cm. in diameter. Imp: Lt. posterior pararenal mass contains fat density DDx retroperitoneal mass.

20
Malignant Hypertension due to Secondary HT

21
Effects of HT (TOD) 1. Heart - Concentric LV hypertrophy
- Myocardial ischemia/ infarction - Congestive heart failure 2. Neurologic - Retinal and CNS dysfunction - Dizziness, light-headedness, vertigo, tinnitus, syncope - Cerebral infarction/ hemorrhage - Hypertensive encephalopathy: severe HT, impaired consciousness, increased ICP, retinopathy with papilledema, seizure

22
Effects of HT (TOD) 3. Kidney
- Atherosclerosis of afferent and efferent arteriole, glomerular capillary tufts - Decrease GFR, tubular dysfunction - Glomerular disease as a cause: proteinuria, microscopic hematuria

23
Hypertensive emergency
Diastolic BP > 120 mmHg Severe acute target organ damage - Hypertensive encephalopathy: severe headache, vomiting, visual disturbances, transient paralysis, convulsion, stupor, coma - Cardiac decompensation - Rapidly declining renal function

24
Hypertensive emergency
Vascular lesion - Fibrinoid necrosis of walls of small arteries arterioles - Cerebral arteries dilate excessive cerebral blood flow Microangiopathic hemolytic anemia ( 2ry to deteriorate renal function)
")
25
Hypertensive emergency: Management
Rapid acting IV antihypertensive agent - Labetalol, Fenoldopam, Nitroprusside, Nimodipine - Decrease DBP 10-15% in < 1 hr.( not to level < 95 mmHg) IV nitrate + furosemide in acute pulmonary edema Correction underlying disease
 IV nitrate + furosemide in acute pulmonary edema. Correction underlying disease.")
26
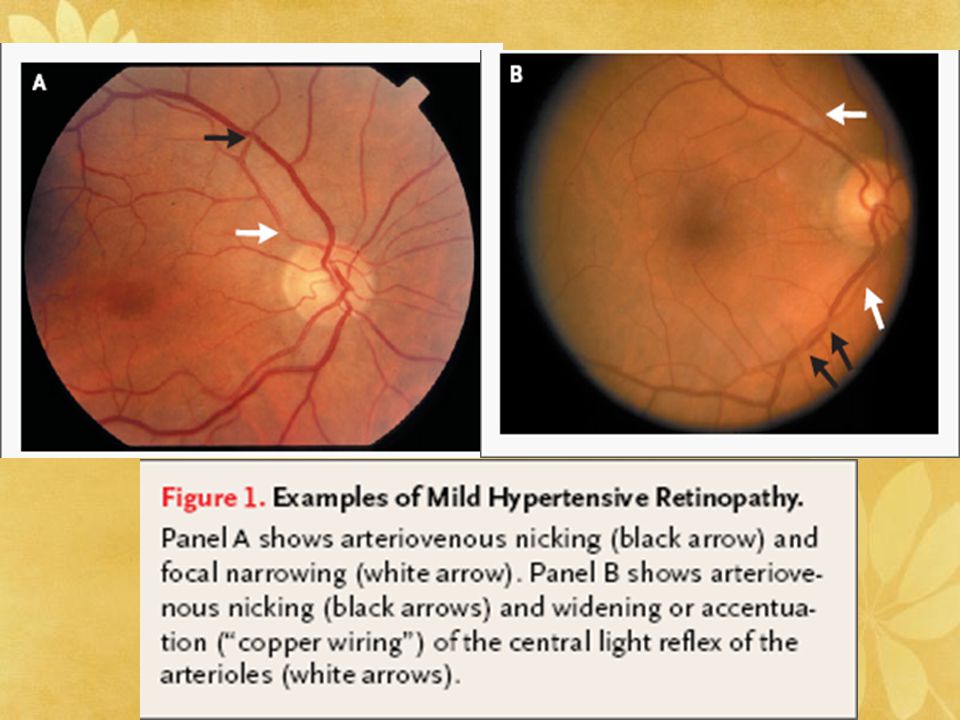
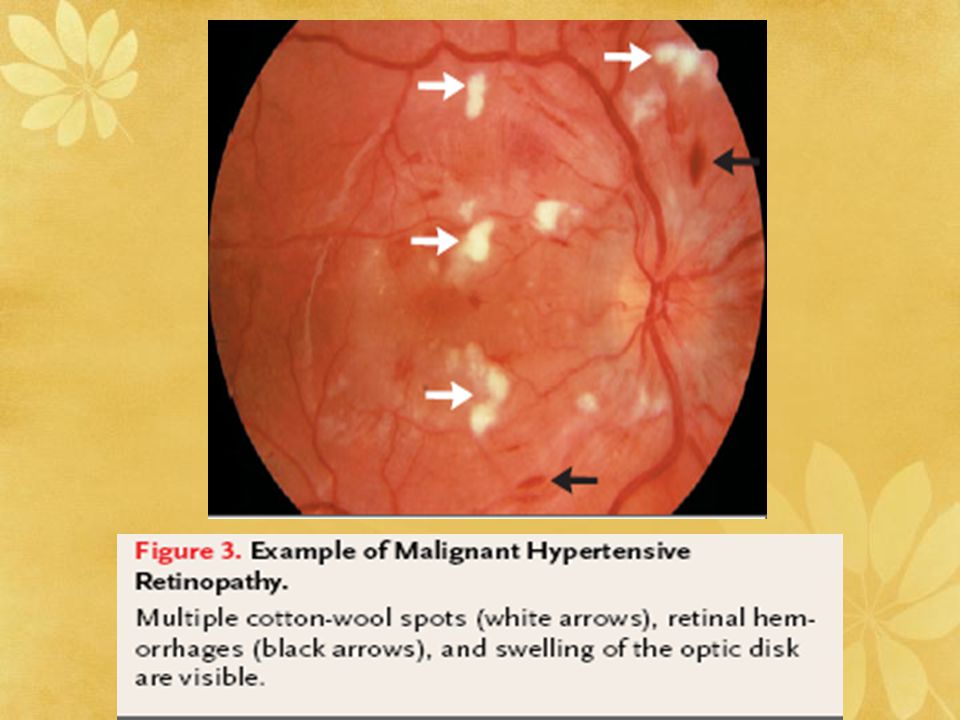
Hypertensive Retinopathy
In 1939, Keith et. al. ----predictive of death in HT patients Classification system: Keith-Wagener-Barker classification – categorized into 4 groups of increasing severity Signs of hypertensive retinopathy regress with control of BP

31
Hypertensive nephrosclerosis
Present with HT& its complications (eg, heart failure, stroke), and/or symptoms of uremia. Features suggesting HN : - Black race - Hypertensive retinal changes - Left ventricular hypertrophy - Long-standing (usually >10 y) or very severe hypertension - Proteinuria less than 0.5 g/d - Hypertension diagnosed prior to onset of proteinuria - Hypertension preceding renal dysfunction - No evidence of another renal disease - Biopsy findings compatible with the diagnosis
, and/or symptoms of uremia. Features suggesting HN : - Black race. - Hypertensive retinal changes. - Left ventricular hypertrophy. - Long-standing (usually >10 y) or very severe hypertension. - Proteinuria less than 0.5 g/d. - Hypertension diagnosed prior to onset of proteinuria. - Hypertension preceding renal dysfunction. - No evidence of another renal disease. - Biopsy findings compatible with the diagnosis.")
32
Hypertensive nephrosclerosis
- 30% present with declined GFR at presentation - Some patients with biopsy-proven HN have 24-hour urinary protein increase to the nephrotic range when secondary changes of FSGS present

33
Glomeruli obsolescence, interstitial fibrosis, arterial intimal fibroplasia, arteriolar hyalinization in arterioles Glomerular hyalinosis and the development of secondary tubular atrophy and interstitial fibrosis Wrinkling of the glomerular tuft and thickening of the Bowman capsule

34
Hypertensive nephrosclerosis
Antihypertensive therapy and ACE inhibitor - Nephrosclerosis is part of generalized vascular disease - Patients with cardiovascular disease and impaired renal function benefit more than those with normal kidney function - BP control magnify long-term cardiovascular risk

35
Essential vs. Secondary HT

36
2ry HT is suspicion 1. Age <35 or > 55
2. Therapeutic failure with initial drug program(3-drug rx.) 3. BP >180/110 mmHg 4. Sudden↑ BP in well-controlled HTN
 3. BP >180/110 mmHg. 4. Sudden↑ BP in well-controlled HTN.")
37
2ry HT is suspicion 5. Signs & symptoms of specific disease
- HA/palpitation/pallor/sweats - Renal bruits - SBP in legs < 20 mm SBP in arms - Cushing's physical stigmata 6. Abnormal lab - K+ <3.5 - Elevated creatinine - Elevated calcium - Abnormal UA

38
Causes of 2ry HT Renal HT Renal parenchymal Renovascular Endocrine HT
1ry aldosteronism renin producing tumor Cushing’s syndrome Pheochromocytoma Hyperthyroidism Hypercalcemia Acromegaly

39
Causes of 2ry HT Vascular cause - Coarctation of aorta
Obstructive sleep apnea Medications: OCPs, Cocaine, EtOH

40
Renal Parenchymal Disease
Single largest cause of secondary hypertension Most are irreversible. Acute renal failure - Acute glomerulonephritis (especially post-infectious, crescentic, or focal segmental changes) - Vasculitis (esp. SLE, scleroderma, or polyarteritis - Acute obstruction
 - Vasculitis (esp. SLE, scleroderma, or polyarteritis. - Acute obstruction.")
41
Renal Parenchymal Disease
Chronic renal failure: nephron loss>80% - Vasculitis - Glomerular disease (especially diabetic nephropathy and crescentic or focal segmental glomerulitis) - Polycystic renal disease
 - Polycystic renal disease.")
42
Chronic glomerulonephritis
1. Rapidly progressive glomerulonephritis (RPGN) or crescentic glomerulonephritis - 90% progress to ESRD within weeks or months. 2. Focal segmental glomerulosclerosis (FSGS) - 80% progress to ESRD in 10 years - Collapsing variant : Malignant FSGS, have more rapid progression : Idiopathic or related to HIV infection. 3. Membranous nephropathy % progress to chronic renal failure (CRF) and ESRD in 10 years.
 or crescentic glomerulonephritis. - 90% progress to ESRD within weeks or months. 2. Focal segmental glomerulosclerosis (FSGS) - 80% progress to ESRD in 10 years. - Collapsing variant. : Malignant FSGS, have more rapid progression. : Idiopathic or related to HIV infection. 3. Membranous nephropathy % progress to chronic renal failure (CRF) and ESRD in 10 years.")
43
Chronic glomerulonephritis
4. Membranoproliferative glomerulonephritis (MPGN) - 40% progress to CRF and ESRD in 10 years. 5. IgA nephropathy - 10% progress to CRF and ESRD in 10 years. 6. Poststreptococcal glomerulonephritis - 1-2% progress to CRF and ESRD. - Older children or adults with crescentic glomerulonephritis are at greatest risk
 - 40% progress to CRF and ESRD in 10 years. 5. IgA nephropathy. - 10% progress to CRF and ESRD in 10 years. 6. Poststreptococcal glomerulonephritis % progress to CRF and ESRD. - Older children or adults with crescentic glomerulonephritis are at greatest risk.")
44
Chronic glomerulonephritis
Hemodialysis + antihypertensive may increase survival in malignant hypertension associated with severely damaged renal function Difficult to distinguish - HT is a consequence of nephritis or consequence of renal failure

45
Renovascular HT Fibromuscular dysplasia of renal arteries - About 25% of all renovascular HT - Young females Atherosclerotic disease - Nearly 70% of the total - Generally arise bilaterally Arteriography- gold standard : Critical stenoses of ≥80%

46
Renovascular HT ACE-inhibitor produces a fall GFR on the affected side. Positive scan correlates with successful angioplasty or surgical intervention in ≥ 90% (less definitive in the presence of renal dysfunction)
")
47
Hyperaldosteronism Primary hyperaldosteronism
- Adenoma, carcinoma, or bilateral hyperplasia - Enzymatic deficiencies (11-OH-hydroxylase deficiency, 17-OH-hydroxylase deficiency, and 11-OH-dehydrogenase deficiency syndromes) - Chronic licorice ingestion Non-specific weakness, fatigue, polyuria, or cramps (reflecting hypokalemia)
 - Chronic licorice ingestion. Non-specific weakness, fatigue, polyuria, or cramps (reflecting hypokalemia)")
48
Hyperaldosteronism Best screening test : 24-hour urinary collection for aldosterone Simpler screening test : Plasma aldosterone to plasma renin activity (PRA) ratio PA/PRA ratio >30 and a PA >20 ng/ml (withdrawn from antihypertensive medications for ≥two weeks)
 ratio. PA/PRA ratio >30 and a PA >20 ng/ml. (withdrawn from antihypertensive medications for ≥two weeks)")
49
Pheochromocytoma Nearly 80% of the tumors limited to adrenal glands
- Usually unilaterally - Bilateral or multiple in neurofibromatosis, Von Hippel-Lindau disease, or MEN type 2a or 2b 10-20% intra-abdominal sites, <5% from intrathoracic sites

50
Pheochromocytoma Classic triad : episodic headache, palpitations with or without tachycardia, and inappropriate perspiration Definitive diagnosis and full localization requires both : Biochemical tests for catecholamines : Scanning potential sites by CT or MRI

51
Medications - Vasoconstrictors : phenylephrine, pseudoephedrine, phenylpropanolamine, β-agonist bronchodilators, ephedrine, cocaine, stimulant abuse, anti-adrenergic agent withdrawal, and MAOI cotreatment with tyramine-containing foods Volume expanders (glucocorticoids, estrogens at high doses, NSAIDS Poorly specified mechanisms such as cyclosporine, tacrolimus, or erythropoietin Miscellaneous other agents like psychotropic drugs that interfere with sympatholytic antihypertensive agents

52
Thank you for your attention



















 98.08% 100.02% จังหวัด.>")




