ดาวน์โหลดงานนำเสนอ
1
SNHL in children and Hearing Screening
Dr. Greetha Moungthong , Dept. Otolaryngology PMK Hospital

2
การสูญเสียการได้ยินแบบประสาทหูเสื่อมในเด็ก (Sensorineural Hearing Loss in children)
วัตถุประสงค์ 1. รู้รายละเอียดของการสูญเสียการได้ยินแบบประสาทหูเสื่อมในเด็ก รู้แนวทางในการตรวจการวินิจฉัยเด็กที่มีปัญหาสูญเสียการได้ยิน 3. รู้แนวทางในการรักษาเด็กที่มีปัญหาสูญเสียการได้ยิน 4. สามารถให้คำแนะนำแก่บิดามารดาได้

3
การสูญเสียการได้ยินจะมีผลกระทบต่อ
การพูด (speech & language development) การพัฒนาการภาษา ( language development) การเรียนรู้ของเด็ก (Psychosocial & cognitive development) การพัฒนาด้านสังคม ( Social development ) Poor quality of life
 การพัฒนาการภาษา ( language development) การเรียนรู้ของเด็ก (Psychosocial & cognitive development) การพัฒนาด้านสังคม ( Social development ) Poor quality of life.")
4
คนปกติจะสามารถได้ยินความดัง 20 – 25 dB ความถี่ระหว่าง 20 – 20,000 Hz
การสูญเสียการได้ยินแบบ Conductive Hearing Loss การสูญเสียการได้ยินแบบ Sensorineural Hearing Loss 1 : 1000 in infant 2 : 1000 by age 19 years

5
Cochlea Cross-Section & Organ of Corti

6
No Hair Cells!

7
CLASSIFICATION OF SNHL
Congenital : Genetic :-syndromic :-non- syndromic : Acquired (Prenata/ Perinatal) Delayed : Acquired (Postnatal)
 Delayed. : Acquired (Postnatal)")
8
Etiology of SNHL Genetic factor 36 %
Viral (prenatal / perinatal ) % Meningitis % Perilymphatic fistula(PLF) % Labyrinthine abnormalities % Metabolic / neoplatic % Unknown %
 31 % Meningitis 6 % Perilymphatic fistula(PLF) % Labyrinthine abnormalities 15 % Metabolic / neoplatic 1 % Unknown 31 %")
9
Congenital SNHL in Childhood
Present at birth Could be caused by Hereditary , infection, intrauterine insult, teratogenic factors If bilateral, should be detected early Neonatal screening is important

10
Hereditary SNHL in Childhood (30 -50 %)
1/3 of genetic are syndromic > 1000 syndromes 2/3 of genetic are nonsyndromic 80 % Recessive 18 % Dominant 2 % X-Linked

11
SNHL syndromic 1/3 of all hereditary
Characteristic physical and other findings comprise the phenotype Common : Treacher-Collins, Waardenberg, Pendred, Usher Other : Goldenhar-hemifacial microsomy

12
WAARDENBURG SYN SNHL with pigmentary abn. Autosomal dominant >90 %

13
Branchio-oto-renal (Melnick-Fraser syn)
Branchial arch defects ( ear pits, cervical fistula Renal abnl. Lacrimal duct abnl.

14
USHER SYNDROME SNHL & retinitis pigmentosa 4 % of congenital deafness
Visual is progressive :age 10 ; Night blindness 92 % Retinal changes may be diagnosed in infancy ½ of the deaf–blind population

15
PENDRED SYNDROME Autosomal recessive Goiter & Hearing loss
2 % of severe to profound deafness

16
Jervell & Lange-Nielsen syn
Autosomal recessive, Severe congenital SNHL, Syncopal episodes EKG : prolong QT interval , Large T waves

17
ALPORT’S SYNDROME Autosomal dominant, recessive , X-Linked
1 % of childhood deafness , 50% progressive high frequency SNHL ,develops in first & second decade of life, progressive Renal dysfunction Dx: Proteinuria, hematuria, cellular casts with progress Hearing loss

18
Congenital Non-syndromic SNHL
Inner ear anomallies Michel’s Mondini’s Scheibe’s Alexander’s Degree of inner ear dysplasia/aplasia

19
ACQUIRED SNHL (Prenatal/Perinatal)
Infection Ototoxic substances Prematurity Kernicterus Birth trauma

20
INFECTIOUS (Prenatal/Perinatal)
Toxoplasmosis Rubella Cytomegalovirus Herpes Syphilis TORCHES

21
Meningitis and Labyrinthitis
S. pneumoniae SNHL occurs more frequently in patient with S. pneumoniae Incidence of meningitis 20 HIB decreasing due to vaccine

22
Prematurity 20 fold increase in SNHL 5% of NIUC graduates have SNHL

23
Risk factors associated with prematurity
Anoxia Low birth weight Acidosis Hyperbilirubinemia Ototoxic medications Meningitis Prolonged mechanical ventilation

24
EVALUATION & ASSESSMENT OF SNHL IN CHILDHOOD

25
Protocol for high risk infant
Evaluation by : Otolaryngologist Audiologist Speech therapist Genetics Family counseling

26
การวินิจฉัย (Evaluation)
1. ประวัติการพัฒนาการ (Developmental History) 2. ประวัติครอบครัว (Family History) 3. ประวัติการตั้งครรภ์ (Prenatal History) พบว่าการติดเชื้อในครรภ์มารดากลุ่ม “TORCHES” (Toxoplasmosis, Syphilis, Rubella, Cytomegalovirus, และ Herpes) มีผลต่อการเกิด Congenital SNHL 4. Perinatal History
 2. ประวัติครอบครัว (Family History) 3. ประวัติการตั้งครรภ์ (Prenatal History) พบว่าการติดเชื้อในครรภ์มารดากลุ่ม TORCHES (Toxoplasmosis, Syphilis, Rubella, Cytomegalovirus, และ Herpes) มีผลต่อการเกิด Congenital SNHL. 4. Perinatal History.")
27
Physical examination Cleft lip/palate White forelock
Heterochromic irises Vitiligo Dystopia canthorum Branchial arch/cleft anomalies(esp. bilateral) Hemifacial microsomia/micrognathia Abnormal pinna Goiter
 Hemifacial microsomia/micrognathia. Abnormal pinna. Goiter.")
28
Childhood SHNL : Evaluation
BUN/Cr ; U/A Metabolic : TFT ; FBS Autoimmune : Cogan’s, Ds Serology for Syp. Immunologic Tests for viral infection EKG Ophthalmological Consultation CT Temporal bone : inner ear malfunction

29
Hearing Assessment subjective method Tympanogram
OAE (Otoacoustic Emission) ABR (Auditory Brainstem Respond) Objective method BOA (Behavioral Observation Audiometry) VRA ( Visual Reinforcement) ( 6 ms - 2 yr.) Play Audiometry ( yr.)
 ABR (Auditory Brainstem Respond) Objective method. BOA (Behavioral Observation Audiometry) VRA ( Visual Reinforcement) ( 6 ms - 2 yr.) Play Audiometry ( yr.)")
30
Tympanogram Audiogram

31
resonance OAEs

32
TEOAE IN NORMAL HEARING

33
Hearing screening in infant
Incidence of Bilateral SNHL 50 dB in school age = per 1000 Bilateral SNHL 75 dB in school age = per 1000 1/174 children in NICU vs 1/1278 in Non NICU National Institute of Health of USA Recommend Universal Hearing screen ( All infant in NICU & All infant within 3 ms of age ) Thailand : recommend esp. in high risk infant
 Thailand : recommend esp. in high risk infant.")
34
High risk infant FH of Hereditary SNHL Intrauterine infection (TORSCH)
Craniofacial anomalies Birth weight < 1500 gm Hyperbilirubinemia Ototoxic medication Bacterial Menigitis Severe asphyxia Mechanical ventilation

35
Hearing Assessment Play Audiometry PASS OAE Normal Hearing
Rehabilitation ABR FAIL Abnormal

36
หลักการรักษาการสูญเสียการได้ยินในเด็ก
วินิจฉัยการสูญเสียการได้ยิน โดยเร็วที่สุดตั้งแต่ในวัยเด็ก รักษาโรคตามสาเหตุที่ตรวจพบ เพื่อยุติการสูญเสียการได้ยินเพิ่มขึ้น ฟื้นฟูสมรรถภาพการได้ยิน

37
Hearing Rehabilitation
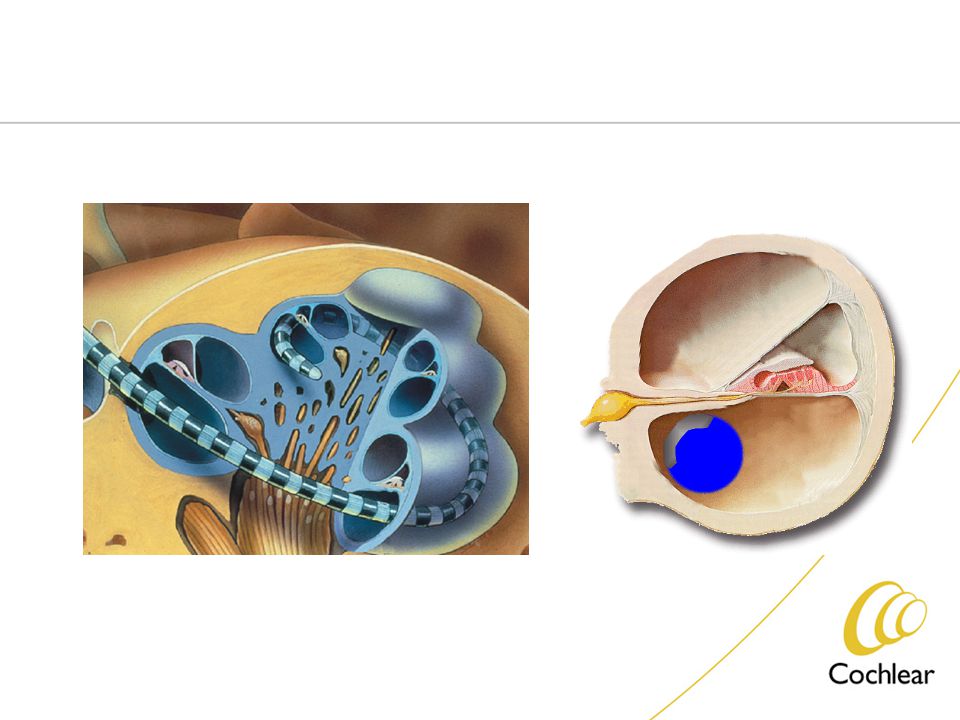
Hearing Aid Cochlear Implantation (การฝังประสาทหูเทียม ) Sigh and language learning
 Sigh and language learning.")
38
เครื่องช่วยฟัง (Hearing Aid)
ปัญหาของการสูญเสียการได้ยินทั้งสองหู ระดับสูญเสียการได้ยินมาก (Moderate to Severe SNHL) โดยจะทำหน้าที่ขยายเสียงที่เด็กจะรับในช่วงความถี่ที่เหมาะสม (ความถี่ช่วงภาษาพูด) ตัดความถี่ของเสียงที่รบกวนออกไป (ความถี่สูงๆ)
 โดยจะทำหน้าที่ขยายเสียงที่เด็กจะรับในช่วงความถี่ที่เหมาะสม (ความถี่ช่วงภาษาพูด) ตัดความถี่ของเสียงที่รบกวนออกไป (ความถี่สูงๆ)")
39
Cochlear Implantation Criteria
Profound SNHL Both Ear Age > 2 year No benefit from Hearing Aids following 6 month trial Earlier implantation in cases of meningitis Action : directly stimulate auditory Nerve fiber within cochlea

41
Complications of Cochlear Implant
1. Facial nerve injury 2. Meningitis 3. Failure implantation 4. Extrusion of implant

42
Hearing outcomes in young children UK pediatrics progress report 1990, N = 182
Understand conversation without lip reading Nottingham CI Program Identify environmental sounds Not aware of sounds

43
Factors influence to post operative results
Number of inserted electrodes Duration of deafness Intelligence Inherent linguistic ability Hearing impairment since childhood

44
Thank you for attention
and Any question



 JAMA. 2009;301(15):1547-1555.>")

















