ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

2
The Detection of Ischemia in Asymptomatic Diabetics (DIAD study) JAMA. 2009;301(15):1547-1555
 JAMA. 2009;301(15):")
3
Coronary artery disease (CAD) Coronary artery disease (CAD) : major cause of mortality and morbidity in patients with type 2 DM Often asymptomatic until MI or sudden cardiac death Type 2 DM = CAD risk equivalent Current standard of care emphasizes the reduction of cardiovascular risk factors But But the utility of screening patients with type 2 DM for asymptomatic CAD is controversial.
 Coronary artery disease (CAD) : major cause of mortality and morbidity in patients with type 2 DM Often asymptomatic until MI or sudden cardiac death Type 2 DM = CAD risk equivalent Current standard of care emphasizes the reduction of cardiovascular risk factors But But the utility of screening patients with type 2 DM for asymptomatic CAD is controversial.")
5
To assess whether routine screening for CAD identifies patients with type 2 DM as being at high cardiac risk and whether it affects their cardiac outcomes.

6
Method Age 50-75 years Onset of type 2 DM occurred at age 30 years No history of ketoacidosis Angina pectoris or chest discomfort Stress test or CAG within the prior 3 years History of MI, heart failure, or coronary revascularization Abnormal rest EKG results Pathological Q waves Ischemic (1 mm depression) ST segments Deep negative T waves, or Complete LBBB Inclusion criteria (3) Exclusion criteria (7)
 ST segments Deep negative T waves, or Complete LBBB Inclusion criteria (3) Exclusion criteria (7)")
7
Method Any clinical indication for stress testing Active bronchospasm precluding the use of adenosine Limited life expectancy due to cancer or end-stage renal or liver disease

9
Method Between July 2000 and August 2002. (25 month) DIAD protocol The study design and procedures were explained by a member of the local research team All participants History : health status, medications, intervening cardiac events, additional stress testing, CAG, and revascularizationat 6- month intervals Physical examination : diabetic neuropathy, cardiac autonomic dysfunction Lab : Blood and urine laboratory testing
 DIAD protocol The study design and procedures were explained by a member of the local research team All participants History : health status, medications, intervening cardiac events, additional stress testing, CAG, and revascularizationat 6- month intervals Physical examination : diabetic neuropathy, cardiac autonomic dysfunction Lab : Blood and urine laboratory testing.")
10
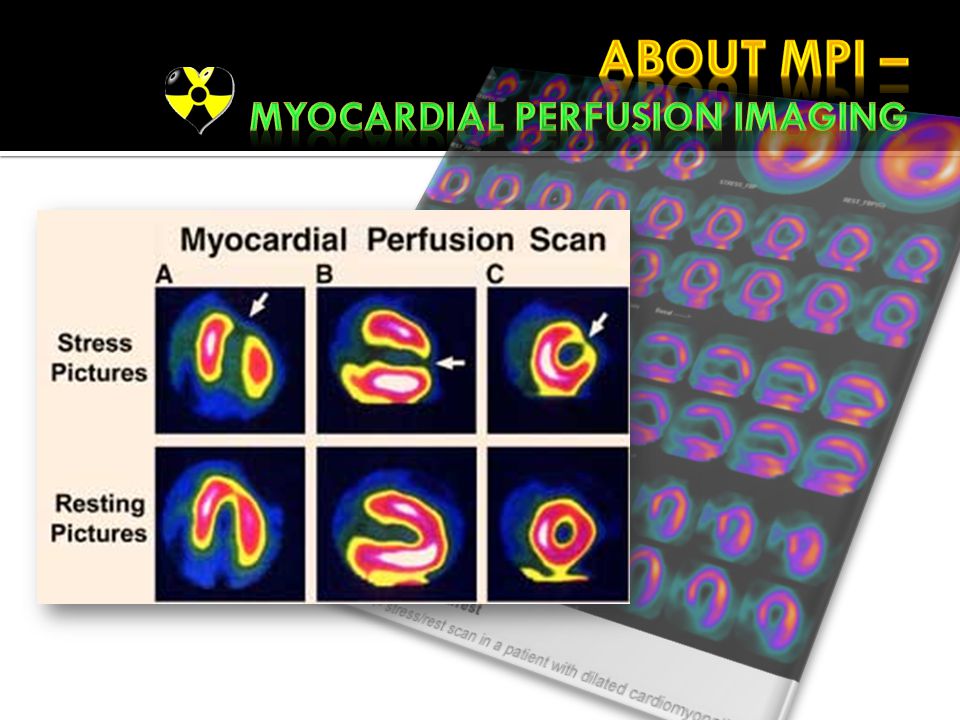
Method Randomization Sequential identification number at each site A corresponding sealed envelope was opened Random permuted blocks (block size 6) sequence 1:1 561 participants was screening with adenosine Tc- 99m sestamibi MPI, interpreted by nuclear cardiologists
 sequence 1:1 561 participants was screening with adenosine Tc- 99m sestamibi MPI, interpreted by nuclear cardiologists")
12
Nonfatal MI Cardiac death-included fatal MI (within 30 days) Death due to heart failure or arrhythmia Sudden cardiac death Unstable angina Heart failure Stroke Coronary revascularization Primary end point Secondary end points
 Death due to heart failure or arrhythmia Sudden cardiac death Unstable angina Heart failure Stroke Coronary revascularization Primary end point Secondary end points")
13
DataStatistic analysis SAS statistical software version 9.1 Bivariate associations, according to loss F/U, randomization status, and factors associated with cardiac events t tests Wilcoxon Rank sum, 2, and Fisher Changes in medicationsMcNemar test and logistic regression. Hazard ratios (HRs) comparing (1)Events in screened vs nonscreened (2)Events in participants with normal MPI vs nonperfusion, small or moderate or large perfusion defects Cox proportional hazards regression
 comparing (1)Events in screened vs nonscreened (2)Events in participants with normal MPI vs nonperfusion, small or moderate or large perfusion defects Cox proportional hazards regression.")
14
Was the assignment of patients to screening randomised ?

15
Were measures objective or were the patients and clinicians kept “blind” to which treatment was being received?

16
Mean (SD) 4.8 (0.9) years Median 5 years F/U was complete 97% at 3.5 years Last data collected in Sep 2007 Mean (SD) 4.8 (0.9) years Median 5 years F/U was complete 97% at 3.5 years Last data collected in Sep 2007
 4.8 (0.9) years Median 5 years F/U was complete 97% at 3.5 years Last data collected in Sep 2007 Mean (SD) 4.8 (0.9) years Median 5 years F/U was complete 97% at 3.5 years Last data collected in Sep 2007")
20
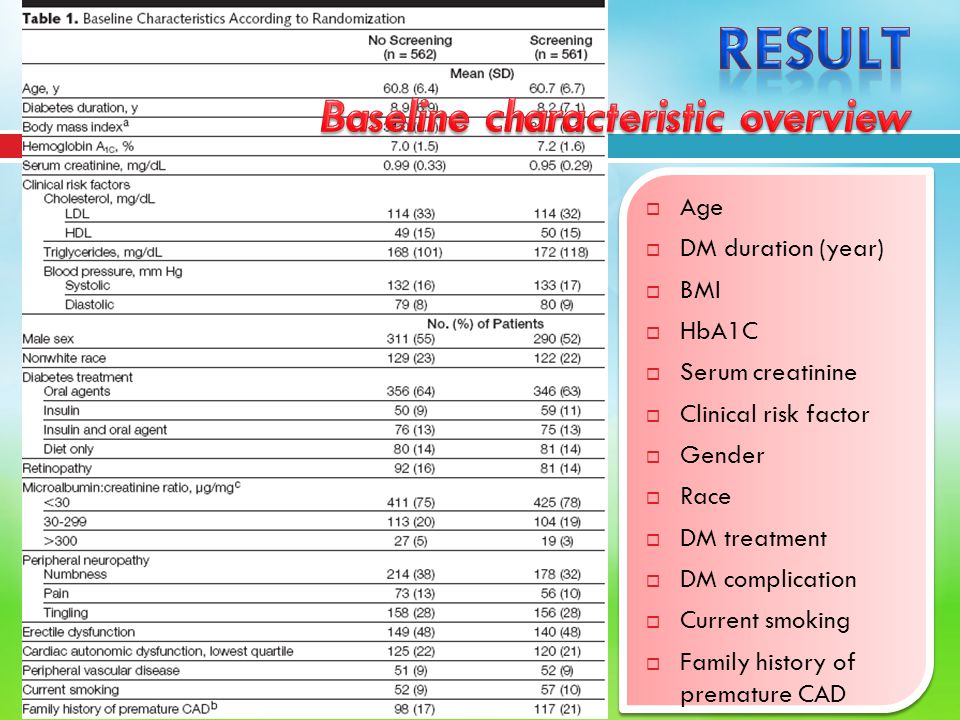
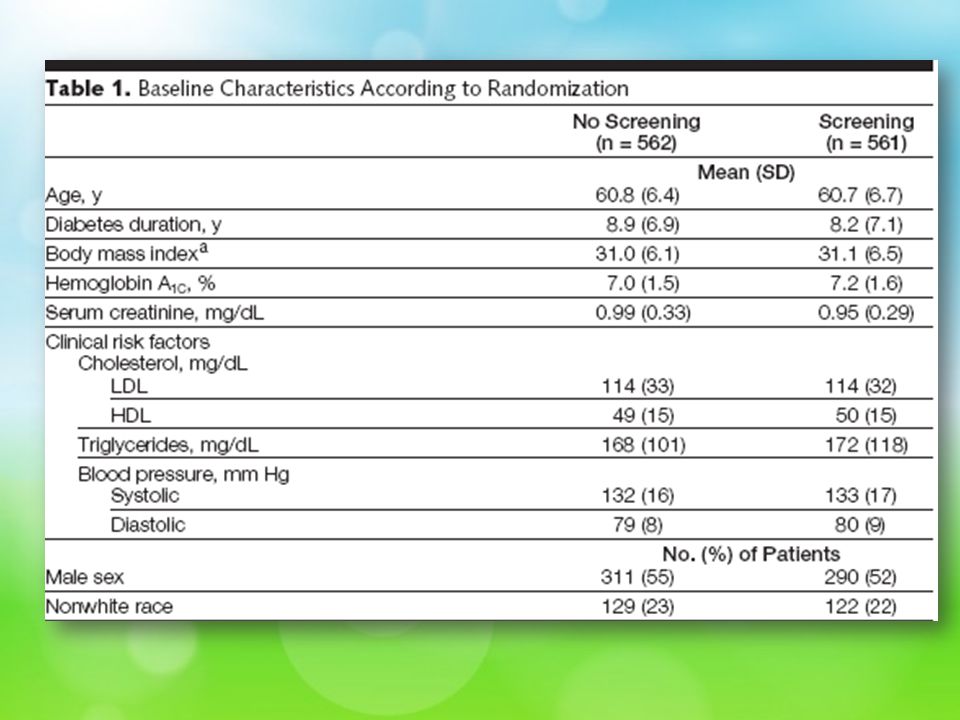
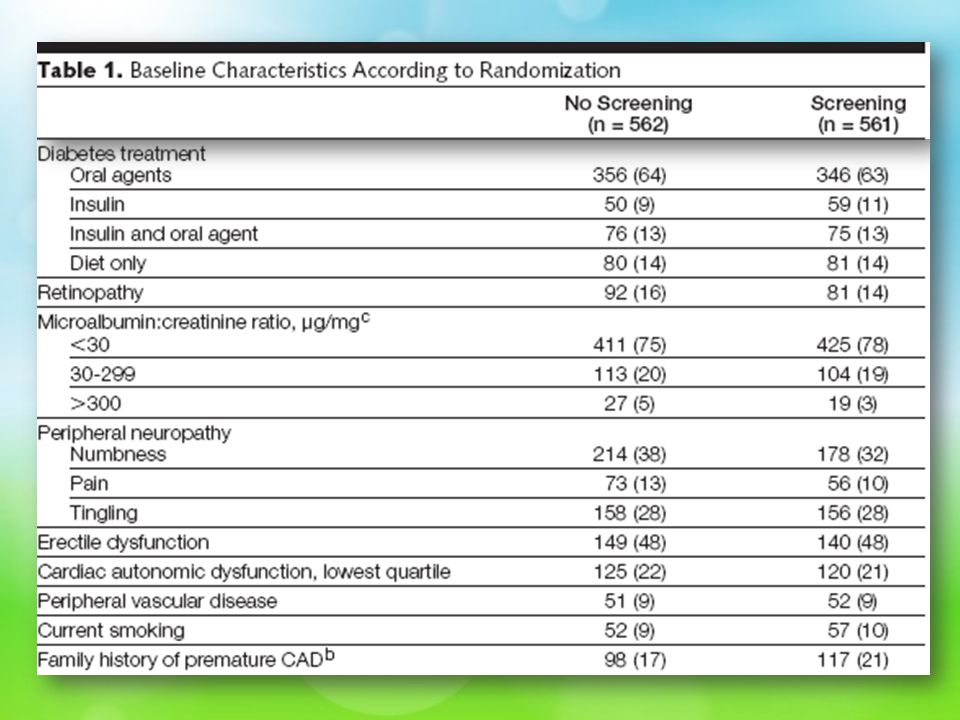
Were the groups similar at the start of the trial?

21
Aside from the allocated screened, were groups screened equally?

22
Were all patients who entered the trial accounted for? – and were they analysed in the groups to which they were randomised?

25
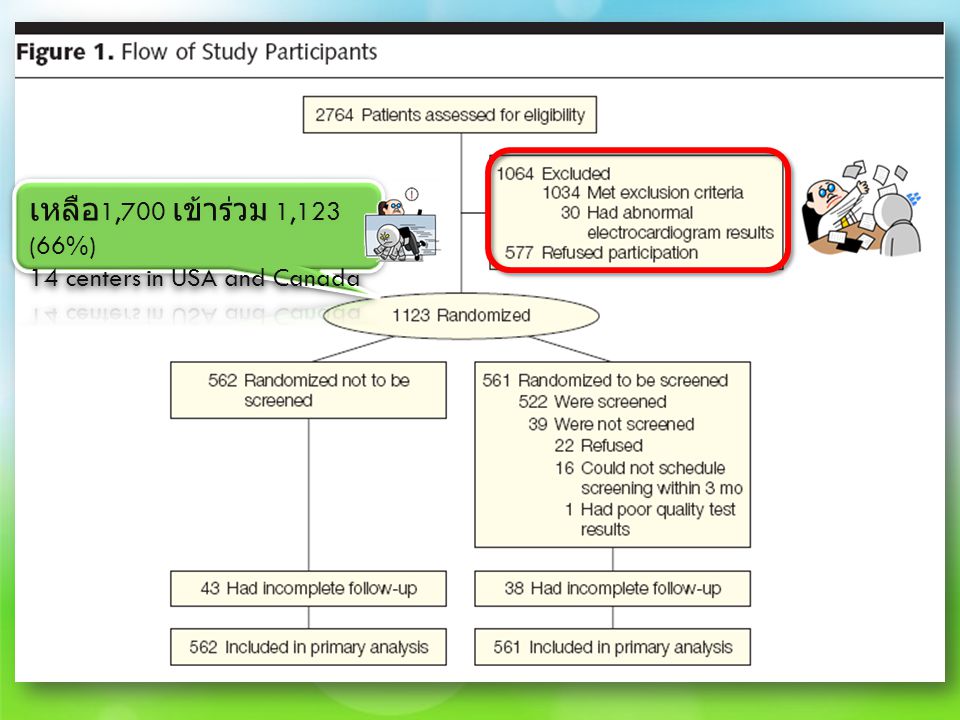
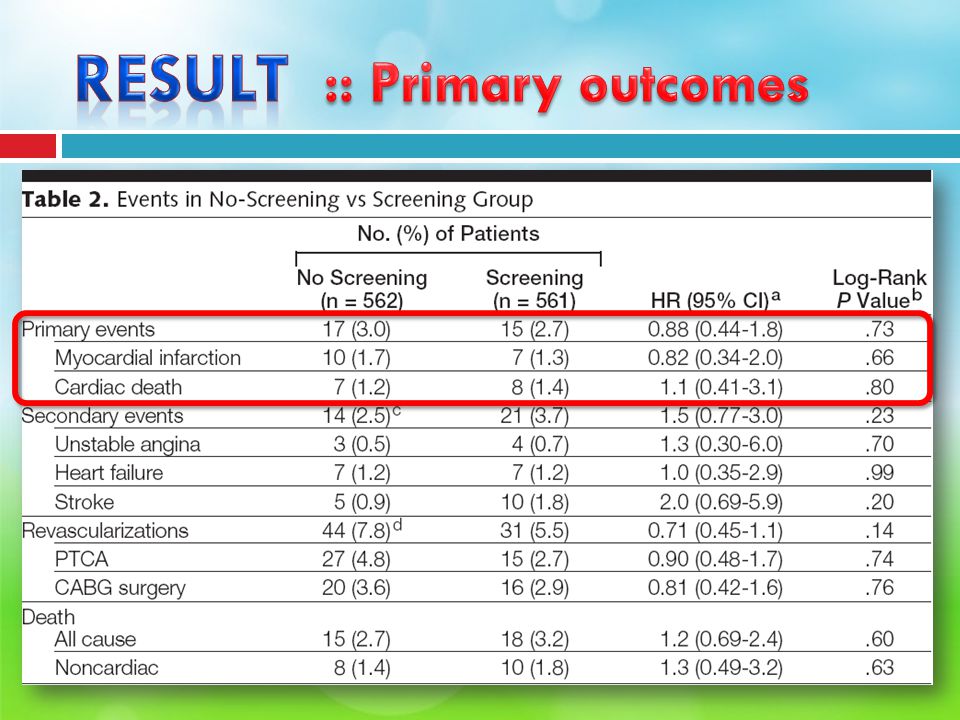
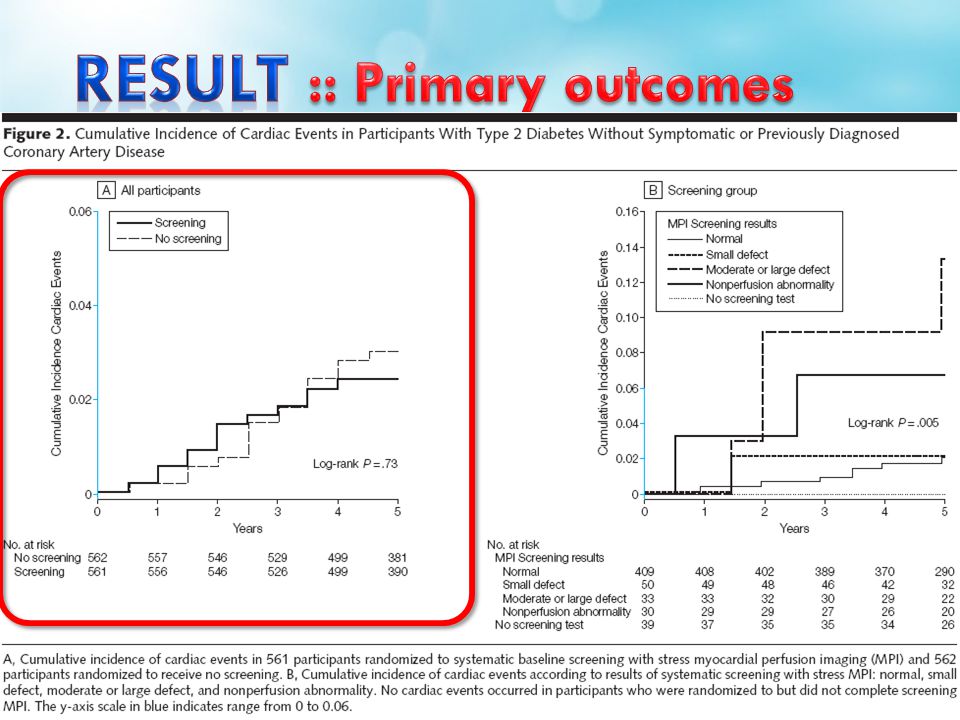
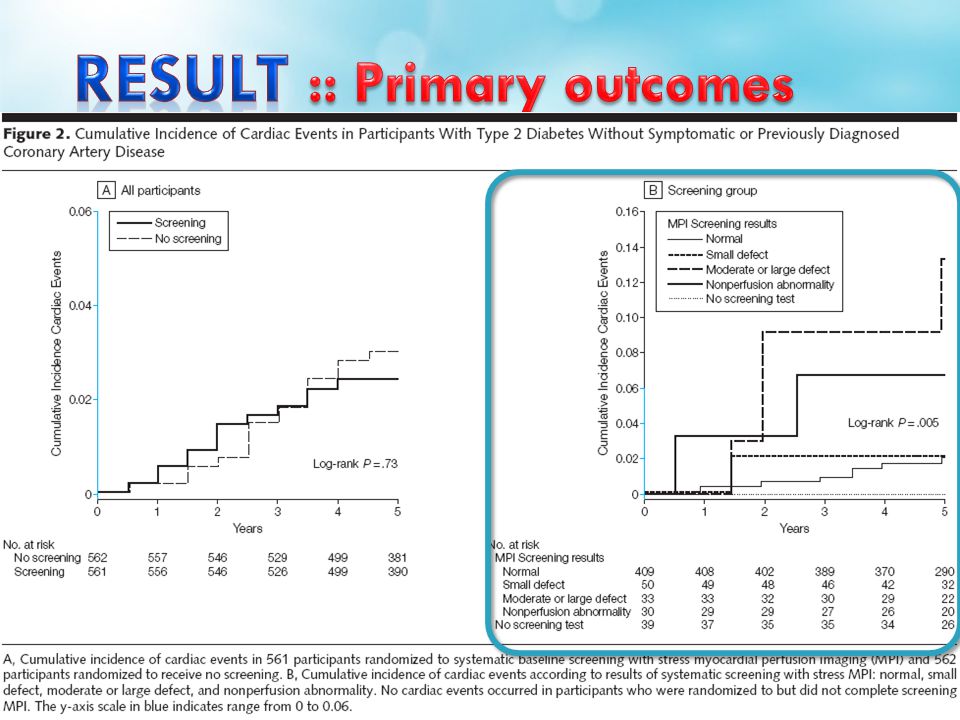
32 cardiac event (17 MI + 15 cardiac death) Overall cumulative 5-year cardiac event rate = 2.9 % (average 0.6% per year)
 Overall cumulative 5-year cardiac event rate = 2.9 % (average 0.6% per year)")
28
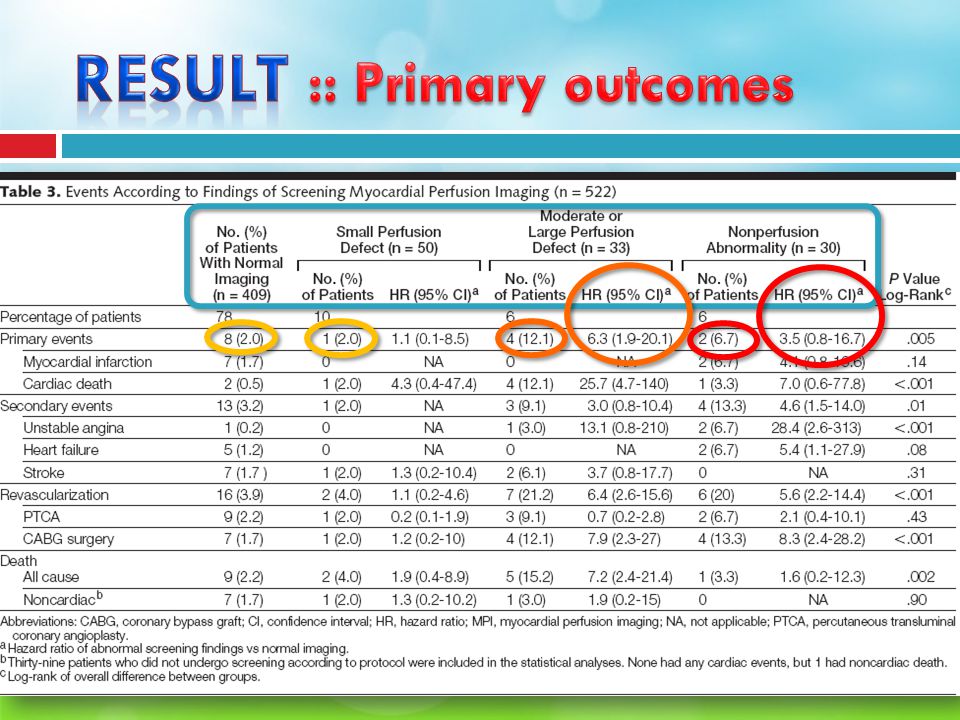
Mean (SD) Mean (SD) MPI defect size [P = 0.12] Cardiac event4.1% (6.6%) No cardiac event 1.4% (2.2%) Negative predictive value Negative predictive value of having a normal MPI = 98% (401of 409). Positive predictive value 6% (7 of 113) of patients for any MPI abnormality 12% (4 of 33) of patients for moderate or large MPI defects.
![ Mean (SD) Mean (SD) MPI defect size [P = 0.12] Cardiac event4.1% (6.6%) No cardiac event 1.4% (2.2%) Negative predictive value Negative predictive value of having a normal MPI = 98% (401of 409).](http://images.slideplayer.in.th/7/1885800/slides/slide_28.jpg " Positive predictive value 6% (7 of 113) of patients for any MPI abnormality 12% (4 of 33) of patients for moderate or large MPI defects..")
29
Cardiac event +veCardiac event - ve Test + ve7106 Test - ve8401

33
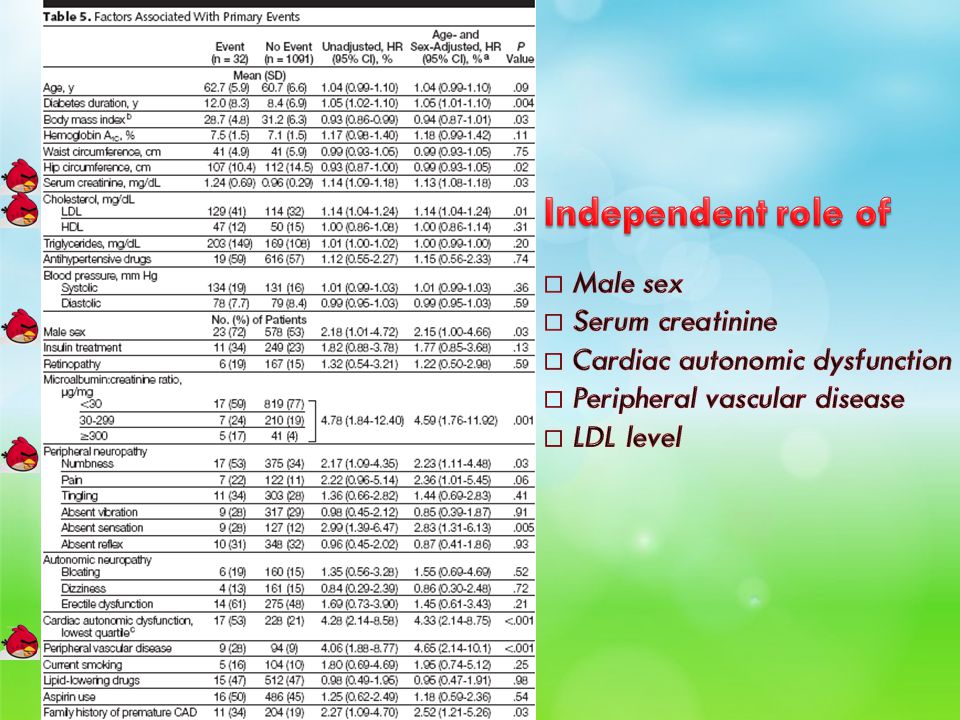
Male sex Diabetes duration Microalbuminuria/proteinuria Serum creatinine Symptomsof peripheral neuropathy Diminished peripheral sensation Cardiac autonomic dysfunction Peripheral vascular disease Elevated LDL Family history of premature CAD Male sex Diabetes duration Microalbuminuria/proteinuria Serum creatinine Symptomsof peripheral neuropathy Diminished peripheral sensation Cardiac autonomic dysfunction Peripheral vascular disease Elevated LDL Family history of premature CAD

35
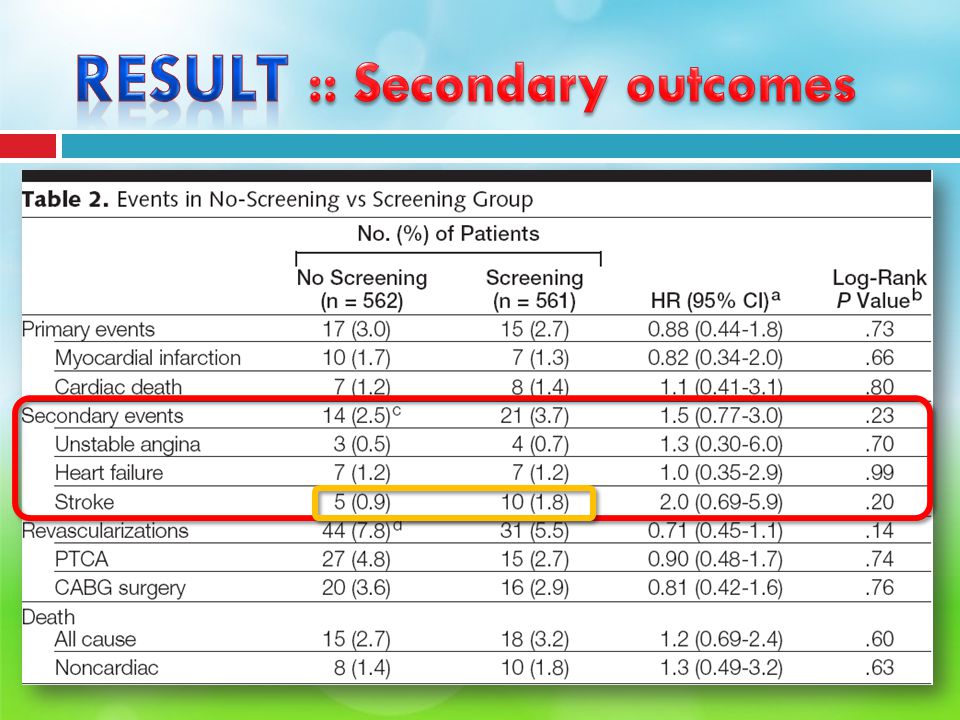
How large was the screening effect? Hazard Ratio =0.88 Relative Risk = 2.7%/3.0% = 0.9 Absolute Risk Reduction = 3.0%-2.7% = 0.3% Relative Risk Reduction = 1.0-0.9 = 0.1 or 10% Number Needed to Screen = 1/0.003 = 333

36
How precise was the estimate of the treatment effect?

37
Cardiac event rates ในประชากรที่ศึกษา 0.6% per year อัตราน้อยกว่าที่คาดการณ์ไว้ เห็นผลการเกิด cardiac event จากการคัดกรองได้ไม่ชัดเจน อัตราต่ำกว่าบางการศึกษาอื่นที่มีมาก่อน (retrospective analysis; cardiology laboratories) 3-4 เท่า เนื่องจาก ประชากรในการศึกษาอื่นนั้นๆ มี risk มากกว่า อัตราใกล้เคียงกับ 3 การศึกษาในการ screening asymptomatic ischemia in type 2 DM ACCORD study = 1.4% per year มีการกำหนด primary outcome definition, selection older patient with specific additional risk
 3-4 เท่า เนื่องจาก ประชากรในการศึกษาอื่นนั้นๆ มี risk มากกว่า อัตราใกล้เคียงกับ 3 การศึกษาในการ screening asymptomatic ischemia in type 2 DM ACCORD study = 1.4% per year มีการกำหนด primary outcome definition, selection older patient with specific additional risk")
38
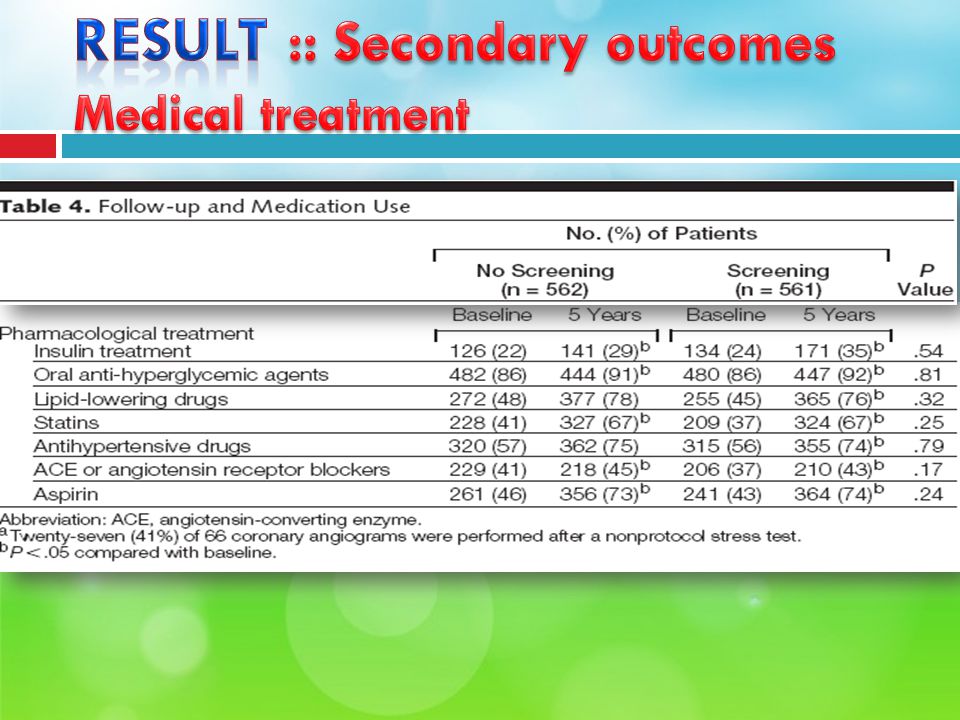
ความผิดปกติที่ตรวจพบจากการทำ MPI สัมพันธ์กับ อุบัติการณ์การเกิด cardiac event แม้ว่าจะมี PPV ต่ำ และยังมีโอกาสเกิด cardiac event ได้แม้ในคนที่ผล MPI ปกติ Cardiac outcomes ที่ดี เกิดจาก Aggressive guideline-driven management of cardiac risk factor การ screen ซ้ำที่ 3 ปี พบว่ามี resolution of inducible ischemia

39
ผู้ป่วยที่คาดว่าจะมี intermediate cardiac risk Long-standingdiabetes Older age Obesity ผู้ป่วยที่คาดว่าจะมี high cardiac risk Poor ability to exercise จากผล PPV, NPV พบว่ามากกว่าครึ่งหนึ่งของ cardiac event เกิดใน normal screening test

40
Cardiac event rates were significantly lower than originally anticipated at the time of the design of the study Not have the power to exclude a small difference between the screened and unscreened participants Non protocol stress tests were done during F/U when clinically indicated in both groups Screening led to only a modest reduction in subsequent diagnostic testing In no-screening group : crossover to a physician-direct screening strategy and theoretically

41
Clinical implications Routine screening for inducible ischemia in asymptomatic patients with type 2 DM cannot be advocated Yield of detecting significant inducible ischemia is relatively low. Overall cardiac event rate is low. Routine screening does not appear to affect overall outcome. Routine screening of millions of asymptomatic diabetic patients would be prohibitively expensive

42
Will the results help me in caring for my patient?

43
Screening criteria CriteriaThis study The burden of suffering Death, Disease, Disability, Discomfort, Dissatisfaction, Destitution The quality of screening test Sensitivity and specificity, Simplicity, Safety, Cost Effectiveness of Treatment Cost-effectiveness Longevity

งานนำเสนอที่คล้ายกัน






![คำสั่ง DISPLAY รูปแบบที่ 1 DISPLAY identifier-1, identifier-2 … literal-1 literal-2 [ UPON mnemonic-name ] ตัวอย่าง DISPLAY STUDENT-NAME. DISPLAY.](/7/1925791/big_thumb.jpg "คำสั่ง DISPLAY รูปแบบที่ 1 DISPLAY identifier-1, identifier-2 … literal-1 literal-2 [ UPON mnemonic-name ] ตัวอย่าง DISPLAY STUDENT-NAME. DISPLAY.>")












 MICU 68% CCU 32%>")


