ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Interesting case 14/6/50

2
History ผู้ป่วยหญิงไทยคู่อายุ 45 ปี อาชีพ ทำนา ภูมิลำเนา จ.ขอนแก่น
CC : ขาทั้งสองข้างอ่อนแรงมากขึ้น 10 วัน PI : 3 เดือน PTA : มีอาการอ่อนแรงที่ขาสองข้าง ยกขาได้ทั้งสองข้างแต่เวลาเดินต้องเดินลากขา ไม่มีอาการชา ปัสสาวะอุจจาระปกติ ไม่มีเดินเซ ไม่มีไข้ ไม่มีปวดศีรษะ ไม่มีความรู้สึกตัวเปลี่ยนแปลง ไม่ปวดหลัง ไปรักษารพ.ศูนย์ขอนแก่น follow up มาตลอด Rx ให้ Rivotril / Folic หลังได้รับการรักษา ญาติให้ประวัติว่ามีหกล้มหลายครั้ง และ มีปัสสาวะราดกลั้นไม่ได้บางครั้ง แขนมีแรงดีทั้งสองข้าง

3
History PH : มีประวัติเคยมีก้อนที่หน้าท้อง (Abdominal wall mass ) ขนาด
6 อาทิตย์ PTA : อาการเป็นมากขึ้น ญาติเริ่มบอกว่าผู้ป่วยมีหลงลืมเป็นบางครั้ง อาการมากไม่หาย 10 วัน PTA : อาการเป็นมากขึ้นจนช่วยเหลือตัวเองไม่ได้ นั่งไม่อยู่ จะล้มไปทางด้านหลังตลอด มีปัสสาวะราดบ่อยขึ้น PH : มีประวัติเคยมีก้อนที่หน้าท้อง (Abdominal wall mass ) ขนาด 5 x 5 cm ได้ excision เป็น Pus 10 cc ส่งเพาะเชื้อ ไม่ได้มาฟังผล ไม่มี underlying disease อื่น ๆ
 ขนาด. 5 x 5 cm ได้ excision เป็น Pus 10 cc ส่งเพาะเชื้อ ไม่ได้มาฟังผล. ไม่มี underlying disease อื่น ๆ.")
4
Physical examination A thai female, good conscious
V/S BT 37oC BP 130/70 mmHg RR 20 bpm PR 80 bpm HEENT : not pale, no jaundice no OC / no OHL CLN negative Lung : clear, no adventitious sound

5
Physical examination Abdomen : soft not tender,
surgical scar at low midline, no hepatosplenomegaly Ext : no edema, no PPE Neuro : E4M6V5, good orientation, memory = impair recall slow response to command/question,

6
Physical examination CN : intact all
Motor : normal volume, rigidity both legs grade V all Sensory : intact all modality Reflex : generalized hyperreflexia Cerebellar sign : impair FTN / HTS , no dysdiadochokinesia Rhomberg positive, tandem positive BKK – plantar response both Clonus – negative both sides

7
Physical examination Cortical lobe sign – negative Gait : Other
Difficult in initiating Magnetic gait Other Can’t sustain upright position

8
Problem list 1. gait instability 2. parkinsonism
3. urinary incontinence 4. impair recall memory 5. Hx of abdominal mass

9
Gait instability Paresis : weakness Ataxia Apraxia

10
Parkinsonism - cockwheel rigidity - bradykinesia - tremor
- postural instability - response to levodopa

11
Parkinsonism Parkinson disease ≠ Parkinsonism
Reversible VS Irreversible Reversible Drug induced – anti-DA Vascular Normal Pressure Hydrocephalus Wilson’s disease Post-encephalitis

12
Parkinsonism Irreversible Parkinson disease Parkinson plus syndrome
+ long tract sign = SND + cerebellar sign = OPCD + Autonomic = shy-drager + limited EOM = PSP + alien limb syndrome = CBD + ALS = MSA

13
CBC Hb 14.4 Hct 42.3% WBC 9700 Platelet 302,000 Neu 66 % L 26.8 %
M 5.9 % E 0.8 % Platelet 302,000

14
Lab chemistry BUN 7.8 Cr 0.6 Na 140 K 4.1 HCO3 30 Cl 102
Chol TB/DB 0.2/0 ALT/AST 15/25 ALP 51

15
CSF Rbc 10 CSF prot 346 Wbc 170 CSF sugar 19 Pressure 130
PMN 24 % L 68 % Pressure 130 India ink : negitive Crypto : +ve >100

16
Other Serum crypto Ag +ve C/S of pus Cryptococcus neoforman

17
Normal Pressure hydrocephalus

19
Ventricular system Foramen of Lushka / magendie Foramina of Monro
Aqueduct of Sylvius Foramen of Lushka / magendie

21
Classic triad Gait apraxia Urinary incontinence Dementia

22
Gait apraxia most responsive to shunting
a magnetic gait, gait apraxia, or a frontal ataxia parkinsonian gait – narrow base + response to visual / auditory cue

23
Cognitive impairment Apathy / depress / decrease attention
Cortical features = less prominent

24
Urinary incontinence First – secondary from gait apraxia
Late – lack of concern

25
Causes Idiopathic : identifiable ~ 50 : 50
idiopathic - most common in > 60 years Identifiable - all age groups Impair absorption ! Identifiable cause = SAH / post-trauma / Chronic meningitis

26
Differential diagnosis
Cortical predominate Dementia ! Alzheimer FTD DLB VaD CJD Subcortical predrom. Abnormal movement ! Parkinsonism DLB VaD Drug induced

27
Differential diagnosis
Diffuse process – involve both cortex / subcortex = dementia with parkinsonism Vascular dementia Dementia of lewy bodies Parkinson disease’s dementia

28
Diagnosis Exclude other condition Confirm diagnosis Evaluate prognosis

29
MMSE Only 5% of all dementia Hardly detect by MMSE
1. Absence of cortical dysfunction 2. Subcortical type of memory deficit (recall) 3. Frontal type mental deficit (apathy)
 3. Frontal type mental deficit (apathy)")
30
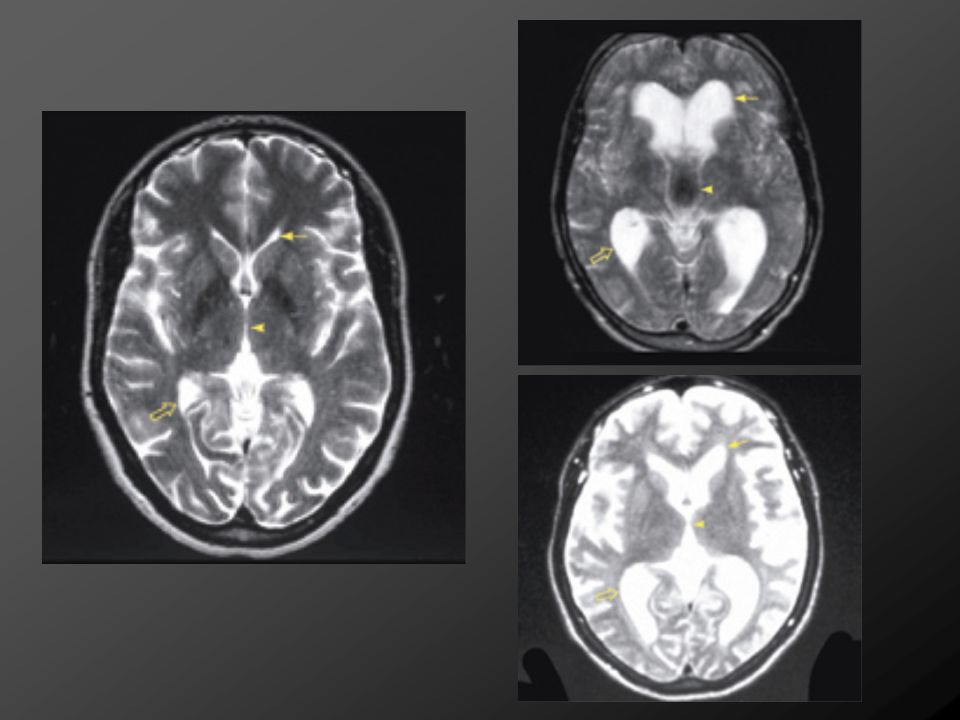
CT Ventricle enlarge disproportion to cerebral sulci
Predominate frontal & temporal Spare hippocampus

31
MRI Imaging of choice More detail on DDx ex. In alzeimer dz / white matter lesion / CSF voiding flow More detail on prognosis after Rx

33
CSF removal result in improvement of gait instability
40-50 cc removed per day cc per day of external lumbar drain for 3-5 days No clear definition of “improvement” Accuracy undetermined but easy to perform Can result in meningitis / subdural hematoma / radicular pain If response – 80% improve after shunt at 3 mo

34
Other tests Cisternography CBF study Hydrodynamic test
ICP monitoring – for B wave Lumbar infusion CSF conductance

35
Treatment CSF shunting Treat primary disease

37
Prognosis substantial improvement is
30–50% in idiopathic 50–70% in secondary NPH Dementia is the least likely to improve Peri/postsurgical complications ~ 20% and 40%, but serious complications do not exceed 5–8% ineffectiveness of the shunt should be suspected before document poor surgical outcome In mild case watchful waiting is not worse.

38
Progression 8 dec – 27 dec 28 dec Amphotericin B 0.8 mkd LP OD
V-P shunt was done

39
Non-HIV cryptococcus AIDS results in a higher burden of organisms and a diminished inflammatory response symptoms for a longer period of time, up to several months India ink +ve 75% in HIV 50% in non-HIV

40
Non-HIV cryptococcus Cell count Culture
Low in AIDs High in non-HIV Culture 90% in non-HIV nonHIV patients do not require chronic suppressive therapy A combination of amphotericin B (0.5 to 0.7 mg/kg per day) flucytosine (100 to 150 mg/kg per day in four daily doses) should be given for two weeks follow by oral fluconazole (400 mg/day) – 3 to 6 mo
 flucytosine (100 to 150 mg/kg per day in four daily doses) should be given for two weeks follow by oral fluconazole (400 mg/day) – 3 to 6 mo.")
41
Non-HIV cryptococcus Patients who die from cryptococcal meningoencephalitis Positive India ink examination of the CSF CSF WBC count <20/microL Initial CSF or serum cryptococcal antigen titer >1:32 Extraneural sites of infection High opening pressure on lumbar puncture

42
Non-HIV cryptococcus Patients who relapse after treatment
Persistently low CSF glucose concentrations after four weeks of therapy Low initial CSF white blood counts Posttreatment CSF or serum antigen titers of >1:8 Treatment with at least 20 mg of prednisone or its equivalent after the completion of therapy

43
T h a n k y o u

งานนำเสนอที่คล้ายกัน