ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Technique and US in hepatobiliary disease
US hepatobiliary system Technique and US in hepatobiliary disease พญ.เสาวลักษณ์ ชนม์ยืน รังสีแพทย์ โรงพยาบาลน่าน

2
Outline Anatomy US technique
Hepatobiliary tract disease( Liver, gallbladder and biliary tract )
")
3
Anatomy

4
ส่วนยอด บน ของ ตับ อยู่ที่ซี่โครงที่ 5 หรือ ต่ำกว่าราวนม ครึ่งนิ้ว

6
ท่อที่ผ่าน เข้า-ออก Liver
มี 4 ท่อ ดังนี้ 1. Hepatic Vein 2. Portal Vein 3. Bile Duct 4. Hepatic Artery

9
Hepatic segmental landmarks

10
Normal liver anAtomy -the ligamentum venosum (FL) separating the caudate lobe (C) and the left lateral segment (LL) -the ligamentum teres (LT)The left lateral segment (LL) and the left medial segment (LM) are separated by the ligamentum teres. -The interlobar fissure (IF) -The interlobar fissure and the gallbladder fossa separate the left medial segment (LM) from the right anterior segment (RA). -umbilical segment of the left portal vein (U)
The left lateral segment (LL) and the left medial segment (LM) are separated by the ligamentum teres. -The interlobar fissure (IF) -The interlobar fissure and the gallbladder fossa separate the left medial segment (LM) from the right anterior segment (RA). -umbilical segment of the left portal vein (U)")
11
Biliary system

12
Technique

13
Upper Abdominal Ultrasonography
supine position นอนหงาย left lateral decubitus position นอนตะแคง เอาด้านซ้ายลง right lateral decubitus position นอนตะแคง เอาด้านขวาลง

16
วาง probe เอียงไปทาง ด้านซ้าย
STOMACH ศีรษะ เท้า

17
เอียง probe จากด้านซ้าย มาเกือบกึ่งกลาง
stomach Aorta

18
เห็น aorta and branches

19
เห็น pancreas ในการตรวจ
Sagittal view in epigastrium

20
เลื่อน probe ผ่านกึ่งกลาง มาทางขวา

21
Caudate lobe IVC

22
Ligamentum teres

24
เอียง probe ขึ้น ไปทางศีรษะ จะเห็นหัวใจ

25
เลื่อน probe ลงมาจะเห็น pancreas

27
Hepatic veins เทเข้า IVC

28
IVa II VIII VII

29
RHV LHV MHV

30
Portal vein Periportal fibrofatty tissue produces brighter echoes around the portal veins Normal size ไม่ควรเกิน 13 mm ถ้ามากกว่านี้ให้สงสัยว่ามีภาวะ portal hypertension

31
Main portal vein แยกเป็น right และ left portal veins

32
IVC H

36
Gallbladder GB PV

37
Dilated CBD

40
Branches of Right Portal vein
VIII VI VII

42
Right subcostal section in left lateral decubitus position
ท่าตะแคงจะทำให้ ตับเลื่อนลงมา เราจะเห็น lesion บางอย่างที่ ท่านอนหงาย มองไม่เห็น

45
The liver

46
Liver Size - Right MCL วัด craniocaudal direction ขนาดน้อยกว่า 15 cm
Indirect signs of hepatomegaly extension of the right lobe below the lower pole of the kidney rounding of the inferior tip of the liver extension of the left lobe into the LUQ above the spleen

47
Liver mass /Focal lesion
Liver abnormality Parenchymal disease -Fatty liver -Liver cirrhosis -Periductal fibrosis Liver mass /Focal lesion

48
Liver parenchyma Homogeneous echogenicity โดยที่ echogenicity of the liver ≥ renal cortex, < renal capsule < spleen, < pancreas Smooth surface Visible tubular structuresare hepatic veins and portal veins Hepatic veins ; thin wall IVC Portal vein ; thick wall hepatic hilum Bile duct parallel with portal vein seen at porta hepatis

49
Diffuse hepatic inhomogeneity
COMMON -cirrhosis -metastasis -fatty infiltration UNCOMMON -hepatocellular cancer -hepatic fibrosis -lymphoma

50
Fatty infiltration เทียบกับ kidney and pancreas
Intracellular deposition of triglycerides within hepatocytes Causes – Alcoholic ,Steroid ,DM,Drug NASH ( Nonalcoholic Steatohepatitis ) = Severe fatty liver with hepatomegaly with inflammation and fibrosis Findings - Increased echogenicity of the liver, finer echotexture than normal liver เทียบกับ kidney and pancreas ปกติ liver ขาวกว่า kidney เล็กน้อย ถ้า fatty infiltrate จะเห็นเนื้อตับกับไตแยกจากกันชัดเจน ปกตื liver จะดำกว่า pancreas ถ้า fatty infiltrate เนื้อตับจะขาวกว่า
 = Severe fatty liver with hepatomegaly with inflammation and fibrosis. Findings - Increased echogenicity of the liver, finer echotexture than normal liver. เทียบกับ kidney and pancreas. ปกติ liver ขาวกว่า kidney เล็กน้อย ถ้า fatty infiltrate จะเห็นเนื้อตับกับไตแยกจากกันชัดเจน. ปกตื liver จะดำกว่า pancreas ถ้า fatty infiltrate เนื้อตับจะขาวกว่า.")
51
Fatty Infiltration Sensitivity 60-94 % Specificity 66-95 %
Diffuse - Grading -mild = mildly increasing echogenicity -moderate = blurring of veins margins -severe = significant of posterior shadowing Focal fatty infiltration

52
Diffuse Fatty liver grading
1.Normal 2.Mild - increasing echogenicity 3.Moderate - increasing echogenicity ,impaired visualised hepatic vessels and diaphragm 4.Severe - markedly increasing liver echogenicity with poor penetration, poor visualised hepatic vessels and diaphragm

53
Focal fatty sparing Focal Fatty infiltration
Focal fat infiltration Focal fatty sparing Diffuse fatty infiltration with FFS Geographic hypoechoic area Usually located in front of the RPV or PV bifurcation or around the gallbladder Lack of mass effect on hepatic vessels Focal or nodular Anterior aspect of LL (esp. medial segment), adjacent to the falciform ligament, anterior to the PV bifurcation Atypical locations metastases or hemangioma
, adjacent to the falciform ligament, anterior to the PV bifurcation. Atypical locations metastases or hemangioma.")
54
Focal fatty sparing Focal fat sparing at preportal and gallbladder fossa regions

55
Focal fatty infiltration
2 ภาพแรกเทียบเนื้อ liver VS kidney, liver VS spleen/// บรรยายภาพที่ 3 attenuation of the sound beam with progressive decreased echogenicity of the deeper aspects of the liver, indicating more advanced fatty infiltration Multiple focal nodular areas of increased echogenicity Focal fat infiltration No mass effect Focal nodular fatty infiltration

56
Cirrhosis US appearance Surface nodularity reliable sign
Coarsening and nodularity of the liver parenchyma(RN/DN) Segmental hypertrophy/atrophy Hypertrophy of the caudate lobe and lateral segments of left lobe (S2&3) Atrophy of the posterior segments (S6&7) of the right lobe RL:LL(longitudinal ratio) < 1.3 (normal =1.44) Signs of portal hypertension
 Segmental hypertrophy/atrophy. Hypertrophy of the caudate lobe and lateral segments of left lobe (S2&3) Atrophy of the posterior segments (S6&7) of the right lobe. RL:LL(longitudinal ratio) < 1.3 (normal =1.44) Signs of portal hypertension.")
57
Sonographic signs of portal hypertension
Ascitis Splenomegaly Portal vein enlargement >13 mm Portosystemic collateral Enlarged hepatic arteries Hepatofugal(reversed)portal flow
portal flow.")
58
Liver CIRRHOSIS diffuse heterogeneity
and nodularity to the liver parenchyma surface nodularity Liver CIRRHOSIS multiple nodular impressions on the hepatic vein lumen Scattered multifocal hypoechoic nodules

59
Liver abnormality Liver mass /Focal lesion Parenchymal disease
-Fatty liver -Liver cirrhosis -Periductal fibrosis Liver mass /Focal lesion

60
Echogenicity of liver mass /Focal liver lesion
Echogenic pattern - calcifications - anechogenic - hypoechogenic - isoechogenic - hyperechogenic - mixed echogenic Outline - well defined / poor Others - acoustic shadow - posterior enhancement - dilated bile duct

61
Calcifications

62
Calcification in the liver

63
Cysts Simple cyst Complex cyst Most common focal liver lesion
Anechoic lumen Increased through transmission A well-defined back wall Partial septation/ puckering of the wall Complex cyst Internal echoes Thick wall Septations that are numerous or thick Solid elements Calcification 2 รูปแรกเป็น simple cyst, รูปที่สามเป็น complex cyst

64
Causes of cystic lesions in the liver

65
Liver abscess Complex fluid collections with a mixed echogenicity
May mimic solid hepatic masses Thick-walled cystic lesions or cysts with fluid-fluid levels Gas forming abscess DDx: hematoma, hemorrhagic cyst, necrotic or hemorrhagic tumor

66
Liver abscess Large hypoechoic lesion with increased through transmission Complex cystic lesion Multiple small hypoechoic solid-appearing lesions Large heterogeneous, predominantly hyperechoic, lesion

67
Hemangioma Approximately 7% of adult, F>M, 10% are multiple
Typical appearance (60-70%) homogeneous round/lobulated hyperechoic mass usually less than 3 cm sharp&smooth margins calcification มีได้ แต่ rare Atypical hemangiomas Hyperechoic periphery and a hypoechoic center “reverse target” appearance Hemangioma ไม่ค่อยมี flow แต่ถ้าก้อนนั้นมี flow ให้สงสัย HCC or metastasis
 homogeneous. round/lobulated. hyperechoic mass. usually less than 3 cm. sharp&smooth margins. calcification มีได้ แต่ rare. Atypical hemangiomas. Hyperechoic periphery and a hypoechoic center reverse target appearance. Hemangioma ไม่ค่อยมี flow แต่ถ้าก้อนนั้นมี flow ให้สงสัย HCC or metastasis.")
68
Typical Typical “reverse target” appearance Atypical

69
Hemangioma Usually stable over time ~ 10% decrease in echogenicity
~ 5% regress partially or completely ~ 2% enlarge

70
DDx hyperechoic masses
Hemangioma Metastasis Hepatocellular cancer Focal fatty infiltration ถ้าผป มีประวัติ extrahepatic malignancy หรือ history of chronic liver disease ก่อนจะ Dx hemangioma ควร confirm ด้วย CT or MRI แต่ถ้าคนไข้ไม่มี risk factors ก็ไม่จำเป็นต้องตรวจอย่างอื่นเพิ่ม

71
Hepatocellular carcinoma
Strongly associated with chronic liver diseasehepatitis B&C and cirrhosis Growth pattern of HCC solitary, multifocal or diffuse and infiltrating Typical a large dominant lesion with scattered smaller satellite lesions Sonographic appearance non-specific Venous invasion 30-60% for the portal veins and 15% for the hepatic veins

72
Hepatocellular carcinoma
Pic 3-17

73
Hepatocellular carcinoma
Diffusely infiltrating tumor Intense hypervascularity typical of HCC

74
Metastases 98% multiple Usually involve both lobes of the liver
Variety of sonographic appearance ส่วนใหญ่จะเห็นเป็น “target appearance” echogenic/isoechoic center and a hypoechoic halo Others: hypo/hyperechoic nodule, calcified metastases, cystic metastasis, diffuse heterogeneous

75
target appearance Echogenic/isoechoic center and a hypoechoic halo

76
Hepatic target lesions
Target lesions are much more likely to be malignant than benign

77
Other focal liver lesion
Benign - Focal nodular hyperplasia hypoechogenic mass with central scar F > M - Hepatic adenoma hyperechogenic with central hypoechogenic area heterogenous echogenicity Malignant CHCA,Biliary cystic tumor

78
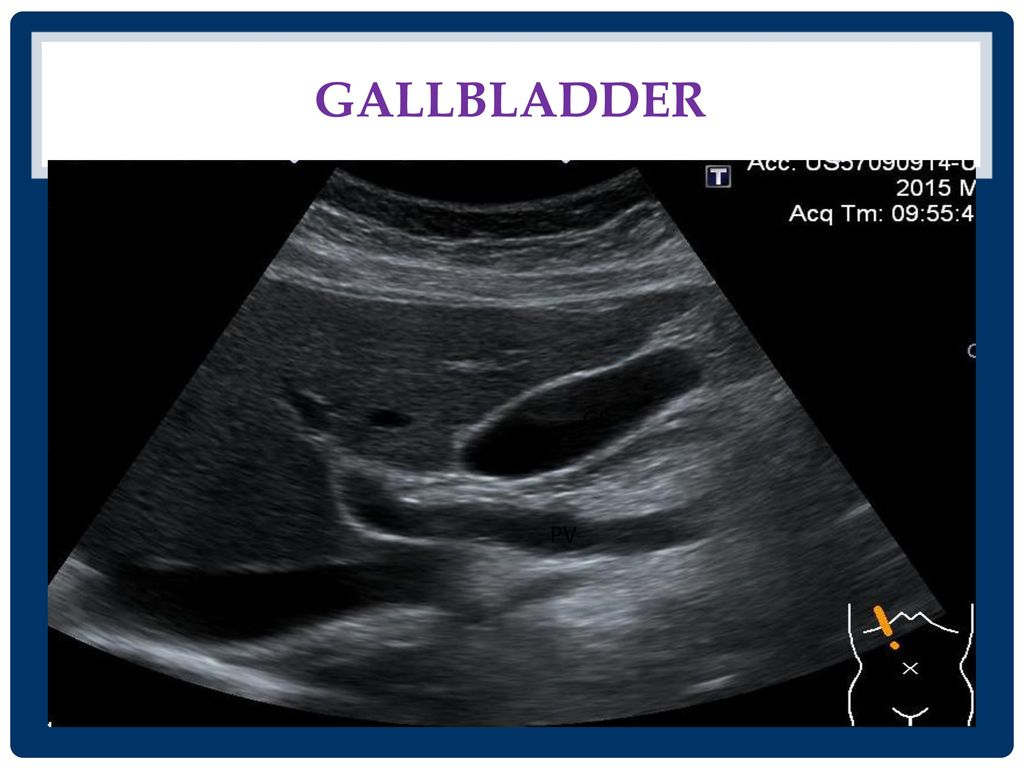
Gallbladder

79
The gallbladder อยู่ใต้ interlobar fissure
ใช้เป็น landmark for identifying the junction between the left and right lobes of the liver งดน้ำงดอาหาร ประมาณ 4-6 ชั่วโมงadequate gallbladder distention + reduce upper abdominal bowel gas

80
Transverse view GB อยู่ใต้ interlobar fissure ligamentum teres

81
The gallbladder GB PV

82
Characteristics of the normal gallbladder

84
Gallbladder Pathology
stones biliary sludge/ microlithiasis polyp contracted gallbladder porcelain gallbladder gallbladder wall thickening acute cholecystitis Chronic cholecystitis Hyperplastic cholecystitis carcinoma of gallbladder

85
Intraluminal abnormalities in the GB

86
Gallstone Accuracy 96% -echogenic foci -movable
-posterior acousticshadow

87
sludge Sludge and GS Sludge ball polyp

88
GB polyp Benign 95% m/c cholesterol polyp

89
Gallbladder polyp Benign size 5 mm-benign 5-10 mm FU pedunculated
m/c multiple stable size Malignant size >10 mm(37-88%) sessile single increasing in size
 sessile. single. increasing in size.")
90
acute cholecystitis GB wall thickening > 3 mm GB enlargement
Pericholecystitic fluid +/- Gall stone US Murphy’s sign positive

91
GB distension GB wall thickening GS&sludge Pericholecystic fluid collection

92
GB wall thickening Biliary cause Cholecystitis Adenomyomatosis Cancer
AID cholangiopathy Sclerosing cholangitis Non biliary cause Hepatitis Pancreatitis Heart failure Cirrhosis Hypoproteinemia Lymphatic obstruction Portal hypertension

93
Other gallbladder Disease
Adenomyomatosis - Intramural diverticular diffuse or focal thickening GB wall Carcinoma GB - Focal or diffuse thickenedwall Polypoid maa GB mass

94
Biliary system

95
The bile duct จะวิ่งขนานไปกับ portal veins & hepatic arteries
Intrahepatic bile duct จะวิ่งขนานไปกับ portal veins & hepatic arteries anterior to the adjacent portal veins IHD ส่วนใหญ่จะตรวจไม่พบใน US หรือถ้าพบก็มักจะมีขนาดไม่เกิน 2 mm

96
The bile duct Extrahepatic bile duct
US ไม่สามารถบอกตำแหน่งของ cystic duct มาเทเข้าได้ จึงบอกไม่ได้ว่าท่อน้ำดีที่ขั้วตับนั้นเป็น CBD or CHD ดังนั้นจึงเรียกกลางๆเป็น common duct common duct < 7 mm วัดจากขอบด้านในของด้านหนึ่งไปอีกด้านหนึ่ง

97
The bile duct The hepatic artery จะอยู่ anterior to the portal vein และ medial to the common duct

98
Mickey Mouse appearance

99
Right hepatic artery จะวิ่งระหว่าง portal vein and common duct

100
RIGHT HEPATIC ARTERY CHD HEPATIC ARTERY PROPER CBD PORTAL VEIN

101
Biliary dilatation Intrahepatic duct -larger than 2 mm diameter
-more than 40% diameter of the adjacent portal vein

102
Biliary dilatation Intrahepatic duct -larger than 2 mm diameter -more than 40% diameter of the adjacent portal vein Extrahepatic duct -CHD 4-5 mm -CBD 4-6 mm 6-7 mm equivocal >8 mm indicate ductal dilatation may be tortous or irregular wall

103
tortuous configuration
parallel channel sign Irregular appearance tortuous configuration Posterior enhancement

104
Biliary dilatation อาจจะไม่พบ ductal dilatation 4-6 mm
Extrahepatic duct - CHD 4-5 mm - CBD วัดจากขอบด้านในของด้านหนึ่งไปอีกด้านหนึ่ง 4-6 mm 6-7 mm equivocal >8 mm indicate ductal dilatation Elderly patients and in postcholecystectomy patients อาจพบ common duct dilatation ได้ถึง 9-10 mm Acute, intermittent, and partial obstruction อาจจะไม่พบ ductal dilatation

105
Dilated CBD

107
Choledocholithiasis/stone
Most common causes of biliary obstruction Intrahepatic duct stones less common than CBD stones Gall stone % ass.with CBD stone CBD stone ---95% ass. With GS

108
CBD stone

109
Intrahepatic duct stones
DDx IHD stones Intrabiliary gas/ pneumobilia Hepatic artery calcification

110
Pneumobilia brighter reflection and dirtier shadow than do stones
a ring-down artifact mobile on real time Intrahepatic arterial calcification two bright parallel lines

111
Bile duct wall thickening
Nonspecific finding Duct wall thickening > 5 mm and disproportionately dilated IHD suspicion of cholangiocarcinoma

112
Causes of bile duct wall thickening
Risk factor of CHCA > 5 mm and disproportionately dilated IHD Risk factor of CHCA

113
Increased periportal echo ( IPE )
Normal echo IPE

114
Increased periportal echo ( IPE )
")
115
Increased periportal echo (IPE) grading = Periductal fibrosis ( PDF)
IPE Grade 1 is diffuse echogenic foci (‘starry sky’) minimal wall thickening of portal and segmental branches IPE Grade 2 is Ring echoes around vessels in cross-section,pipe-stems parallel with portal vein IPE Grade 3 is echogenic ruff around portal bifurcation and main stem ;main portal vein vessels wall thickening
 minimal wall thickening of portal and segmental branches. IPE Grade 2 is Ring echoes around vessels in cross-section,pipe-stems parallel with portal vein. IPE Grade 3 is echogenic ruff around portal bifurcation and main stem ;main portal vein vessels wall thickening.")
116
Hypothesis Repeated infection with O. viverrini by consumption of fresh water fish Worms inhabit in biliary tree Chronic inflammation of biliary tree Periductal fibrosis ( PDF) Cholangiocarcinoma
 Cholangiocarcinoma.")
117
Cholangiocarcinoma

118
Ultrasonographic pattern of CHCA
1.Parenchymal mass 2.Dilatation of bile duct without mass 3.Parenchymal mass with dilated duct 4. Dilatation of bile duct with intraluminal mass

119
Dilatation of bile duct with intraluminal mass
Parenchymal mass Mass with ductal dilatation Dilatation of bile duct with intraluminal mass

120
Take home point Review anatomy
Middle hepatic vein is landmark for right and left lobe liver CBD and all bile duct runs parallel to portal vein Comparing echo pattern, liver echo > renal cortex Normal tubular structures visible in liver parenchyma are portal vein, hepatic vein

121
Take home point Cholangiocarcinoma have non-specific sonographic feature Important in surveillance US 1.abnormal echo mass lesion 2.dilatation of IHD or EHD PDF has protential to be sonographic sign to closely follow up in a risk group of CCA surveillance

122
ThaNk you

งานนำเสนอที่คล้ายกัน