ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
พญ.ปฏิมาวรรณ เขียนวงศ์
Shoulder dystocia !!! พญ.ปฏิมาวรรณ เขียนวงศ์ สูติแพทย์ รพ.พิจิตร
2
diagnosis จาก งานวิจัย
เก็บเวลาเฉลี่ยการคลอดปกติ 210 ราย (ที่ไม่ติดไหล่) จากหัว-ตัว ใช้เวลาเฉลี่ย 24 วินาที + 2SD = 60 วินาที จำกัดความว่า คลอด หัว-ตัว ใช้เวลานานเกิน 60 วินาที = ติดไหล่
 จากหัว-ตัว ใช้เวลาเฉลี่ย 24 วินาที + 2SD = 60 วินาที จำกัดความว่า คลอด หัว-ตัว ใช้เวลานานเกิน 60 วินาที = ติดไหล่")
3
พบว่า เคสที่เข้าเกณฑ์ข้างต้น มีลักษณะผลลัพธ์การคลอดคือ คือ
ทำวิจัยต่อ เคสที่เข้าเกณฑ์วินิจฉัยติดไหล่คือ ใช้เวลาคลอดหัว-ตัว นานกว่า 60 วิ หรือใช้หัตถการช่วยคลอด (นับตั้งแต่ McRobert, suprapubic pressure, posterior arm release) พบว่า เคสที่เข้าเกณฑ์ข้างต้น มีลักษณะผลลัพธ์การคลอดคือ คือ เด็กตัวโตกว่า มี apgar ต่ำกว่า มี birth trauma มากกว่า แต่ใน 99 รายที่เข้าเกณฑ์ มีเพียง 24 รายที่ได้รับการวินิจฉัยว่าติดไหล่โดยแพทย์ (ในเวชระเบียน) สรุปว่าการวินิจฉัยทำได้ยาก และข้อมูลมีความแปรปรวนมาก
 พบว่า เคสที่เข้าเกณฑ์ข้างต้น มีลักษณะผลลัพธ์การคลอดคือ คือ. เด็กตัวโตกว่า มี apgar ต่ำกว่า มี birth trauma มากกว่า. แต่ใน 99 รายที่เข้าเกณฑ์ มีเพียง 24 รายที่ได้รับการวินิจฉัยว่าติดไหล่โดยแพทย์ (ในเวชระเบียน) สรุปว่าการวินิจฉัยทำได้ยาก และข้อมูลมีความแปรปรวนมาก.")
5
Prediction and Prevention ?
The use of shoulder dystocia prediction models cannot be recommended.

6
Prevention A : Q : Does induction of labour prevent shoulder dystocia?
Induction of labour does not prevent shoulder dystocia in non-diabetic women with a suspected macrosomic fetus. Induction of labour at term can reduce the incidence of shoulder dystocia in women with gestational diabetes.

7
The NICE diabetes guideline recommends that pregnant women with diabetes who have a normally grown fetus should be offered elective birth through induction of labour, or by elective caesarean section if indicated, after 38 completed weeks. National Institute for Health and Clinical Excellence. Diabetes in pregnancy. Management of diabetes and its complications from pre-conception to the postnatal period. Clinical Guideline 63. London: NICE; 2008.

8
Q: Should elective caesarean section be recommended for suspected fetal macrosomia to prevent brachial plexus injury (BPI)? A: Elective caesarean section should be considered for pregnancies complicated by pre-existing or gestational diabetes, with an estimated fetal weight of greater than 4.5 kg.

9
Q: What is the appropriate mode of delivery for the woman with a previous episode of shoulder dystocia? A: Either caesarean section or vaginal delivery can be appropriate after a previous shoulder dystocia. The decision should be made jointly by the woman and her carers.

11
HELPERR H : call for help E : Evaluate for episiotomy
L : Leg : McRobert maneuver P : External pressure E Enter : rotational maneuver R : Remove the posterior arm R : Roll the patient to her hand and knees

12
Preparation in labour:
what measures should be taken when shoulder dystocia is anticipated? All birth attendants should be aware of the methods for diagnosing shoulder dystocia and the techniques required to facilitate delivery.

13
Birth attendants should routinely look for the signs of shoulder dystocia. ● difficulty with delivery of the face and chin ● the head remaining tightly applied to the vulva or even retracting (turtle-neck sign) ● failure of restitution of the fetal head ● failure of the shoulders to descend.
 ● failure of restitution of the fetal head ● failure of the shoulders to descend.")
14
Initial step Team No pushing during preparation
No fundal pressure, excessive neck rotating, excessive traction Lithotomy position Generous episiotomy if needed Empty bladder

15
Avoid increasing traction Suprapubic pressure
Anterior shoulder Downward and lateral (toward fetal sternum) McRobert maneuver
 McRobert maneuver.")
16
McRobert maneuver with suprapubic pressure
17
McRobert’s Maneuver (Before) Shoulder Dystocia
ACOG Simulation Committee

18
McRobert’s Maneuver (After) Shoulder Dystocia
ACOG Simulation Committee

19
Suprapubic Pressure Shoulder Dystocia
ACOG Simulation Committee

20
ACOG Simulation Committee
Suprapubic Pressure ACOG Simulation Committee
21
McRobert maneuver with suprapubic pressure
22
No single method clearly superior than another
Second procedure No single method clearly superior than another

23
Rubin and Wood corkscrew maneuver
24
Rubin and Wood corkscrew maneuver
25
Posterior Rubin’s Maneuver Shoulder Dystocia
ACOG Simulation Committee

26
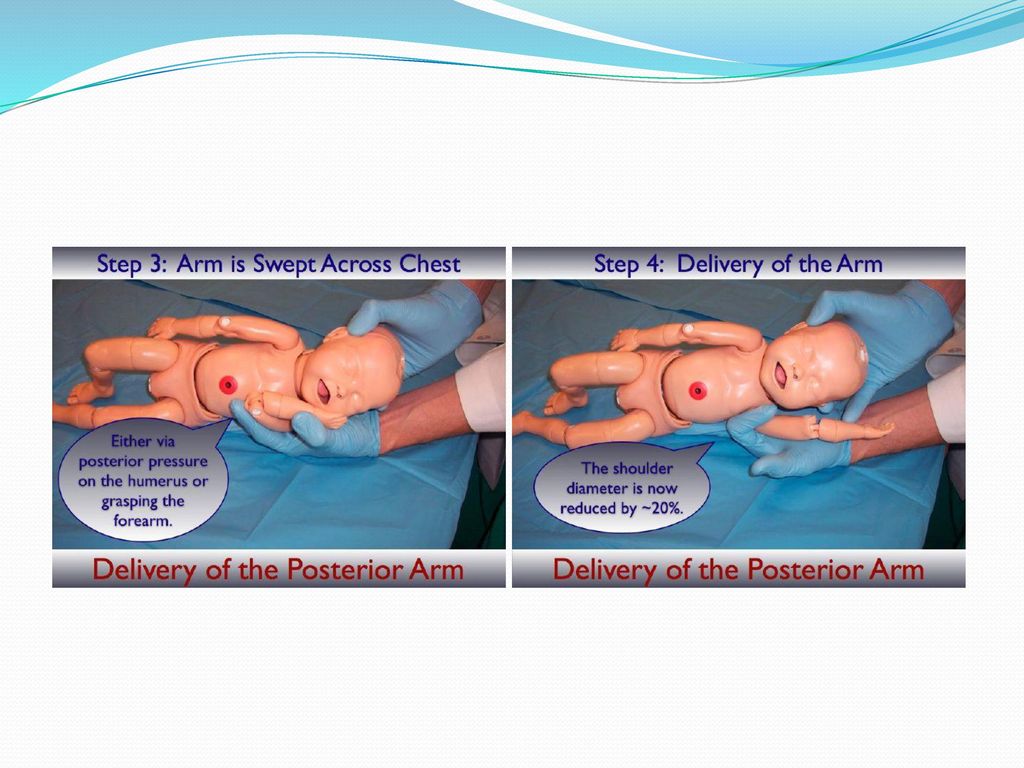
Delivery of posterior arm
Delivery of posterior shoulder Posterior axillary sling

27
Delivery of posterior arm
Posterior arm identified and follow to reach elbow Flexed elbow Grasp forearm and hand and pull out Extended elbow Pressure applied at antecubital fossa

28
ACOG Simulation Committee
Effect of Posterior Arm Delivery (reducing obstructing part of fetal shoulder) ACOG Simulation Committee
 ACOG Simulation Committee.")
30
Posterior Arm Delivery Shoulder Dystocia
ACOG Simulation Committee
31
Delivery of Posterior Arm (1 of 3) Shoulder Dystocia
ACOG Simulation Committee

32
Delivery of Posterior Arm (2 of 3) Shoulder Dystocia
ACOG Simulation Committee

33
Delivery of Posterior Arm (3 of 3) Shoulder Dystocia
ACOG Simulation Committee

34
Delivery of posterior shoulder
35
Posterior axillary sling
36
Extraordinary maneuvers
Fracture of the clavicle Cephalic replacement Abdominal rescue Symphysiotomy

37
Cephalic Replacement (1 of 2) Shoulder Dystocia
ACOG Simulation Committee

38
Cephalic Replacement (2 of 2) Shoulder Dystocia
ACOG Simulation Committee

39
Symphysiotomy
40
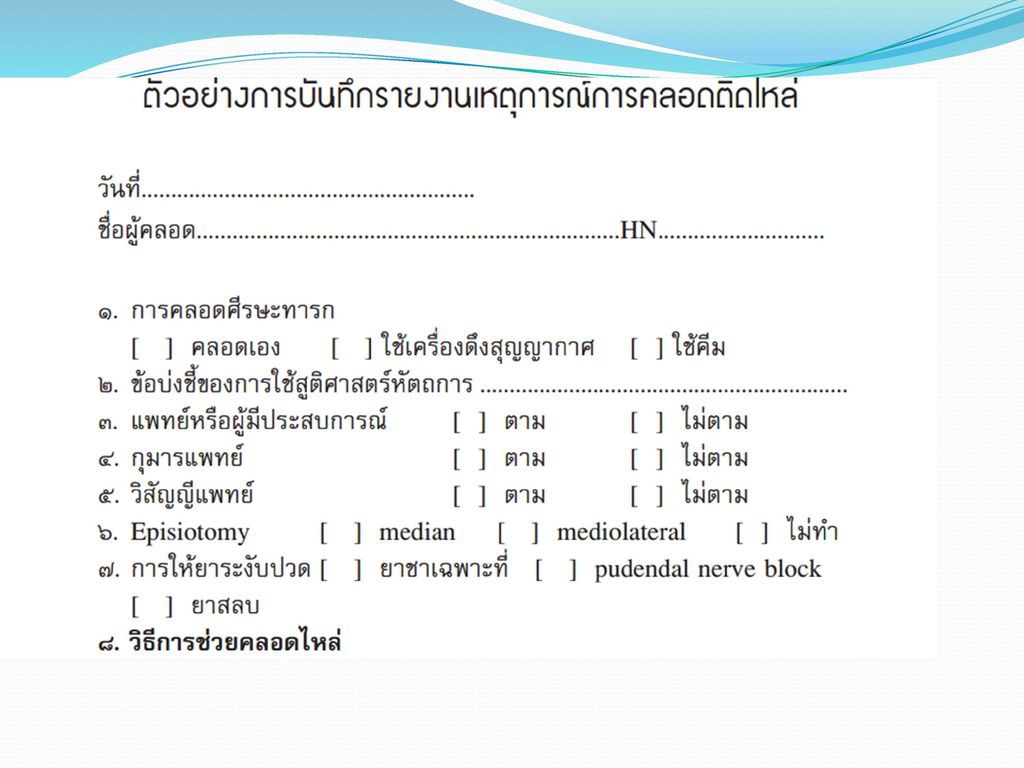
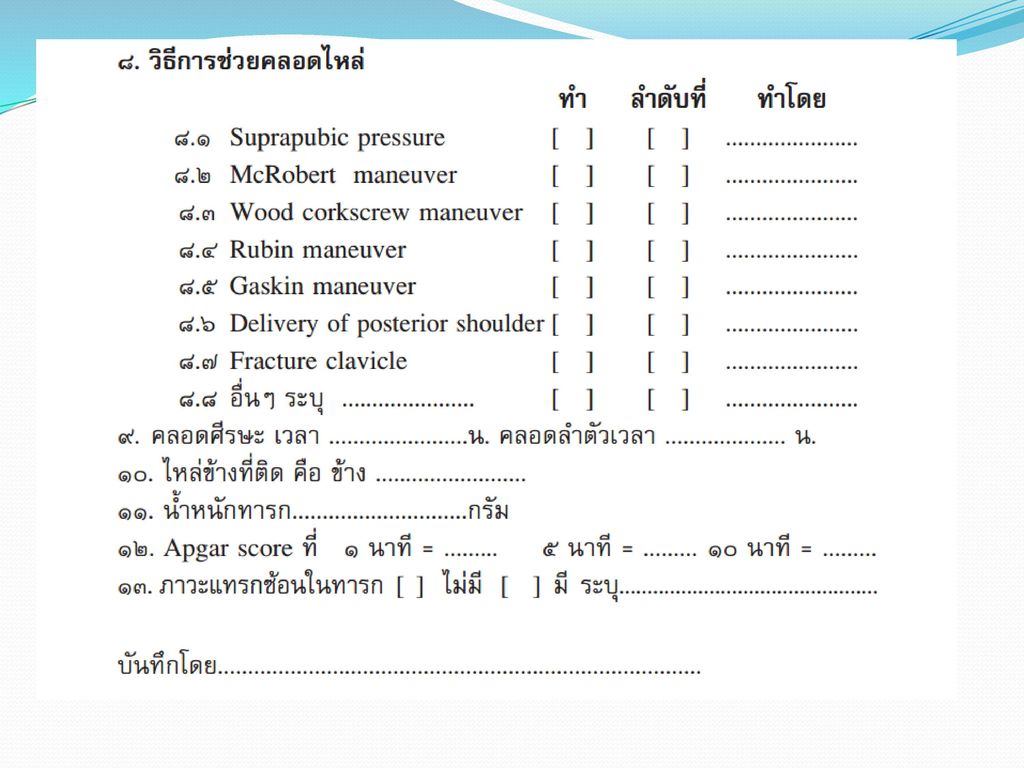
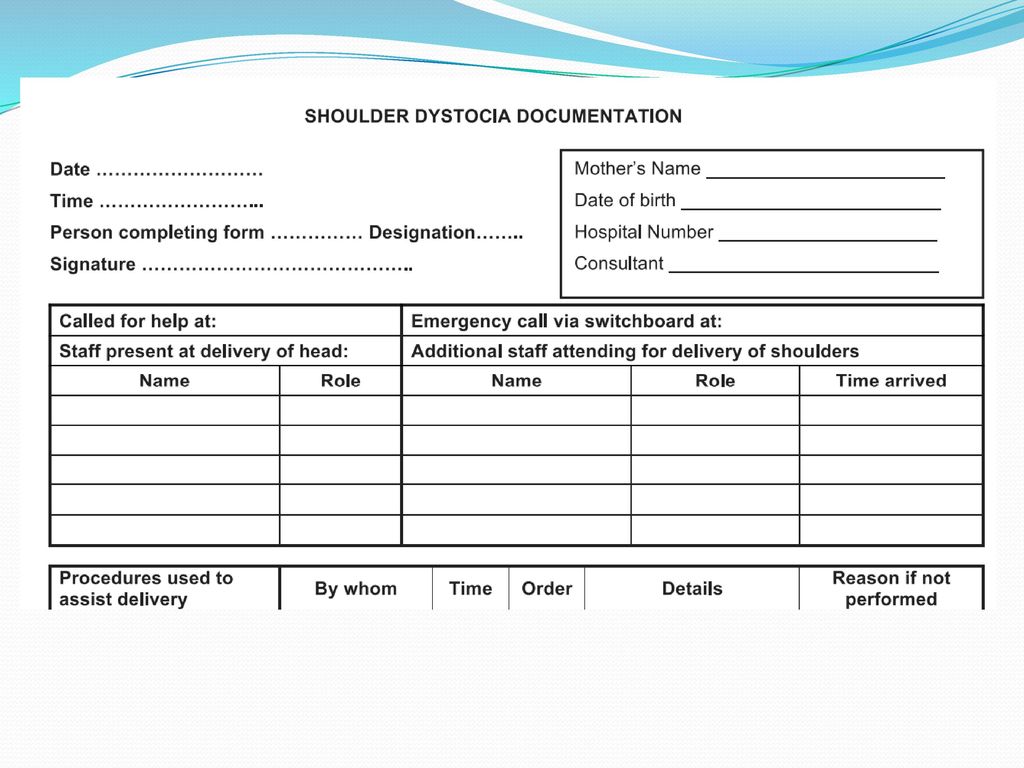
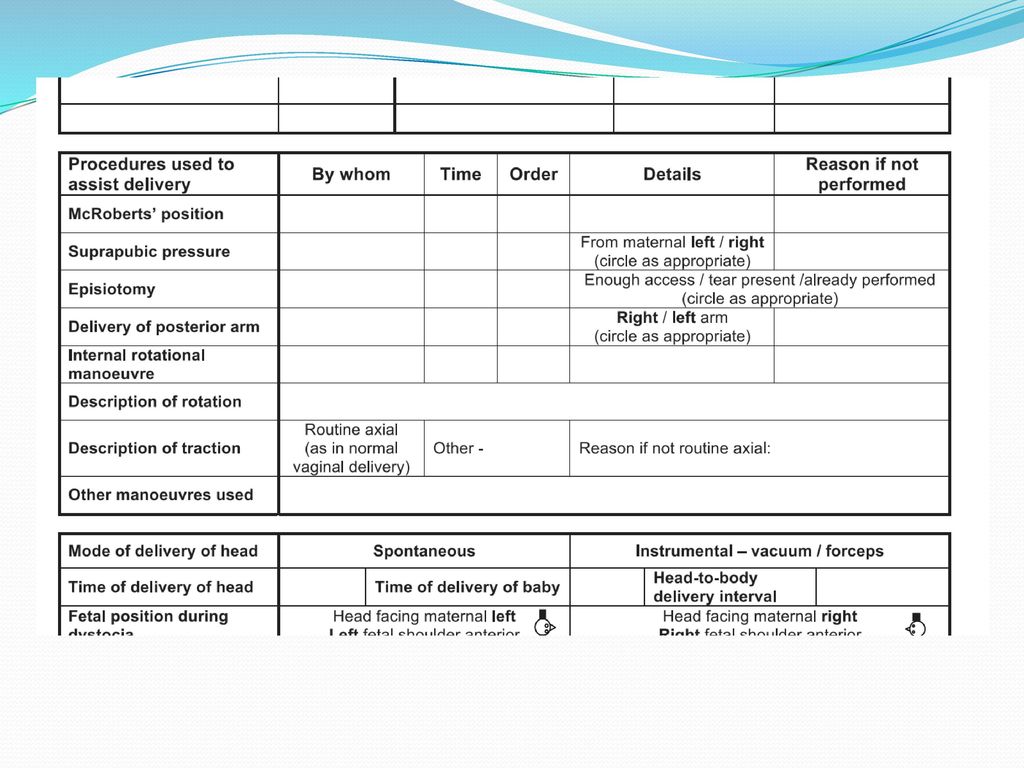
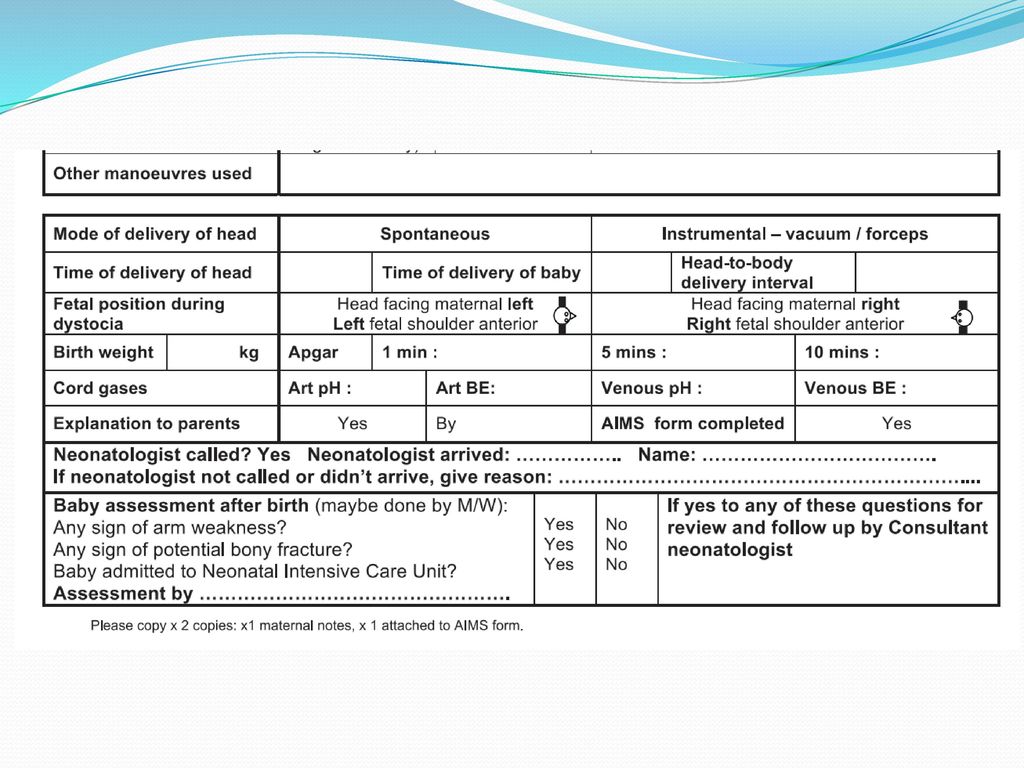
Documentation การบันทึกเหตุการณ์

46
การให้ข้อมูล มารดาและญาติ
ข้อเท็จจริงตามเหตุการณ์ ภาวะแทรกซ้อนที่เกิดขึ้น การรักษาและพยากรณ์โรค มารดา ตกเลือดหลังคลอด แผลฝีเย็บฉีกขาด Separation of pubic symphysis ทารก Birth asphyxia Birth trauma เฝ้าระวังภาวะซึมเศร้าหลังคลอด

47
Birth injury from shoulder dystocia
Fracture clavicle Heal in 1 month Fracture humerus Brachial plexus injury Erb’s palsy Klumpke’s palsy Total brachial plexus injury

49
Erb’s palsy
50
Prognosis of Erb’s palsy
Improve spontaneously in 6th-9th mo 10 % need treatment Physical therapy Surgery

51
ขอเล่าตอนท้องหน่อยนะคะ ตอนนั้นอายุ 28 สูง 158 นน. 62 อายุครรภ์ 38 w. นน.เพิ่ม 12 โล. แรกคลอดน้องออมตังค์ นน g. หมอบอกว่าที่ติดไหล่เพราะกระดูกเชิงกรานแม่แคบ ถ้าจะมีใครสักคนที่ผิด น่าจะเป็นตัวฉันเอง ครอบครัวของเราเชื่อเสมอมาว่า "ลูกของเราต้องดีขึ้น ไม่มีอะไรต้องห่วง" ตามที่หมอ(รพ.แรก ทั้งกลุ่มพากันบอกไว้) ฉันเชื่อและบอกกับทุกคนว่า "ฉันเชื่อใจหมอ ถึงมือหมอแล้ว ไม่ต้องห่วง น้องจะดีขึ้นในไม่ช้า"
 ฉันเชื่อและบอกกับทุกคนว่า ฉันเชื่อใจหมอ ถึงมือหมอแล้ว ไม่ต้องห่วง น้องจะดีขึ้นในไม่ช้า")
52
แต่ถึงตอนนี้ความเชื่อมั่น ความศรัทธา และความนับถือในใจของฉันมันหมดไปแล้ว ฉันไม่เชื่อ ไม่ศรัทธา ไม่แน่ใจ และไม่ไว้ใจสิ่งใดๆ ในโลกนี้แล้ว อยากบอกคุณหมอทุกคนว่า "ขอให้ท่านบอกกับคนไข้ไปตรงๆ ว่าเรากำลังเจอกับปัญหาอะไร แนวทางแก้ไขเป็นยังไง และเปอร์เซ็นความผิดพลาด หรืออะไรก็ได้ ที่มันทำให้เราต้องเผื่อใจไว้เจ็บ"

53
Risk management Q&A Training
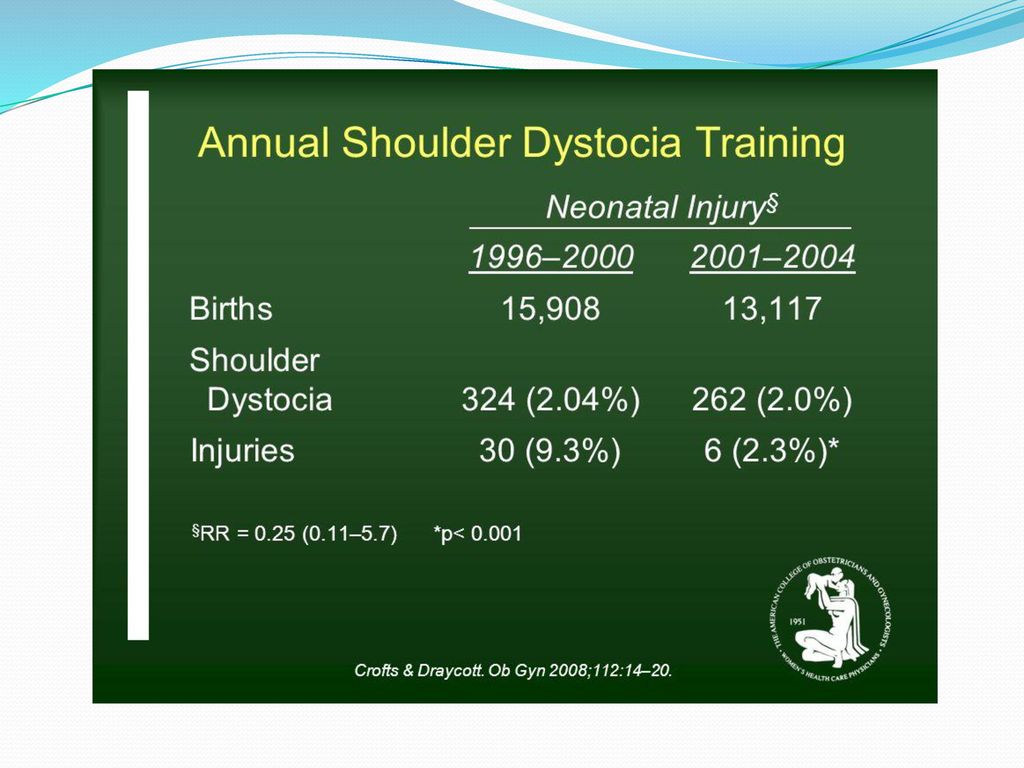
Q : What are the recommendations for training? A : All maternity staff should participate in shoulder dystocia training at least annually.

54
Q&A A : What is the evidence for the effectiveness of shoulder dystocia training? A : What measures can be taken to ensure optimal management of shoulder dystocia?

56
Internal rotation procedure 22/324 (6.8%) 29/262 (11.1%)
Techniques Pre train Post train McRobert 95/324 (29.3%) 229/262 (87.4%) Suprapubic pressure 90/324 (27.8%) 119/262 (45.4%) Internal rotation procedure 22/324 (6.8%) 29/262 (11.1%) Posterior arm delivery 24/324 (7.4%) 52/262 (19.8%) Excessive traction 54/324 (16.7%) 24/262 (9.2%)
 229/262 (87.4%) Suprapubic pressure. 90/324 (27.8%) 119/262 (45.4%) Internal rotation procedure. 22/324 (6.8%) 29/262 (11.1%) Posterior arm delivery. 24/324 (7.4%) 52/262 (19.8%) Excessive traction. 54/324 (16.7%) 24/262 (9.2%)")
งานนำเสนอที่คล้ายกัน