ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Chronic Kidney Disease
(CKD) นพ.พันธพงศ์ ตาเรืองศรี พบ., วว.อายุรศาสตร์, วว.อายุรศาสตร์โรคไต
 นพ.พันธพงศ์ ตาเรืองศรี พบ., วว.อายุรศาสตร์, วว.อายุรศาสตร์โรคไต.")
2
Renal Anatomy

3
Renal Anatomy

4
Renal Anatomy

5
Renal Function Excretory & Regulatory Synthetic
Solute : electrolyte & non-electrolyte Solvent : water Synthetic Erythropoietin RBC stimulation 1,25-(OH)2 Vitamin D3 (Calcitriol) Etc.
2 Vitamin D3 (Calcitriol) Etc.")
6
Renal Function GFR (90 ml/min./1.73 m2)
")
7
โรคไตเนโฟรติก (ไข่ขาวในปัสสาวะ)
ไตวาย ติดเชื้อ โรคไตเนโฟรติก (ไข่ขาวในปัสสาวะ) นิ่ว อื่นๆ เฉียบพลัน เรื้อรัง เรื้อรังระยะสุดท้าย กรวยไตอักเสบ กระเพาะปัสสาวะอักเสบ ไต ท่อไต กระเพาะปัสสาวะ SLE IgA Nephropathy etc.
 นิ่ว. อื่นๆ. เฉียบพลัน. เรื้อรัง. เรื้อรังระยะสุดท้าย. กรวยไตอักเสบ. กระเพาะปัสสาวะอักเสบ. ไต. ท่อไต. กระเพาะปัสสาวะ. SLE. IgA Nephropathy. etc.")
8
RENAL FAILURE Definition : ↓ Renal function
↓ GFR (Glomerular filtration rate) → ↓ Uremic toxin excretion → ↑ Serum BUN, Cr
 → ↓ Uremic toxin excretion. → ↑ Serum BUN, Cr.")
9
GFR Measurement 1. Direct clearance of substance
Inulin – Gold standard Radioisotope - 99mTc EDTA, 125I Iothalamate Creatinine – practical CCr (Cr Clearance) ~ GFR CCr (ml/min.) = UCr x V (urine volume) PCr
 ~ GFR. CCr (ml/min.) = UCr x V (urine volume) PCr.")
10
GFR Measurement 2. Formula Cockcroft-Gault MDRD CCr (ml/min)
= (140 - Age) x Body weight x (0.85 if Female) 72 x SCr MDRD eGFR (ml/min/1.73m2) = 186 x (SCr) x (Age) x (0.742 if Female) x (1.210 if African-American)
 x Body weight x (0.85 if Female) 72 x SCr. MDRD. eGFR (ml/min/1.73m2) = 186 x (SCr) x (Age) x (0.742 if Female) x (1.210 if African-American)")
11
2. Formula CKD-EPI – Recommended formula
GFR Measurement 2. Formula CKD-EPI – Recommended formula Serum Cr eGFR (ml/min/1.73m2) Female ≤ 0.7 144 × (Scr/0.7) × (0.993)Age > 0.7 144 × (Scr/0.7) × (0.993)Age Male ≤ 0.9 141 × (Scr/0.9) × (0.993)Age > 0.9 141 × (Scr/0.9) × (0.993)Age
 Female. ≤ × (Scr/0.7) × (0.993)Age. > × (Scr/0.7) × (0.993)Age. Male. ≤ × (Scr/0.9) × (0.993)Age. > × (Scr/0.9) × (0.993)Age.")
12
GFR Measurement

13
RENAL FAILURE ARF (Acute Renal Failure) CRF (Chronic Renal Failure)
↓ Renal function in hours to days CRF (Chronic Renal Failure) ↓ Renal function in > 3 months AKI (Acute Kidney Injury) CKD (Chronic Kidney Disease)
 ↓ Renal function in > 3 months. AKI (Acute Kidney Injury) CKD (Chronic Kidney Disease)")
14
Reversible ! ARF CRF Irreversible…

15
Clues in Diagnosis of CKD (from AKI)
Uremia > 3 months Previous high serum BUN, Cr Clinical : nausea, edema, hematuria, nocturia Small size kidneys : < 9 cm Anemia Renal osteodystrophy

16
Chronic Kidney Disease (CKD)
Definition: duration ≥ 3 months 1. Kidney damage Pathology Structure: Stone, Cyst, Mass, etc. Function: Proteinuria, Albuminuria Hematuria, Abnormal Cast And / Or 2. GFR < 60 ml/min/1.73 m2

17
Stages of CKD At increased risk 1 Kidney damage with normal GFR 2
Description GFR Action At increased risk ≥ 90 Screening, CKD risk reduction 1 Kidney damage with normal GFR Dx & Rx, Rx of comorbid condition, Slowing progression, CVD risk reduction 2 Kidney damage with mild GFR 60-89 Estimating progression 3 Moderate GFR 30-59 Assess & Rx complication 4 Severe GFR 15-29 Praparation for RRT 5 Kidney failure < 15 Renal replacement

18
CRF Stages of CKD At increased risk 1 Kidney damage with normal GFR 2
Description GFR Action At increased risk ≥ 90 Screening, CKD risk reduction 1 Kidney damage with normal GFR Dx & Rx, Rx of comorbid condition, Slowing progression, CVD risk reduction 2 Kidney damage with mild GFR 60-89 Estimating progression 3 Moderate GFR 30-59 Assess & Rx complication 4 Severe GFR 15-29 Praparation for RRT 5 Kidney failure < 15 Renal replacement CRF

19
Male, BW 60 Kg, Age 60 Serum Cr CKD-EPI Cockcroft-Gault CKD stage 1.3 59 51 3 2.5 27 4 5.0 12 13 5

20
Prevalence in THAILAND
Stages of CKD Stage Description GFR Prevalence in THAILAND 2550 At increased risk ≥ 90 1 Kidney damage with normal GFR 2 Kidney damage with mild GFR 60-89 3 Moderate GFR 30-59 4 Severe GFR 15-29 5 Kidney failure < 15 8.9 % 8.7 % (4,500,000 – Thai) (120,000 – ChiangMai)
 (120,000 – ChiangMai)")
21
CKD stage 1-2 → Asymptomatic !
Signs & Symptoms Uremic symptoms (รู้สึกไม่สบาย คลื่นไส้ เบื่ออาหาร) Anemia (โลหิตจาง), Fatigue (เหนื่อยง่าย อ่อนเพลีย) Dysuria (ปัสสาวะขัด), Nocturia (ปัสสาวะบ่อยตอนกลางคืน), Hematuria (ปัสสาวะมีสีแดง) Edema (บวม), ปัสสาวะน้อยลง ปวดหลัง ปวดเอว ความดันโลหิตสูง, เวียนศีรษะ CKD stage 1-2 → Asymptomatic !
 Anemia (โลหิตจาง), Fatigue (เหนื่อยง่าย อ่อนเพลีย) Dysuria (ปัสสาวะขัด), Nocturia (ปัสสาวะบ่อยตอนกลางคืน), Hematuria (ปัสสาวะมีสีแดง) Edema (บวม), ปัสสาวะน้อยลง. ปวดหลัง ปวดเอว. ความดันโลหิตสูง, เวียนศีรษะ. CKD stage 1-2 → Asymptomatic !")
22
How to approach CKD Patients
Work up cause & Correction Slow progression of CKD Comorbidity treatment Counseling & Patient education Cost Mode of Renal replacement therapy : HD, CAPD, Kidney transplantation Nutrition Vascular access (in HD) Renal replacement therapy
 Renal replacement therapy.")
23
Causes of CKD DM : most common (~ 30-40 %)
Chronic glomerulonephritis (CGN) Vascular disease : HT Tubulointerstitial : Stones, NSAIDs, Gout Others : Polycystic kidney, etc.
 Vascular disease : HT. Tubulointerstitial : Stones, NSAIDs, Gout. Others : Polycystic kidney, etc.")
24
Initial investigation for CKD
U/A : proteinuria, sediment Proteinuria trace – repeat in 3-6 m. – repeat in 3-6 m. or urine protein-creatinine ratio (UPCR) > +2 – urine protein-creatinine ratio (UPCR) Abnormal : UPCR > 0.2 (or urine protein > 0.3 g/day) Serum creatinine, eGFR Plain KUB (or ultrasound) Others (depend on patient)
 > +2 – urine protein-creatinine ratio (UPCR) Abnormal : UPCR > 0.2 (or urine protein > 0.3 g/day) Serum creatinine, eGFR. Plain KUB (or ultrasound) Others (depend on patient)")
25
Slow Progression in CKD
Control BP ACEI, ARB Low Protein, Low Salt Diet Control Blood Sugar Control Lipid Level (?) Avoid Smoking Avoid Nephrotoxic Agents
 Avoid Smoking. Avoid Nephrotoxic Agents.")
26
Control BP Goal: ~ 130/80 – 140/90 mmHg Lifestyle modifications
Weight reduction: BMI 19-23 Diet: Low Salt Low Fat (saturated) Exercise (30 min. x 5 / week) Moderate Alcohol consumption (Beer 720 cc, Wine 300 cc, Whisky 90 cc)
 Exercise (30 min. x 5 / week) Moderate Alcohol consumption (Beer 720 cc, Wine 300 cc, Whisky 90 cc)")
27
Control BP Medication – ACEI, ARB
ACEI (Angiotensin Converting Enzyme Inhibitor): Enaril (Enalapril) Coversil (Perindopril) Tritace (Ramipril)
: Enaril (Enalapril) Coversil (Perindopril) Tritace (Ramipril)")
28
Control BP Medication ARB (Angiotensin II Receptor Blocker)
Cozaar (Losartan) Diovan (Valsartan) Micardis (Telmisartan) Aprovel (Irbesartan)
 Diovan (Valsartan) Micardis (Telmisartan) Aprovel (Irbesartan)")
29
Control BP Medication Ca2+-channel blocker Amlodipine
Adalat (Nifedipine) Madiplot (Manidipine) Zanidip (Lercanidipine) Isoptin (Verapamil) Herbesser (Diltiazem)
 Madiplot (Manidipine) Zanidip (Lercanidipine) Isoptin (Verapamil) Herbesser (Diltiazem)")
30
Control BP Medication Diuretics Beta-blocker Lasix (Furosemide)
HCTZ (Hydrochlorothiazide) Aldactone (Spironolactone) Beta-blocker Metoprolol Atenolol Propranolol
 Aldactone (Spironolactone) Beta-blocker. Metoprolol. Atenolol. Propranolol.")
31
Control BP Medication Alpha-blocker Centrally acting agent
Cardura, Pencor (Doxazosin) Minipress (Prazosin) Centrally acting agent Aldomet (Methyldopa) Direct vasodilator Apresoline (Hydralazine) Minoxidil
 Minipress (Prazosin) Centrally acting agent. Aldomet (Methyldopa) Direct vasodilator. Apresoline (Hydralazine) Minoxidil.")
32
RAAS (Renin-Angiotensin-Aldosterone System)
")
33
Diet Protein GFR < 30 ml/min/1.73 m2 (stage 3) 0.8 g/kg/day
CKD at risk of progression avoid high protein (1.3 g/kg/day) Salt < 2 g/day of Na+ (5 g of NaCl, เกลือแกง 1 ช้อนชา, น้ำปลา 2 ช้อนโต๊ะ)
 Salt. < 2 g/day of Na+ (5 g of NaCl, เกลือแกง 1 ช้อนชา, น้ำปลา 2 ช้อนโต๊ะ)")
34
Control Blood Sugar Goal Post-prandial: 80-160 mg/dl HbA1C: ~ 7 %
Fasting: mg/dl Post-prandial: mg/dl HbA1C: ~ 7 % Precaution of “Hypoglycemia”

35
Control Lipid Level Goal Triglyceride: < 200 mg/dl
Total Cholesterol: < 200 mg/dl Triglyceride: < 200 mg/dl HDL: > 45 mg/dl LDL: < 100 mg/dl

36
Nephrotoxic Agents NSAIDs : Diclofenac, Ibuprofen, Mefenamic acid (Ponstan), Indomethacin, Naproxen, etc. Aminoglycoside : Gentamicin, Amikin Herb medicine ACEI, ARB – stop, if Cr > 25% or Hyperkalemia

37
Treatment of CKD

38
Treatment Medication Anti-hypertensive Diuretics
Phosphate binder : CaCO3, Al(OH)3 Alkaline : NaHCO3 Rx of Anemia : EPO (erythropoietin), PRC transfusion, Ferrous Goal Hb g/dL (Hct 30-36%) Vitamin : Bco, C, Folic Others : DM, IHD, Dyslipidemia, Hyper K+
3. Alkaline : NaHCO3. Rx of Anemia : EPO (erythropoietin), PRC transfusion, Ferrous. Goal Hb g/dL (Hct 30-36%) Vitamin : Bco, C, Folic. Others : DM, IHD, Dyslipidemia, Hyper K+")
39
Treatment Diet Control Low Salt Low K+ Low Phosphate Low Fat
Low Protein Low Salt Low K+ Low Phosphate Low Fat Restricted Fluid Intake

40
Fat (ไขมัน) ควรกิน “Unsaturated fat (ไขมันไม่อิ่มตัว)” : น้ำมันถั่วเหลือง, น้ำมันรำข้าว, น้ำมันงา, น้ำมันมะกอก ไม่ควรกิน “Saturated fat (ไขมันอิ่มตัว)” : หมูสามชั้น, หนังสัตว์, เครื่องใน,ไข่แดง, น้ำมันหมู, น้ำมันปาล์ม, น้ำมันมะพร้าว, กะทิ, อาหารทะเล
 : หมูสามชั้น, หนังสัตว์, เครื่องใน,ไข่แดง, น้ำมันหมู, น้ำมันปาล์ม, น้ำมันมะพร้าว, กะทิ, อาหารทะเล.")
41
ผัก, ผลไม้ ประโยชน์ – วิตะมิน, ใยอาหาร หรือกากอาหาร (ไฟเบอร์) โทษ – โปแตสเซียม (Potassium, K+)
 โทษ – โปแตสเซียม (Potassium, K+)")
42
Potassium (K+) มาก ปานกลาง น้อย หัวปลี, หน่อไม้ฝรั่ง, โหระพา, หอมแดง,ผักกวางตุ้ง, มะเขือ, เห็ดฟาง, แครอท, ผักบุ้งไทย แตงกวา, ฟักเขียว, มะเขือยาว, มะละกอดิบ, พริกหยวก, เห็ดนางฟ้า, ผักบุ้งจีน บวบเหลี่ยม, ถั่วพู (ฝักอ่อน), หอมหัวใหญ่, เห็ดหูหนู ทุเรียน, ลำไย, กล้วย ส้ม, สับปะรด, ฝรั่ง, เงาะ, มะม่วง, องุ่น, ลิ้นจี่, ขนุน, มะละกอ แตงโม
, หอมหัวใหญ่, เห็ดหูหนู ทุเรียน, ลำไย, กล้วย. ส้ม, สับปะรด, ฝรั่ง, เงาะ, มะม่วง, องุ่น, ลิ้นจี่, ขนุน, มะละกอ. แตงโม.")
43
Phosphate (P) อาหารที่มี P สูง ถั่ว นม ไข่แดง น้ำอัดลม (โค้ก)
 อาหารที่มี P สูง ถั่ว นม ไข่แดง น้ำอัดลม (โค้ก)")
44
Water ปริมาณที่เหมาะสม/วัน = ปริมาณปัสสาวะ/วัน ml. Vitamin ไม่ควรกิน : A, E กินได้ : B, C, D

45
Treatment Correct Volume Status Dehydration: Volume overload:
Volume replacement Avoid diuretics Volume overload: Restrict fluid intake Diuretics Dialysis: HD, PD

46
Treatment Renal Replacement Therapy
Indications for Dialysis in CKD (ESRD) GFR ≤ 6 ml/min./1.73 m2 (Serum Cr ~ 10 mg/dl) Volume overload, Uncontrolled BP Hyper K+, Hyper P Uremic encephalopathy Uremic pericarditis, pleuritis Protein-Energy Malnutrition
 GFR ≤ 6 ml/min./1.73 m2. (Serum Cr ~ 10 mg/dl) Volume overload, Uncontrolled BP. Hyper K+, Hyper P. Uremic encephalopathy. Uremic pericarditis, pleuritis. Protein-Energy Malnutrition.")
47
Treatment Mode of Dialysis Hemodialysis (HD) : Intermittent
Continuous (CRRT, Continuous Renal Replacement Therapy) – CVVH(F), CAVH(F), CVVHD, CVVHDF, etc. Peritoneal Dialysis (PD) : Continuous – CAPD (Continuous Ambulatory PD), etc.
 – CVVH(F), CAVH(F), CVVHD, CVVHDF, etc. Peritoneal Dialysis (PD) : Continuous – CAPD (Continuous Ambulatory PD), etc.")
48
Convection

49
Hemodialysis Uremic toxins & Water Ultrafiltrate (UF) Diffusion M E B
Blood Dialysate Uremic toxins & Water Convection

50
Peritoneal Dialysis Uremic toxins & Water Ultrafiltrate (UF) Diffusion
B R A N Blood Peritoneal Cavity Uremic toxins & Water Dialysate

51
Daily Requirement in HD patients
Nutrition Daily Requirement in HD patients Energy 30–35 kcal/kg Protein 1.2 g/kg High biological value > 50% Na+ 3 g K+ Phosphate 1.2 g Water 500–1000 ml + Urine output อาหารโปรตีนที่มี essential amino acid ครบถ้วน ในสัดส่วนที่เหมาะสม ได้แก่ เนื้อสัตว์ ไข่ นม

52
Kidney Transplantation
Living-related KT Cadaveric KT

53
การฟอกเลือดด้วยเครื่องไตเทียม การฟอกเลือดทางช่องท้อง
การปลูกถ่ายไต ข้อดี 1. สามารถกำจัดน้ำที่เกินและของเสียได้อย่างรวดเร็ว และกำหนดปริมาณได้แน่นอน 2. ผู้ป่วยไม่ต้องเรียนรู้วิธีการทำ 1. ทำเองที่บ้านได้, ไม่ต้องเดินทางมาโรงพยาบาลบ่อยๆ 2. เหมาะสำหรับผู้ป่วยที่เป็นโรคหัวใจ และผู้ป่วยที่เป็นโรคเบาหวานมานาน 3. สภาพการทำงานของไตที่เหลืออยู่ดีกว่า 4. ต้องการการจำกัดอาหาร และน้ำน้อยกว่า 1. เป็นการรักษาที่ทำให้มีคุณภาพชีวิตดีที่สุด และคุ้มค่าที่สุด ข้อเสีย 1. ต้องใช้อุปกรณ์และบุคลากรมาก 2. ต้องเดินทางมาทำในโรงพยาบาล สัปดาห์ละ 2-3 ครั้ง 3. อาจเกิดภาวะแทรกซ้อนขณะทำ เช่น ความดันโลหิตต่ำ ปวดศีรษะ ตะคริว ฯลฯ 1. มีโอกาสติดเชื้อทางช่องท้อง 2. อาจรู้สึกแน่นอึดอัดเมื่อน้ำอยู่ในท้อง 1. ต้องกินยากดภูมิคุ้มกัน จึงมีโอกาสเสี่ยงต่อการติดเชื้อได้ง่าย 2. ผู้บริจาคไตหาได้ยาก

54
ผู้ป่วยไตวายเรื้อรังระยะสุดท้าย (ESRD)
ข้อห้ามในการทำ CAPD มี ไม่มี CAPD ทำ CAPD ต่อไม่ได้ ใช่ ไม่ใช่ HD CAPD KT

55
Pitfall ผู้ป่วย CKD ไม่จำเป็นต้องมีปัสสาวะน้อย ดังนั้น ไม่จำเป็นต้องได้ Diuretics ทุกราย ผู้ป่วย CKD ที่ยังไม่ได้เริ่มทำ HD จำกัดโปรตีน ผู้ป่วยที่ทำ HD แล้ว กินโปรตีนให้เต็มที่

56
โรคไตเรื้อรังระยะสุดท้าย
คนปกติ โรคไตเรื้อรัง โรคไตเรื้อรังระยะสุดท้าย ป้องกัน ชะลอการเสื่อม

57
ทำอย่างไร ไตไม่วาย ตรวจร่างกายเป็นประจำทุกปี วัดความดันโลหิต
ตรวจปัสสาวะ ตรวจเลือด – ดูระดับ BUN, Cr ดูแลรักษาสุขภาพ กินอาหารที่เป็นประโยชน์ พักผ่อนให้เพียงพอ : นอนหลับวันละ 6 – 8 ชม. ดื่มน้ำสะอาดให้เพียงพอ : วันละ 6 – 8 แก้ว

58
ทำอย่างไร ไตไม่วาย ดูแลรักษาสุขภาพ (ต่อ)
ออกกำลังกาย : อย่างน้อย 30 นาที, 5 ครั้ง/สัปดาห์ ควบคุมน้ำหนักตัว ดัชนีมวลกาย (Body Mass Index, BMI) = น้ำหนัก (กก.) / ส่วนสูง (เมตร) 2 ถ้ามากกว่า 23 ถือว่า “อ้วน” อย่ากลั้นปัสสาวะ อย่าปล่อยให้ท้องเสียนานเกินไป
 = น้ำหนัก (กก.) / ส่วนสูง (เมตร) 2. ถ้ามากกว่า 23 ถือว่า อ้วน อย่ากลั้นปัสสาวะ. อย่าปล่อยให้ท้องเสียนานเกินไป.")
59
ทำอย่างไร ไตไม่วาย หลีกเลี่ยงปัจจัยเสี่ยงต่อโรคไตเรื้อรัง
เลิกสูบบุหรี่ – มีสารพิษ > 50 ชนิด ! ลดความอ้วน ฯลฯ ระมัดระวังเรื่องการใช้ยา ยาแก้ปวด กลุ่ม “เอ็นเสด (NSAIDs)” อาหารเสริม, สมุนไพร บางชนิด
 อาหารเสริม, สมุนไพร บางชนิด.")
60
ทำอย่างไร ไตไม่วาย ถ้ามีอาการผิดปกติ รีบไปพบแพทย์ ปัสสาวะขัด
ปัสสาวะบ่อยตอนกลางคืน ปัสสาวะมีสีแดง หน้าบวม เท้าบวม ปวดหลัง ปวดเอว

61
Continuous Ambulatory Peritoneal Dialysis
(CAPD) นพ.พันธพงศ์ ตาเรืองศรี พบ., วว.อายุรศาสตร์, วว.อายุรศาสตร์โรคไต
 นพ.พันธพงศ์ ตาเรืองศรี พบ., วว.อายุรศาสตร์, วว.อายุรศาสตร์โรคไต.")
62
Continuous Ambulatory Peritoneal Dialysis (CAPD)
")
63
Peritoneal Dialysis Uremic toxins & Water Ultrafiltrate (UF) Diffusion
B R A N Blood Peritoneal Cavity Uremic toxins & Water Dialysate

64
Mode of PD Manual / Automated Continuous
Continuous Ambulatory PD (CAPD) Continuous Cyclic PD Intermittent Day-time Ambulatory PD Nightly Intermittent PD Manual / Automated หลักการ Prescription Complication
 Continuous Cyclic PD. Intermittent. Day-time Ambulatory PD. Nightly Intermittent PD. Manual / Automated. หลักการ. Prescription. Complication.")
65
Mode of PD Auto mated PD

66
PD Prescription Mode: CAPD Peritoneal Dialysate Fluid Adequacy
1.5%, 2.5%, 4.25% Dextrose 2 Litre / bag 4 - 6 cycles / day Adequacy Weekly Kt/V > 1.7 Weekly nCCr > 50 Litre / 1.73 m2

67
Complications Infection Volume overload Catheter malfunction
Metabolic: HypoK+, Hyperglycemia Anemia Cardiovascular Malnutrition Inadequacy

68
Complications Infection Exit site infection & Tunnel infection
- common cause: staph. aureus - Empirical Rx of exit site infection : Dicloxacillin, oral, 14 d

69
Complications Infection Exit site infection & Tunnel infection
- common cause: staph. aureus - Empirical Rx of exit site infection : Dicloxacillin, oral, 14 d Acute Exit Site Infection

70
Complications Infection Exit site infection & Tunnel infection
- common cause: staph. aureus - Empirical Rx of exit site infection : Dicloxacillin, oral, 14 d Chronic Exit Site Infection

71
Equivocal Exit Site Infection
Exit site infection & Tunnel infection - common cause: staph. aureus - Empirical Rx of exit site infection : Dicloxacillin, oral, 14 d Chronic Exit Site Infection Equivocal Exit Site Infection

72
Tunnel Infection

73
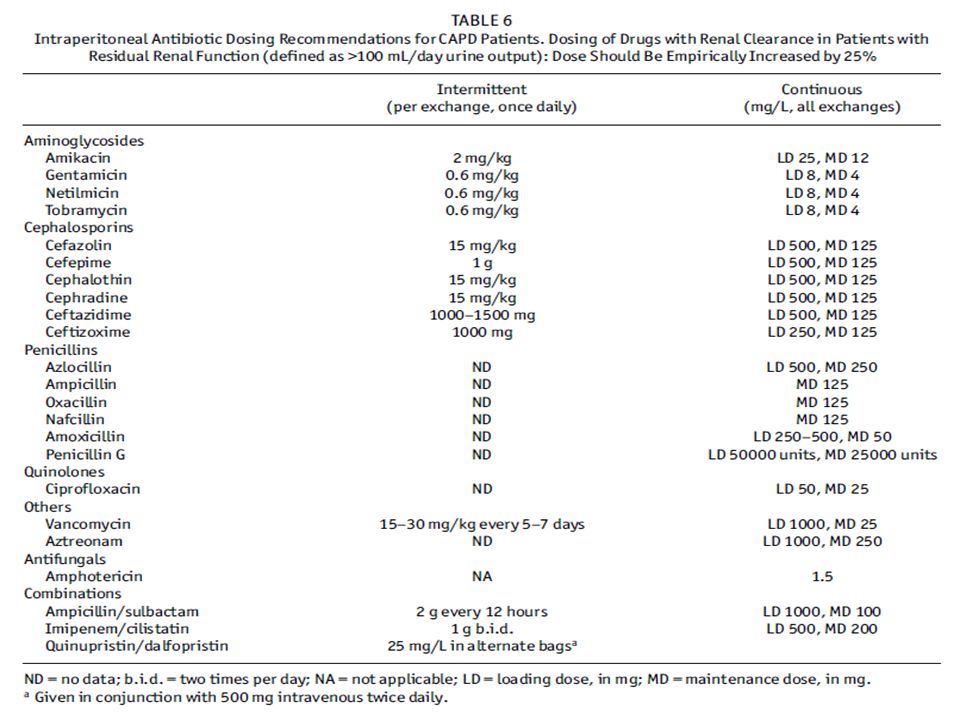
Complications Infection Peritonitis or specific Rx 14 d
- common cause: staph. epidermidis - PDF WBC > 100 /mL, > 50% PMNs - PDF 10 ml in hemoculture media: yield - Empirical Rx: Cefazolin 1 gm, IP, od Ceftazidime 1 gm, IP, od or specific Rx 14 d

75
Complications Infection Peritonitis
- Heparin, 500 u/L, prevent occlusion of the catheter by fibrin - Indications for Catheter Removal: Refractory peritonitis Relapsing peritonitis Refractory exit-site and tunnel infection Fungal peritonitis

76
Infection Peritonitis
Complications Infection Peritonitis < 4 weeks > 4 weeks Same organism Relapsing Repeat New organism Recurrent Refractory : failure of the effluent to clear after 5 days of appropriate ABO

77
Infection Peritonitis
Complications Infection Peritonitis < 4 weeks > 4 weeks Same organism Relapsing Repeat New organism Recurrent Refractory : failure of the effluent to clear after 5 days of appropriate ABO

78
Complications Volume overload Edema False UF Failure True UF Failure
I/O, Salt & Water & Diet Compliance Residual renal function False UF Failure True UF Failure PET study High Low High Av/Low Av Catheter malfunction - Leakage Peritonitis - Large vascular area Adhesion - SEP Aquaporin def. - Lymphatic absorption

79
Complications Infection Catheter malfunction Volume overload
Metabolic: HypoK+, Hyperglycemia Anemia Cardiovascular Malnutrition Inadequacy

80
ขอบคุณครับ สงสัยอะไร เชิญถามได้ครับ

งานนำเสนอที่คล้ายกัน










.>")




 สับปะรด แตงโม.>")



