ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Advisor อาจารย์ นพ.ธเนศ แก่นสาร

2
หญิงไทย อายุ 24 ปี อาชีพ เจ้าหน้าที่ห้องบัตร โรงพยาบาลเอกชน ภูมิลำเนา จังหวัดมุกดาหาร ที่อยู่ปัจจุบัน จังหวัดสมุทรปราการ (หอพักโรงพยาบาล)
 .")
4
5 ปี PTA ทำงานบริษัท เริ่มคบกับแฟนคนแรก ( ) ทำงานที่เดียวกัน มีเพศสัมพันธ์กันสม่ำเสมอ ไม่เจ็บเวลามีเพศสัมพันธ์ มีปวดท้องน้อยนานๆ ครั้งหลังมีเพศสัมพันธ์ แต่ไม่ทุกครั้ง เคยตรวจที่ รพ.เอกชน ด้วยเรื่องตกขาว วินิจฉัยเป็นมดลูกอักเสบ ได้ยากินอาการดีขึ้น
 ทำงานที่เดียวกัน มีเพศสัมพันธ์กันสม่ำเสมอ ไม่เจ็บเวลามีเพศสัมพันธ์ มีปวดท้องน้อยนานๆ ครั้งหลังมีเพศสัมพันธ์ แต่ไม่ทุกครั้ง เคยตรวจที่ รพ.เอกชน ด้วยเรื่องตกขาว วินิจฉัยเป็นมดลูกอักเสบ ได้ยากินอาการดีขึ้น.")
5
2 ปี PTA ย้ายที่ทำงานมาอยู่ที่โรงพยาบาลเอกชน ทำงานเป็นเจ้าหน้าที่ห้องบัตรตั้งแต่เวลา น. ลักษณะงานเป็นงานเอกสารและคอมพิวเตอร์สลับตำแหน่งกันภายในแผนก ไม่มีปัญหากับผู้ร่วมงาน รู้สึกสนุกกับงานที่ทำ

6
9 เดือน PTA เริ่มปวดท้องน้อยตรงกลางท้องบ่อยขึ้น ปวดบีบเป็นพักๆ ปวดทุกวันช่วงเวลา น. ยังทำงานได้ วันที่ปวดมากมักร้าวขึ้นลิ้นปี่ และมีปัสสาวะบ่อยร่วมด้วย ไม่มีปัสสาวะแสบขัด ไม่มีเลือดปน ไม่มีนิ่ว ไม่มีตกขาว อาการปวดท้องไม่สัมพันธ์กับการกินอาหารหรือเหตุการณ์ที่ทำงาน หลังเข้านอนไม่เป็น ไม่มี night pain นอนหลับได้ปกติ

7
9 เดือน PTA ถ่ายอุจจาระ 2 วัน/ครั้ง ค่อนข้างแข็ง ไม่แสบก้น ไม่มีถ่ายเป็นเลือด ไม่มี bowel habit change ประจำเดือนสมาสม่ำเสมอทุก วัน มาครั้งละ 3-5 วัน LMP 5/7/55 ไม่เคยปวดประจำเดือน ไม่ได้ถามประวัติคุมกำเนิด

8
9 เดือน PTA (ต่อ) รักษาที่รพ.เอกชนที่ทำงานอยู่ ได้รับการตรวจร่างกาย ตรวจภายใน UA, TAS 2 ครั้งโดยสูติ-นรีแพทย์, work up R/O KUB stone โดยศัลยแพทย์หลายครั้ง ไม่พบความผิดปกติ วินิจฉัยเป็น pelvic pain, dysuria, dyspepsia เคยได้รับการรักษาเป็น NSAIDs, Hyoscine, Omeprazole หลายครั้งอาการไม่ดีขึ้น

9
9 เดือน PTA (ต่อ) เริ่มรู้จักแฟนคนปัจจุบัน เป็นช่างเขียนแบบ โสด ทำงานคนละที่ เจอกัน 1-2 ครั้ง/สัปดาห์ ทุกครั้งที่เจอกันที่บ้านของแฟน ค้างคืนด้วยกัน แต่เพิ่งเริ่มมีเพศสัมพันธ์กันเมื่อ 1-2 เดือน PTA ไม่เจ็บ แต่ก็ไม่ถึงจุด ...

10
Traumatic head injury S/P Sx
(59) Traumatic head injury S/P Sx ช่วยเหลือตนเองได้ (55) (27) เขียนแบบ 1st relation เลิกปี 2553 2nd relation เริ่มปลายปี 2554 Room mate เจ้าหน้าที่ห้องบัตร
 Traumatic head injury S/P Sx. ช่วยเหลือตนเองได้ (55) (27) เขียนแบบ. 1st relation. เลิกปี nd relation. เริ่มปลายปี Room mate. เจ้าหน้าที่ห้องบัตร.")
11
ปฏิเสธการแพ้ยา ปฏิเสธการแพ้อาหาร
ปฏิเสธโรคประจำตัว ไม่เคยผ่าตัด ไม่ได้ใช้ยาใดเป็นประจำ นอกจากที่ได้จากโรงพยาบาล

12
อาจจะปวดจากทำงาน + เดินมาก ไม่น่าจะเกี่ยวกับเรื่องเพศสัมพันธ์
Idea กลัวมีก้อนที่มดลูก กลัวเป็นโรครุนแรง Feeling ปกติ Function อยากรู้ว่าเป็นอะไรแน่ อยากหาย Expectation

13
A 24-years-old woman with

15
Vital signs BP 100/70 mmHg, BT ไม่ได้วัด PR 80/min, RR 20/min GA A young female, active HEENT No pale conjunctiva, no icteric sclera, no lymphadenopathy CVS Normal S1 and S2, no murmur RS Clear breath sound, no adventitious sound

16
No distension, normal bowel sound, soft, not tender, no palpable mass
Abdomen No distension, normal bowel sound, soft, not tender, no palpable mass Genitalia PV - not test Previous exam at private hospital : unremarkable Extremities No edema, not seen rash or skin lesion Skin Not seen skin lesion or evidence of trauma

19
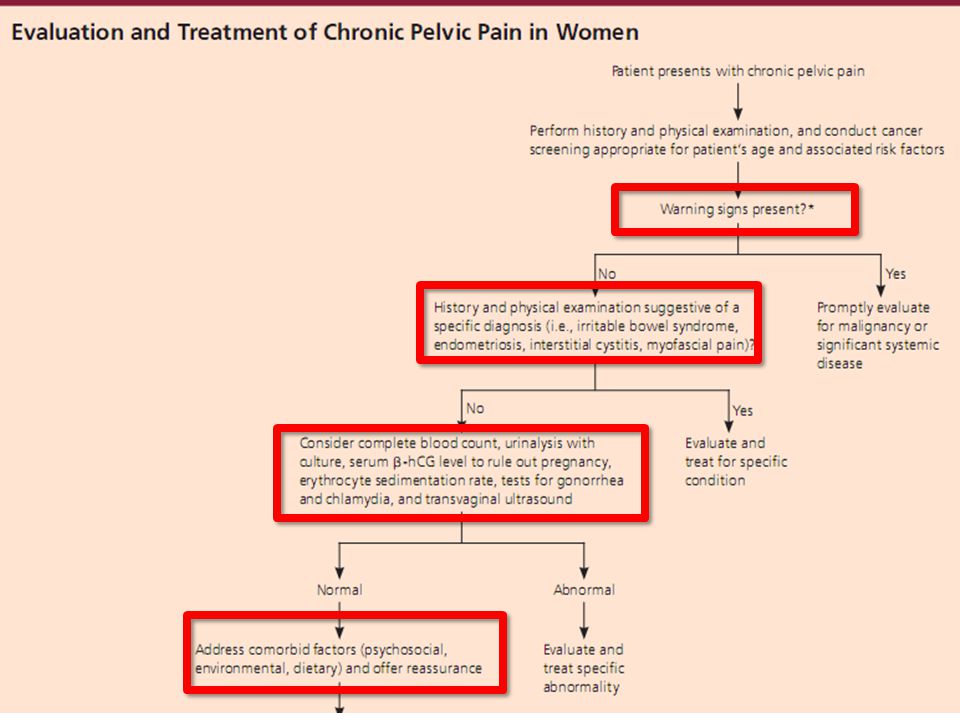
ACOG Committee on Practice Bulletins. ACOG Practice Bulletin No. 51
ACOG Committee on Practice Bulletins. ACOG Practice Bulletin No. 51. Chronic pelvic pain. Obstet Gynecol 2004; 103:589–605. Chronic pelvic pain Cyclic (or noncyclic) pain that lasts longer than 6 month Localized to pelvis, anterior abdominal wall, below umbilicus or buttocks Sufficient severity to cause functional disability or required medical care
 pain that lasts longer than 6 month. Localized to pelvis, anterior abdominal wall, below umbilicus or buttocks. Sufficient severity to cause functional disability or required medical care.")
20
Nociceptive pain Non-nociceptive pain Estrogen Depression
Personality disorder Nociceptive pain Somatic (sharp pain) Visceral (dull pain) Non-nociceptive pain Neuropatic pain Psychogenic pain Allodynia Hyperalgesia
 Visceral (dull pain) Non-nociceptive pain. Neuropatic pain. Psychogenic pain. Allodynia. Hyperalgesia.")
21
A. B. C. D. Endometriosis Bowel dysmotility Depressive disorder
Physical and sexual abuse B. Gynecologic problems C. Non gynecologic medical problems D. Psychological problems Endometriosis Pelvic adhesions Dysmenorrhea and Mittelschmerz Chronic PID Bowel dysmotility Musculoskeletal dysfunction Depressive disorder Somatoform disorders

22
Gynecology Urologic Musculoskeletal Gastrointestinal Psychological
Endometriosis Interstitial cystitis Pelvic adhesions Chronic UTI Pelvic varicosities Urethral syndrome Pelvic inflammatory disease Urinary calculi Adeomyosis Radiation cystitis Vulvodynia Musculoskeletal Uterine myomas Myofascial pain (abdominal wall or pelvic floor muscles) Ovarian cyst, ovarian tumor Coccygeal or low back pain Tuberculous salpingitis Nerve pain Gastrointestinal Psychological Irritable bowel syndrome Childhood physical or sexual abuse Inflammatory bowel disease Emotional abuse Chronic constipation Partner violence Colitis Malignancies Diverticulitis Bladder Post operative Gynecologic Adhesions Colon Previous tubal ligation
 Ovarian cyst, ovarian tumor. Coccygeal or low back pain. Tuberculous salpingitis. Nerve pain. Gastrointestinal. Psychological. Irritable bowel syndrome. Childhood physical or sexual abuse. Inflammatory bowel disease. Emotional abuse. Chronic constipation. Partner violence. Colitis. Malignancies. Diverticulitis. Bladder. Post operative. Gynecologic. Adhesions. Colon. Previous tubal ligation.")
23
20-25 % of CCP (controversial role of pain)
Cause Acute or chronic inflammatory disorder Physico-chemical trauma (surgery)
")
24
30% of CPP (12% in combination with another pelvic pathology)
Pelvic congestion syndrome (PCS) Ovarian and pelvic (internal illiac) varicies Venous incompetence, reduced venous clearance in pelvis/ reflux Unknown pathophysiology
 Ovarian and pelvic (internal illiac) varicies. Venous incompetence, reduced venous clearance in pelvis/ reflux. Unknown pathophysiology.")
25
Unknown caused Lt > Rt
Chronic pelvic, suprapubic, perineal, vulvo-vaginal pain, pressure with urinary urgency, diurnal frequency, nocturia Unknown caused Lt > Rt Exacerbation of pain : during or after sexual intercourse 10-15% overactive bladder Co-existing with endometriosis

26
Functional dysmotility disorder of the bowel 65-79% of woman with CPP
Uncertain etiology and multifactor pathophysiology Altered bowel motility Visceral hypersensitivity Psychosocial factor

27
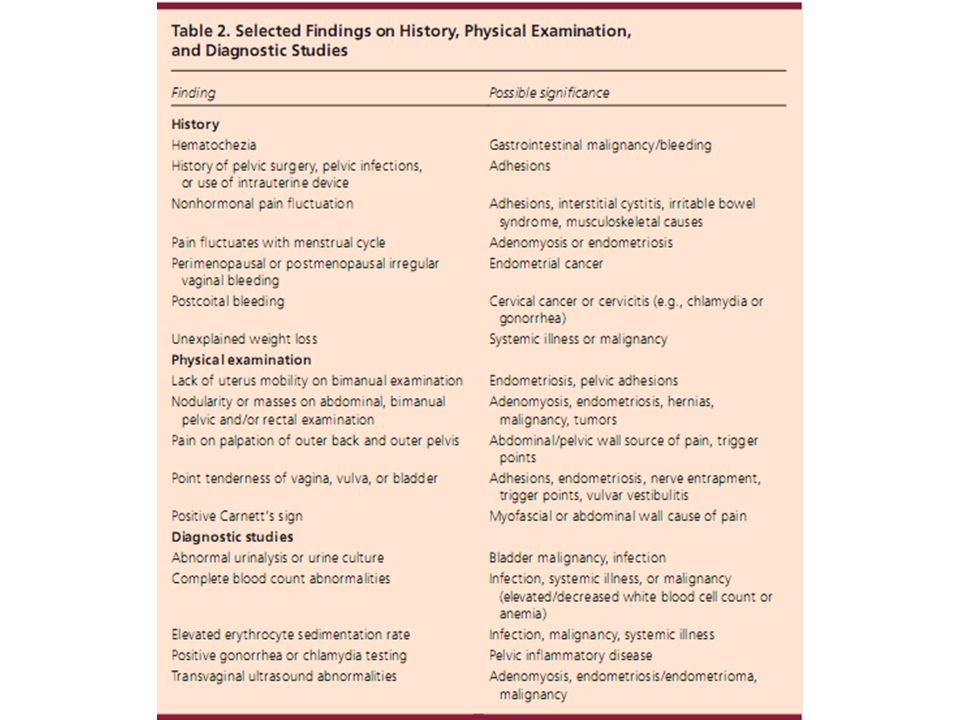
History Pattern of the pain Associated symptom and red flag sign Previous surgery, child delivery Menstrual and contraception Life situation, abuse Patient’s affect

28
Physical Examination General exam PV and focus on bladder and urethra Bimanual or rectovaginal examination Piriformis muscle Abdominal deformity “Carnett’s sign” Back and inguinal area

29
Investigation Cervical cytology Endocervical cultures UA, urine culture Stool occult blood Pelvic ultrasound Laparoscopy Cystoscope Sigmoidoscopy/Colonoscopy +/- cancer screening, beta hCG

31
Multimodal A strong physician-patient relationship Analgesics
Acetamonophen NSAIDs Opioid analgesics Vitamin B1, Magnesium sulfate tablet Anticonvulsants : gabapentin, topiramate, valproic acid, pregabalin Botulinum toxin (Botox) injections
 injections.")
32
Hormonal treatment

33
Antidepressants : TCA, SSRI
Lysis adhesion Hysterectomy Uterosacral nerve ablation

36
CPP has similar to the prevalence of migraine, asthma and low back pain (in UK)
4 most common causes of CPP are (endometriosis) pelvic adhesions, pelvic varicies, interstitial cystitis, and irritable bowel syndrome. Women with CPP have more than one cause for their pain.
 pelvic adhesions, pelvic varicies, interstitial cystitis, and irritable bowel syndrome. Women with CPP have more than one cause for their pain.")
38
Unclear what to do with the answers
Unfamiliarity with treatment approaches Uncertainty about the next question Fear to offending patient Lack of obvious justification Generational obstacles Fear of sexual misconduct charge Sometimes perceived irrelevant Unfamiliarity with some sexual practices

39
Morbidity and motality – STDs and HIV/AIDS
Symptoms of illness Treatment side effects Past may explain present problems Function potentially lifelong Dysfunctions and difficulties are common Association with health and happiness Why not? May be negligent if ignored

40
Ask patient PERMISSION
Interviewer takes INITIATIVE LANGUAGE MEDICAL/TECHNICAL VS slang STATEMENT/QUESTION TECHNIQUE PRIVACY/CONFIDENTIALITY/SECURITY DELAY SENSITIVE QUESTIONS Display NONJUDGEMENTAL attitude Provide EXPLANATION Discuss FEELINGS Promote OPTIMISTIC ATTITUDE

งานนำเสนอที่คล้ายกัน














>")







