ดาวน์โหลดงานนำเสนอ
1
Mechanical Ventilation & Clinical application
กวีวรรณ ลิ้มประยูร หน่วยหออภิบาลผู้ป่วยเด็ก หน่วยโรคระบบทางเดินหายใจ ภาควิชากุมารเวชศสตร์ คณะแพทยศาสตร์ศิริราชพยาบาล

7
Indication

8
Indication Respiratory failure
To decrease or support work of breathing To improve oxygenation To recruit the lung To support other organs e.g.: increased ICP, CHF

9
Normal value Tidal volume 10-12 ml/kg in general or 6-8 ml/kg in ARDS
MV ml /kg

10
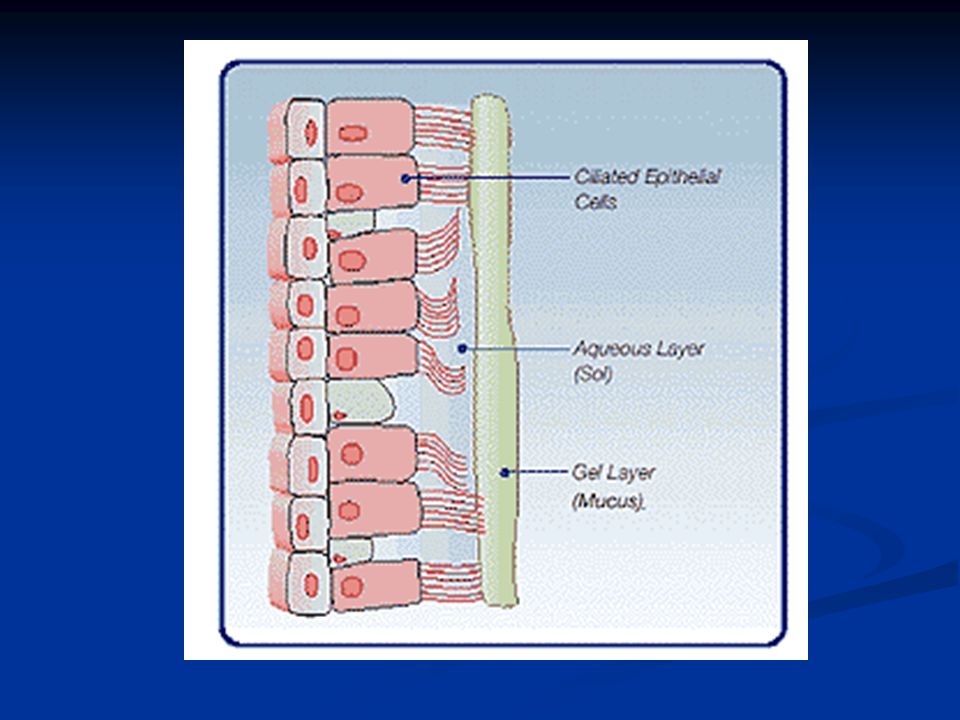
Parts and Humidifiers

17
How to set in some situations
post-operative asthma or BPD pneumonia or ARDS increased ICP

18
Initial Settings FiO (100% O 2 ) for a patient with lung disease; 0.40 (40% O2 ) for a patient without lung disease. PEEP +6-8 for a patient with lung disease; +4 for a patient without lung disease. RR 30 for infants up to 1 year of age; 20 for those 1-6 years of age and 15 for those greater than 6 (which are the average normal respiratory rates for age). I Time Based upon an I:E ratio of 1:2 for infants and pre-school age children and 1:2.5 for schoolage and adolescents. Therefore, 0.7 sec for infants up to 1 year of age; 1 sec for those to 6 years of age and 1.2 secs for those greater than 6. Tidal Volume 10 cc/kg (Range 8-12 cc/kg). Just a “few” years ago, many patients were started on 15 cc/kg, the volume that seemed to work “best” to prevent atelectasis in adult post-op patients ie those with normal lungs. However, with barotrauma (air leaks)
. I Time Based upon an I:E ratio of 1:2 for infants and pre-school age children and 1:2.5 for schoolage and adolescents. Therefore, 0.7 sec for infants up to 1 year of age; 1 sec for those to 6 years of age and 1.2 secs for those greater than 6. Tidal Volume 10 cc/kg (Range 8-12 cc/kg). Just a few years ago, many patients were started on 15 cc/kg, the volume that seemed to work best to prevent atelectasis in adult post-op patients ie those with normal lungs. However, with barotrauma (air leaks)")
19
Guidelineในการตั้งเครื่องช่วยหายใจเบื้องต้น (12)
1.เลือก mode ของเครื่องช่วยหายใจที่คุ้นเคยมากที่สุด โดยจุดประสงค์ของการช่วยหายใจคือให้การช่วยหายใจเพื่อทำให้มีการแลกเปลี่ยนกาซที่เพียงพอ (adequate oxygenation/ventilation) ลดงานซึ่งเกิดจากการหายใจ (reduced work of breathing) หายใจมีปฏิสัมพันธ์กับเครื่องช่วยหายใจ (synchrony between patient and ventilator) (12,17) หลีกเลี่ยงการใช้ความดันขนาดสูง (avoidance of high end-inspiration pressures) 2.ควรตั้งปริมาณความเข้มข้นออกซิเจนขนาดสูงก่อน อาจตั้งโดยใช้ออกซิเจน FiO2 1.0 ก่อนแล้วค่อยๆลดขนาดลงเพื่อพยายามคงค่าความอิ่มตัวออกซิเจนในเลือด (oxygen saturation,SaO2) ให้ได้ประมาณ92-95% ในรายที่มีความผิดปกติของปอดรุนแรง เช่นภาวะ Adult Respiratory Distress Syndrome (ARDS) อาจยอมรับที่ค่าค่าความอิ่มตัวออกซิเจนในเลือดมากกว่าหรือเท่ากับ 88% (12,18)
 ลดงานซึ่งเกิดจากการหายใจ (reduced work of breathing) หายใจมีปฏิสัมพันธ์กับเครื่องช่วยหายใจ (synchrony between patient and ventilator) (12,17) หลีกเลี่ยงการใช้ความดันขนาดสูง (avoidance of high end-inspiration pressures) 2.ควรตั้งปริมาณความเข้มข้นออกซิเจนขนาดสูงก่อน อาจตั้งโดยใช้ออกซิเจน FiO2 1.0 ก่อนแล้วค่อยๆลดขนาดลงเพื่อพยายามคงค่าความอิ่มตัวออกซิเจนในเลือด (oxygen saturation,SaO2) ให้ได้ประมาณ92-95% ในรายที่มีความผิดปกติของปอดรุนแรง เช่นภาวะ Adult Respiratory Distress Syndrome (ARDS) อาจยอมรับที่ค่าค่าความอิ่มตัวออกซิเจนในเลือดมากกว่าหรือเท่ากับ 88% (12,18)")
20
3.เริ่มต้นควรตั้งปริมาตร tidal volume ประมาณ 8-10 ml ต่อน้ำหนักตัว 1 กิโลกรัมในกรณีทั่วไป หรืออาจเริ่มตั้งในขนาด ml ต่อน้ำหนักตัว 1 กิโลกรัมในผู้ป่วย neuromuscular disease เพื่อให้การหายใจได้ตามเครื่อง ในรายที่มีความผิดปกติของปอดรุนแรง เช่นภาวะ Adult Respiratory Distress Syndrome (ARDS) อาจเริ่มตั้งที่ขนาด 5-8 ml ต่อน้ำหนักตัว 1 กิโลกรัมและความดันช่วง plateau pressure น้อยกว่า 30 มม.น้ำ 4.เลือกอัตราการหายใจที่เหมาะสมเพื่อให้ได้การหายใจต่อนาทีที่เหมาะสมกับโรคและลักษณะทางคลีนิก โดยปรับผลตามค่าก๊าซในเลือด (17)
")
21
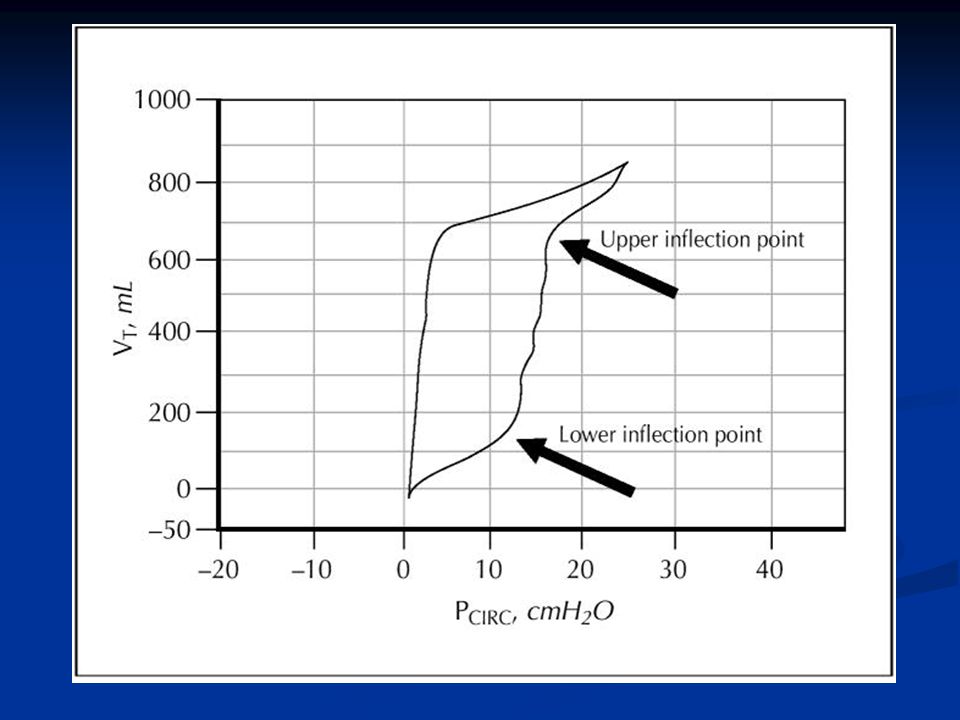
5.พยายามปรับใช้ PEEP ในในรายที่มีความผิดปกติของปอดรุนแรงทั่วไป (diffuse lung injury) เพื่อพยายามทำให้การใช้ออกซิเจนลดลง และพยายามหาค่า PEEP ที่เหมาะสม ส่วนใหญ่อยู่ที่ประมาณ มม.น้ำโดย อาจอาศัยดูค่า pressuse-volume curves หรือการเปลี่ยนแปลงของ ปริมาตร tidal volume ค่าก๊าซในเลือด หรือภาพเอกซ์เรย์ปอดเพื่อดู overinflation และควรติดตามผลที่ไม่พึงประสงค์จาก PEEP (5)เช่น barotrauma ความดันเลือดต่ำ หรือการแลกเปลี่ยนก๊าซแย่ลงในกรณี overinflation 6.ตั้งค่าความไวของ trigger ที่เหมาะสมโดยพยายามให้มีปฏิสัมพันธ์ระหว่างผู้ป่วยกับเครื่องช่วยหายใจมากที่สุดโดยที่ ไม่ตั้งต่ำเกินไปจนกระทั่งเกิดเครื่องช่วยหายใจทำงานเอง (autocycling) 7. ควรระมัดระวังในการใช้อัตราส่วนของระยะเวลาหายใจออกที่เหมาะสม ในผู้ป่วยซึ่งมีความเสี่ยงต่อการเกิด air trapping เนื่องจากการเกิด autoPEEP ที่ไม่ต้องการได้
 7. ควรระมัดระวังในการใช้อัตราส่วนของระยะเวลาหายใจออกที่เหมาะสม ในผู้ป่วยซึ่งมีความเสี่ยงต่อการเกิด air trapping เนื่องจากการเกิด autoPEEP ที่ไม่ต้องการได้")
22
8.ในกรณีซึ่งผู้ป่วยมีการแลกเปลี่ยนกาซที่ไม่ดีและต้องการเครื่องช่วยหายใจขนาดสูงควรคำนึงถึงการใช้ยานอนหลับขนาดสูงและหรือยาคลายกล้ามเนื้อร่วมด้วย 9.ควรปรึกษาหรือพิจารณาส่งต่อในกรณีที่เกินขีดความสามารถในการดูแลหรือปรับเปลี่ยนไปในสถานที่ซึ่งมีความชำนาญหรือมีศักยภาพในการดูแลผู้ป่วย หรือเพื่อการช่วยหายใจแบบ Non-conventional mechanical ventilation

23
Example 1- post operative
Mode: Pressure controlled ventilation PIP cm H2O PEEP cm H2O FiO i Time sec Rate / min

24
Example 2- asthma Mode: Time cycled pressure limited
Flow times minute ventilation (Normal MV = ml/kg) PIP cm H2O PEEP cm H2O FiO i Time sec Rate / min
 PIP 20 cm H2O. PEEP 3 cm H2O. FiO i Time 0.6 sec. Rate 20 / min.")
25
Mode ข้อดี/ข้อได้เปรียบ Assist-control ventilation (AC)
ผู้ป่วยสามารถได้รับความช่วยเหลือเพิ่มมากขึ้นเมื่อผู้ป่วยมีอัตราการหายใจเพิ่มขึ้น , ลดงานของการหายใจ (work of breathing) เมื่อเปรียบเทียบกับการหายใจเองอย่างเดียว (spontaneous breathing) AC volume ventilation รับรองปริมาตรของ tidal volume แม้มีพยาธิสภาพปอดซึ่งเกิดจากความยืดหยุ่นหรือความเสียดทานเปลี่ยนแปลง AC pressure-control ventilation จำกัดค่าความดันสูงสุด ,ลดภยันตรายจากความดันสูงต่อปอด Pressure support ventilation (PSV) หายใจผ่านเครื่องโดยมีปฏิสัมพันธ์ระหว่างผู้ป่วยและเครื่องช่วยหายใจมากขึ้น และลดงานของการหายใจ (work of breathing) Synchronized intermittent mandatory ventilation (SIMV) มีการรบกวนต่อการทำงานของหัวใจและหลอดเลือดน้อย Controlled mechanical ventilation (CMV) กล้ามเนื้อหายใจได้พัก
 เมื่อเปรียบเทียบกับการหายใจเองอย่างเดียว (spontaneous breathing) AC volume ventilation. รับรองปริมาตรของ tidal volume แม้มีพยาธิสภาพปอดซึ่งเกิดจากความยืดหยุ่นหรือความเสียดทานเปลี่ยนแปลง. AC pressure-control ventilation. จำกัดค่าความดันสูงสุด ,ลดภยันตรายจากความดันสูงต่อปอด. Pressure support ventilation (PSV) หายใจผ่านเครื่องโดยมีปฏิสัมพันธ์ระหว่างผู้ป่วยและเครื่องช่วยหายใจมากขึ้น และลดงานของการหายใจ (work of breathing) Synchronized intermittent mandatory ventilation (SIMV) มีการรบกวนต่อการทำงานของหัวใจและหลอดเลือดน้อย. Controlled mechanical ventilation (CMV) กล้ามเนื้อหายใจได้พัก.")
26
Mode ข้อเสีย/ข้อจำกัด Assist-control ventilation (AC)
มีแนวโน้มอาจจะมีผลต่อการทำงานของหัวใจและหลอดเลือด, อาจทำให้เกิดการช่วยหายใจเกินความต้องการ (inappropriate hyperventilation) AC volume ventilation อาจเกิดภยันตรายต่อปอดจากความดันสูงเกิน AC pressure-control ventilation อาจเกิดการช่วยหายใจไม่เพียงพอหรือมากเกินในกรณีค่าความยืดหยุ่นและค่าความเสียดทานของปอดมีการเปลี่ยนแปลง Pressure support ventilation (PSV) สัญญาณเตือนเมือผู้ป่วยหยุดหายใจเป็นเพียงสัญญาณเตือนเมื่อผู้ป่วยหายใจได้ไม่เพียงพอหรือหยุดหายใจ โดยไม่มีการช่วยเมื่อผู้ป่วยหยุดหายใจ, การตอบสนองต่อการช่วยหายใจขึ้นกับปัจจัยในการหายใจเองของผู้ป่วยด้วย Synchronized intermittent mandatory ventilation (SIMV) งานของการหายใจ (work of breathing) มากกว่าเมื่อเปรียบเทียบกับการช่วยหายใจแบบ assist-control Controlled mechanical ventilation (CMV) ต้องการ ยานอนหลับและ/หรือยาคลายกล้ามเนื้อ, อาจจะมีผลต่อการทำงานของหัวใจและหลอดเลือด
 AC volume ventilation. อาจเกิดภยันตรายต่อปอดจากความดันสูงเกิน. AC pressure-control ventilation. อาจเกิดการช่วยหายใจไม่เพียงพอหรือมากเกินในกรณีค่าความยืดหยุ่นและค่าความเสียดทานของปอดมีการเปลี่ยนแปลง. Pressure support ventilation (PSV) สัญญาณเตือนเมือผู้ป่วยหยุดหายใจเป็นเพียงสัญญาณเตือนเมื่อผู้ป่วยหายใจได้ไม่เพียงพอหรือหยุดหายใจ โดยไม่มีการช่วยเมื่อผู้ป่วยหยุดหายใจ, การตอบสนองต่อการช่วยหายใจขึ้นกับปัจจัยในการหายใจเองของผู้ป่วยด้วย. Synchronized intermittent mandatory ventilation (SIMV) งานของการหายใจ (work of breathing) มากกว่าเมื่อเปรียบเทียบกับการช่วยหายใจแบบ assist-control. Controlled mechanical ventilation (CMV) ต้องการ ยานอนหลับและ/หรือยาคลายกล้ามเนื้อ, อาจจะมีผลต่อการทำงานของหัวใจและหลอดเลือด.")
27
Alarms

28
Alarms Usually will set 15% more or less MV 200-300 ml /kg
Tidal volume ml/kg in general or 6-8 ml/kg in ARDS

29
Alarms Pressure alarm for SIMV or volume mode
Expired TV alarm and MV alarm for Pressure mode Apnea alarm or high RR alarm

30
Noninvasive mechanical ventiation

32
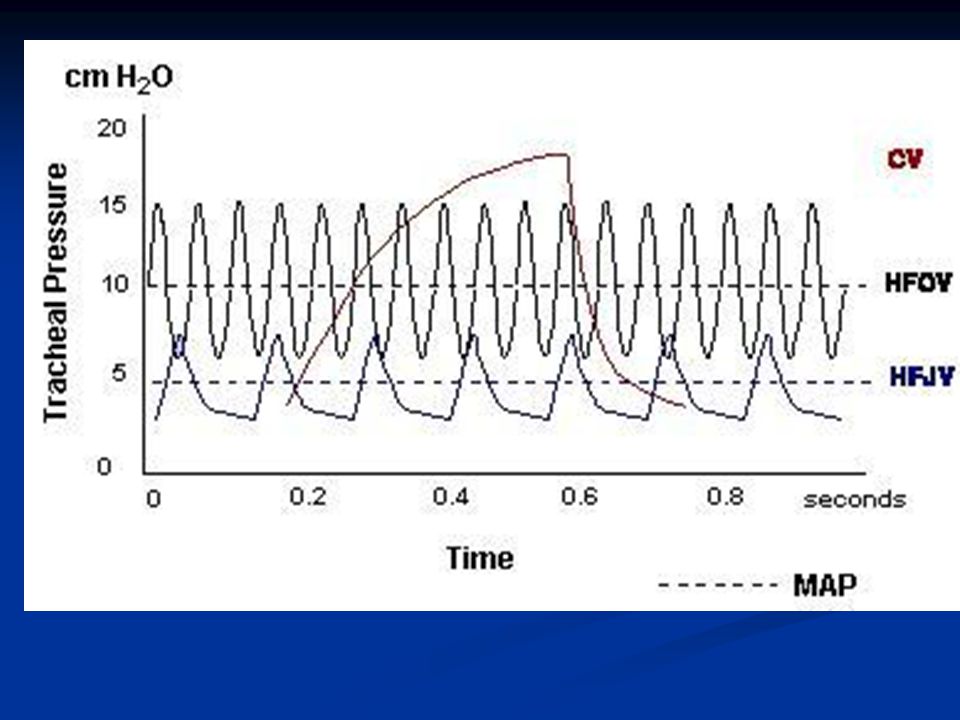
High frequency mechanical ventilation

35
Laminar Henderson

38
Indication 1. To serve as a ventilation mode when conventional ventilation has failed. 2. To provide a mode of ventilation that minimizes barotrauma, or damage, to the delicate tissue in the lungs.

39
Pediatric Indications
Neonatal Respiratory Distress Syndrome Persistent Pulmonary Hypertension Neonatal Meconium Aspiration Syndrome Congenital Diaphragmatic Hernia Neonatal Lung Hypoplasia Neonatal Air Leak Syndrome Pediatric ARDS/Pulmonary Interstitial Edema RSV Pneumonia

40
Monitoring

44
BP NIBP/IBP

45
CXR

46
End-tidal CO2

47
Bedside pulmonary mechanics

49
Weaning

50
Weaning C- Consciousness A- Airway L- Lung M- Muscle strength

51
Patient Ventilator In coordination (Fight)
Ventilator Malfunction Inappropriate setting Under or Over of Trigger sensitivity Under or Over of Peak flow Under or Over of inspiratory time Inadequate Tidal volume

















>")
>")
>")


>")

>")
>")

>")

