ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Management of Posterior Smooth Surface Caries
Somjin Ratanasathien, DDS, MS, PhD Department of Conservative Dentistry Faculty of Dentistry, Prince of Songkla University Jan 31 and Feb 4, 2008

2
Scopes Review of clinical features of posterior smooth surface caries
Clinical evaluation and restorative consideration Principle of cavity preparation for Class II restorations amalgam, resin composite and GIC Discussion

3
Scopes Overview of rationale of selection of restorative materials for restoration of posterior smooth surfaces Indications and contraindications for Class II amalgam and tooth-colored restorations Cavity features of Class II restorations and its rationale of cavity design amalgam resin composite glass ionomer cement

4
1. Rationale of Selection of Restorative Materials to Restore Posterior Smooth Surface Lesions
Tooth Factors Function of restored tooth If esthetics is concerned Material Factors Compressive strength Bonding c. tooth structure Dimensional changes, creep, wear resistance Durability of materials over time Esthetics

5
2-Yr Clinical Behavior of Unrestored Smooth Surface Lesions
From: Neilson A, Pitts NB (1991), The clinical behavior of free smooth surface carious lesions monitored over 2 years in a group of Scottish children, Br Dent J 171, Score 1 Score 2/3 All lesions Same scores 1472 (58%) 71 (32%) (56%) Regressed 480 (19%) 25 (11.3%) 505 (18%) Progressed (6%) 18 (8%) 171 (6%) Filled 45 (2%) 45 (20.4%) 90 (3%) Extracted 55 (2%) 25 (11.3%) 80 (3%) Loss to F/U (13%) 37 (17%) 374 (14%) Totals (100%) 221 (100%) (100%) Same Prog Reg Filled Ext. Loss From: Neilson A, Pitts NB (1991), The clinical behavior of free smooth surface carious lesions monitored over 2 years in a group of Scottish children, Br Dent J 171,
, The clinical behavior of free smooth surface carious lesions monitored over 2 years in a group of Scottish children, Br Dent J 171, Score 1 Score 2/3 All lesions. Same scores 1472 (58%) 71 (32%) 1542 (56%) Regressed 480 (19%) 25 (11.3%) 505 (18%) Progressed 153 (6%) 18 (8%) 171 (6%) Filled 45 (2%) 45 (20.4%) 90 (3%) Extracted 55 (2%) 25 (11.3%) 80 (3%) Loss to F/U 337 (13%) 37 (17%) 374 (14%) Totals 2542 (100%) 221 (100%) 2763 (100%) Same Prog Reg Filled Ext. Loss. From: Neilson A, Pitts NB (1991), The clinical behavior of free smooth surface carious lesions monitored over 2 years in a group of Scottish children, Br Dent J 171,")
7
Class II Amalgam
9
จะเห็นว่ารอยโรค Class I นั้นมี wall ล้อมรอบทั้ง 4 ด้าน ทิศทางการหลุด ในการบูรณะฟันด้วย amalgam จะมีทิศทางเดียว คือ O-G แต่ถ้าเป็น Class I cpd ทิศทางการหลุดมีแนว O-G และ B-L
11
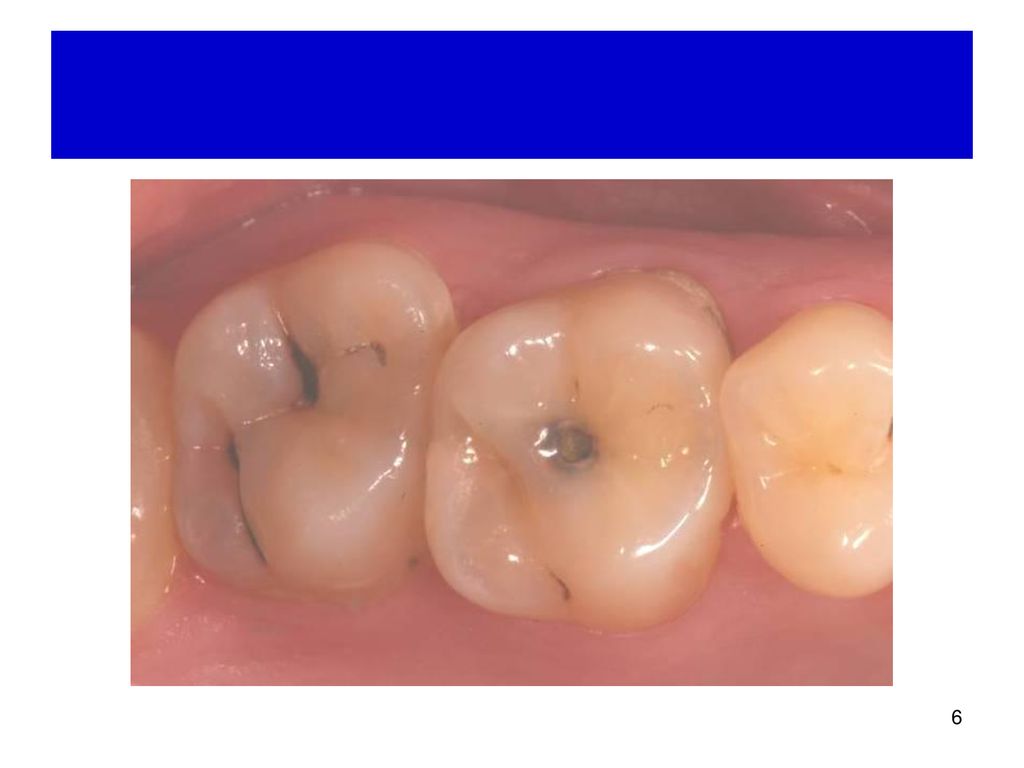
Various types of posterior smooth surface lesions (Class II cavity)
1. Rationale of Selection of Restorative Materials to Restore Posterior Smooth Surface Lesions Various types of posterior smooth surface lesions (Class II cavity) 1 proximal surface only 2 proximal surfaces 1 proximal surface + occlusal surface 2 proximal surfaces + occlusal surface 1-2 proximal surface(s) + occlusal surface + B/L surfaces
 1 proximal surface only. 2 proximal surfaces. 1 proximal surface + occlusal surface. 2 proximal surfaces + occlusal surface. 1-2 proximal surface(s) + occlusal surface + B/L surfaces.")
12
จากรูป ควรทำ preparation แบบไหน จึงจะเหมาะสมที่สุด
Factors to for consideration (Function, conservative tooth preparation, access, able to do retention, and resistance form) Then compare advantage and disadvantage Sequence priority of advantage and disadvantage
 Then compare advantage and disadvantage. Sequence priority of advantage and disadvantage.")
13
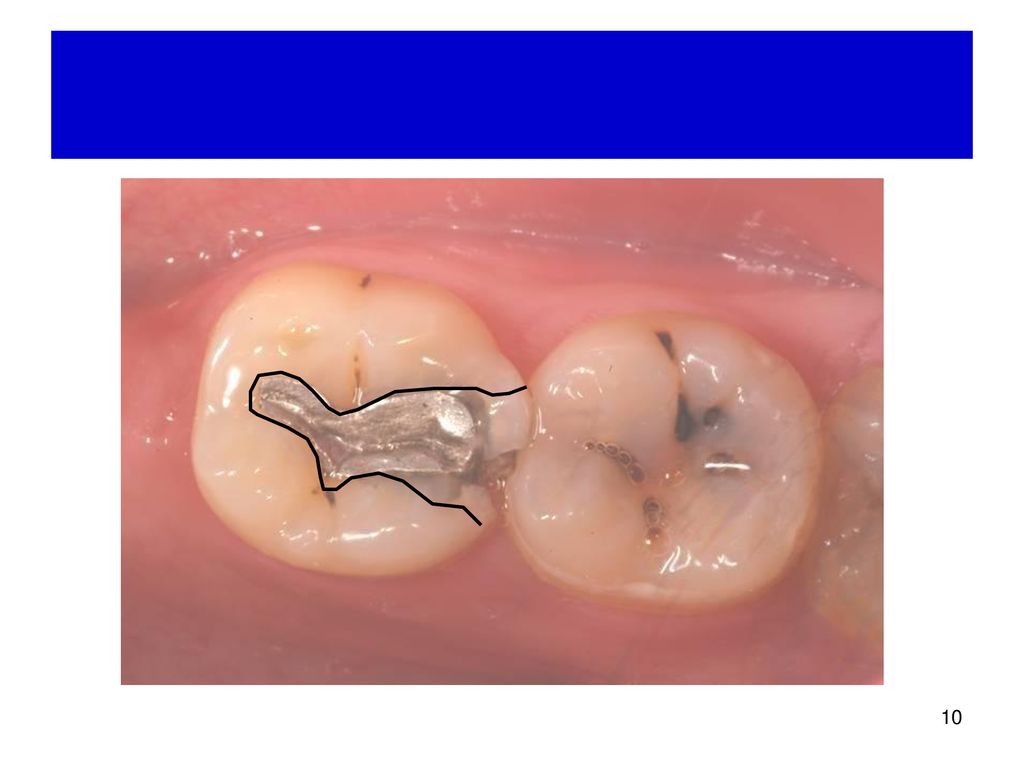
Class II: Cavity Design Direct vs. Indirect access
M/D view M/D view M/D view M/D view

14
Class II: Cavity Design Direct vs. Indirect access
M/D view M/D view M/D view M/D view

15
Class II: Cavity Design Direct vs. Indirect access Material Used
B พิจารณาจาก factors อะไร Access การควบคุมความชื้น ลักษณะ cavity หลังอุด สามารถทำขั้นตอน tooth preparation and restoration ได้ หรือ มี convenience form D C M/D view

16
Class II: Cavity Design Direct vs. Indirect access Material Used
B พิจารณาจาก factors อะไร Access การควบคุมความชื้น ลักษณะ cavity หลังอุด สามารถทำขั้นตอน tooth preparation and restoration ได้ หรือ มี convenience form แบบ B ไม่เหมาะในการทำ direct access for amalgam แม้ว่าจะมี access ในการทำก็ตาม เพราะจะเกิด undermined enamel หลังทำ การทำ slot preparation มองเห็นได้ยาก มีโอกาสที่จะ remove caries ไม่หมด เกิดเป็น residual caries ภายหลังได้ แบบ C เป็น root caries การทำ indirect access โดยเปิดจากข้างบนด้าน occlusal มักใส่ band ไม่ได้ดี เกิด overhanged margin ได้ ไม่ว่าจะเลือกบูรณะด้วยวัสดุอะไรก็ตาม แบบ D รอยโรคอยู่ใต้เหงือกบางส่วน การกรอไม่ระวังอาจโนเหงือก bleeding ได้ ยากต่อการควบคุมความชื้น ไม่เหมาะในการบูรณะด้วย resin composite ควรเลือก GI เพราะไม่รับแรง สามารถ release fluoride และ sensitive ต่อความชื้นน้อยกว่า resin composite และ มี biocompatibility ดีต่อเนื้อเยื่อ การเลือก direct accessถ้า conserve tooth preparation มากไป จะเกิด การremove caries ไม่หมด เกิดเป็น residual caries ภายหลังได้ รวมทั้งในการบูรณะก็ยากในการ insert โดยเฉพาะถ้าเป็น tooth colored material การฉายแสงทำได้ไม่สมบุรณ์ การอุดเกิน ไม่สามารถแก้ไขได้ หรือ ยากต่อการแก้ไขหรืออาจอุดขาด (void) D C M/D view
 D. C. M/D view.")
18
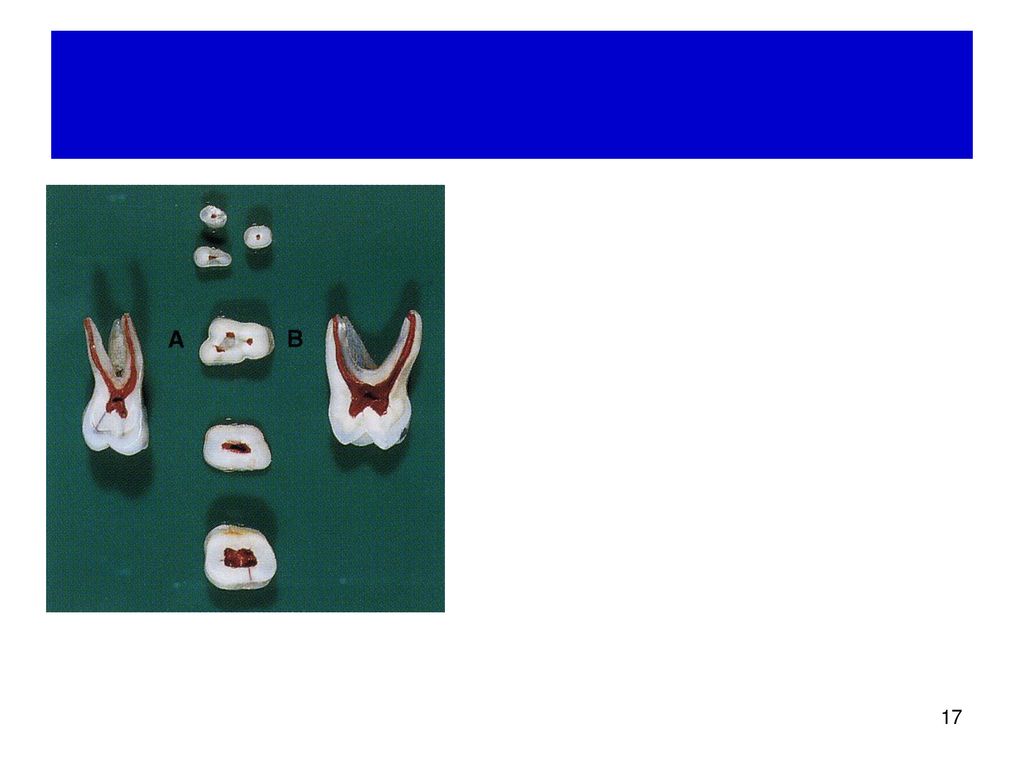
ใต้ contact มี concave area

19
Class II (AF): Cavity Design Direct vs. Indirect access
M/D view

20
How to do direct access with the most tooth conservative tooth preparation?
If proximal lesion can’t be seen from occlusal view, how can we drill through sound enamel and dentin to find the lesion with the most conservative tooth preparation? เจาะหารอยโรคอย่างไร จึงจะเสียเนื้อฟันน้อยที่สุด

22
2. Cavity Design for Class II Amalgam
Outline Direct vs. indirect O: Reverse S-curve Proximal Retention form Resistance form Convenience form

23
Resistance Form for Amalgam
Conservative tooth preparation as much as possible Along direction of enamel rod unsupported enamel Minimize stress: no sharp line angle Sufficient thickness

24
Retention of Amalgam Major Minor (accessories, additional)
Slightly convergence to occlusal surfaces Box Dove tail Undercut Minor (accessories, additional) Retentive grooves
 Retentive grooves.")
25
Design of Class II-Amalgam

26
Retention Direct: Parallelism/undercut of O-G or M-D
Slot or box: Parallelism of B and L-walls Dovetail Conventional: dovetail extension along groove or pit Modified: extension of very narrow grooves along grooves

27
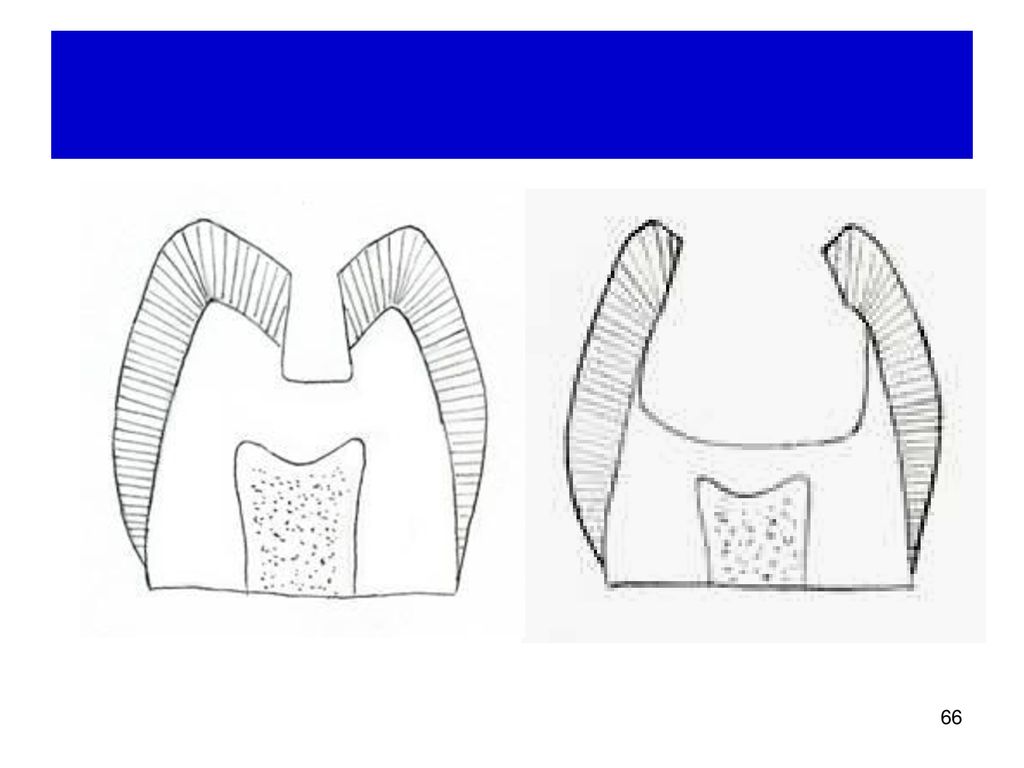
Clinical Features of Class II Amalgam Slot vs. Dovetail
What factors determine if cavity design should be slot or dovetail!

28
Class II Amalgam: Slot vs. Dovetail
Conservative Tooth Preparation as much as possible Slot Caries outline is within contact point (B-L). If outline extends beyond contact point, it should not extend beyond both line angles simultaneously. Dovetail Initial caries removal and cavity preparation shows insufficient retention, though no involvement of occlusal caries. Need to increase retention. Involvement of occlusal caries or previous old amalgam restoration. Less than 0.5 mm distance between 2 proximal cavities, join 2 cavities for MOD.
. If outline extends beyond contact point, it should not extend beyond both line angles simultaneously. Dovetail. Initial caries removal and cavity preparation shows insufficient retention, though no involvement of occlusal caries. Need to increase retention. Involvement of occlusal caries or previous old amalgam restoration. Less than 0.5 mm distance between 2 proximal cavities, join 2 cavities for MOD.")
29
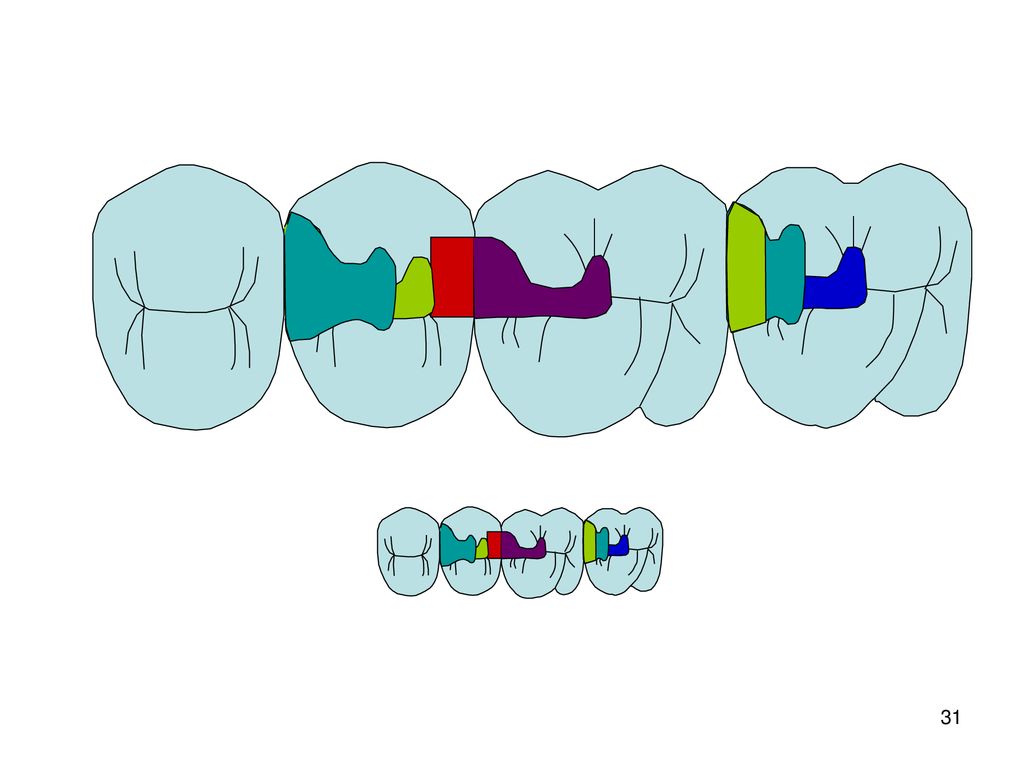
Picture / Diagram Slot Dovetail

30
What factors have influenced on Class II amalgam design: Slot vs
What factors have influenced on Class II amalgam design: Slot vs. Dovetail? Size of lesion: O-G, M-D, B-L

32
Outline: Reverse S-Curve
What is reverse S-curve? Why do we need to do reverse S-curve? When do we do reverse S-curve? Where do we do reverse S-curve in the cavity design? How do we do reverse S-curve?

33
Reverse S-curve What, Why, When, Where

34
Homework: Outline reverse S-curve

35
Outline: Proximal Surface

36
Class II Amalgam Conventional Dovetail
Retention (O-G) B-L walls: Parallelism Proximal box: slightly convergent to occlusal surface Retention (M-D) 3. B-L walls: Parallelism 4. (Retentive grooves at axio- buccal and lingual line angles) Resistance form Tooth: Cavosurface margin ~90 20° Angle of departure ~90 20° Definite but not sharp internal line angle Amalgam: Same as tooth + Minimal cavity depth ~1.5 mm
 B-L walls: Parallelism. Proximal box: slightly convergent to occlusal surface. Retention (M-D) 3. B-L walls: Parallelism. 4. (Retentive grooves at axio- buccal and lingual line angles) Resistance form. Tooth: Cavosurface margin ~90 20° Angle of departure ~90 20° Definite but not sharp internal line angle. Amalgam: Same as tooth + Minimal cavity depth ~1.5 mm.")
37
Class II Amalgam Conventional Dovetail
Retention (O-G) B-L walls: slightly convergent to occlusal surface Proximal box: slightly convergent to occlusal surface Retention (M-D) 3. Dovetail 4. (Retentive grooves at axio- buccal and lingual line angles) Resistance form Tooth: Cavosurface margin ~90 20° Angle of departure ~90 20° Definite but not sharp internal line angle Amalgam: Same as tooth + Minimal cavity depth ~1.5 mm Beveled axio-pulpal line angle
 B-L walls: slightly convergent to occlusal surface. Proximal box: slightly convergent to occlusal surface. Retention (M-D) 3. Dovetail. 4. (Retentive grooves at axio- buccal and lingual line angles) Resistance form. Tooth: Cavosurface margin ~90 20° Angle of departure ~90 20° Definite but not sharp internal line angle. Amalgam: Same as tooth + Minimal cavity depth ~1.5 mm. Beveled axio-pulpal line angle.")
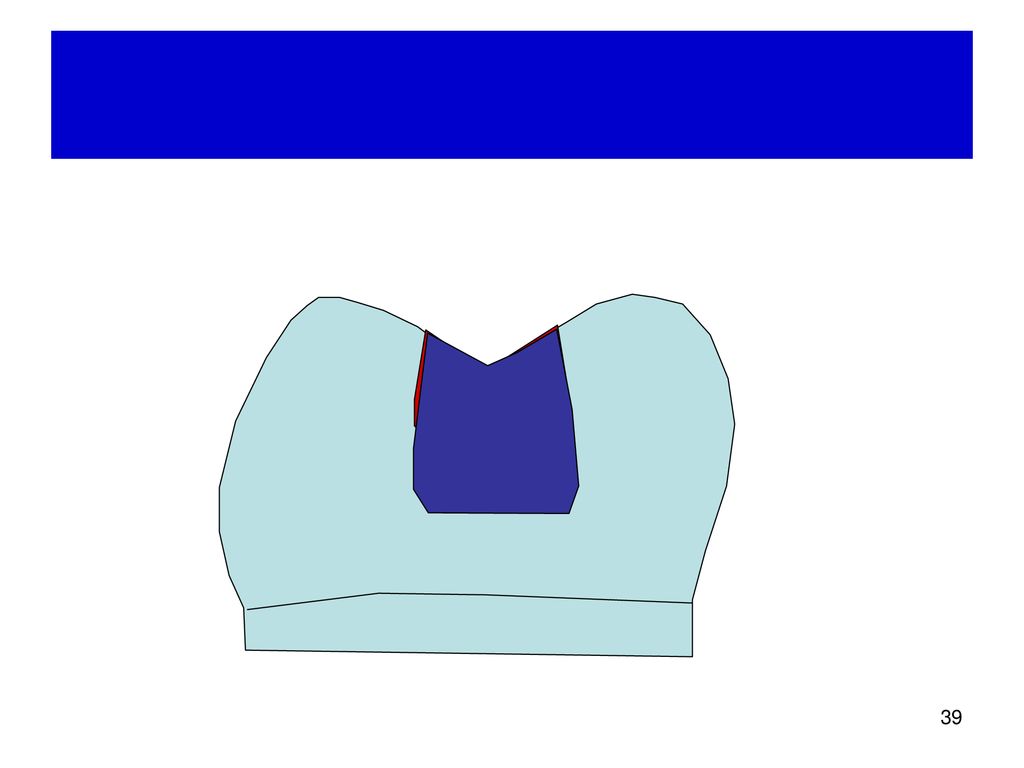
38
Class II Amalgam Modified Dovetail
Retention (O-G) B-L walls: Parallelism Proximal box: slightly convergent to occlusal surface Retention (M-D) 3. B-L walls: Parallelism 4. (Retentive grooves at axio- buccal and lingual line angles) Resistance form Tooth: Cavosurface margin ~90 20° Angle of departure ~90 20° Definite but not sharp internal line angle Amalgam: Same as tooth + Minimal cavity depth ~1.5 mm Beveled axio-pulpal line angle
 B-L walls: Parallelism. Proximal box: slightly convergent to occlusal surface. Retention (M-D) 3. B-L walls: Parallelism. 4. (Retentive grooves at axio- buccal and lingual line angles) Resistance form. Tooth: Cavosurface margin ~90 20° Angle of departure ~90 20° Definite but not sharp internal line angle. Amalgam: Same as tooth + Minimal cavity depth ~1.5 mm. Beveled axio-pulpal line angle.")
40
Clinical Features of Class II Amalgam Slot Preparation
Resistance form for tooth and amalgam Cavosurface margin~90° parallelism of B-L walls Angle of departure~90° Retention form O-G: Paralellism of B-L walls Proximal box: convergent to occlusal surface, box form M-D: (Retentive groove at axio-buccal and lingual line angles)
")
41
Clinical Features of Class II Amalgam Slot Preparation
Advantages More conservative tooth preparation than dovetail design resistance form for tooth better than dovetail design Disadvantages Require great care preparation: easily damage adjacent tooth surfaces Less retention than dovetail design, but sufficient

42
Comparison of Tooth Strength Slot vs. Dovetail

44
Posterior Smooth Surface Caries
จากรูปที่เห็น ควรจะทำ cavity design แบบไหน มีแนวคิดในการตัดสินใจเลือกทำแบบไหนอย่างไร ด้วยเหตุผลหรือเงื่อนไข

45
จากรูปที่เห็น ควรจะทำ cavity design แบบไหน มีแนวคิดในการตัดสินใจเลือกทำแบบไหนอย่างไร ด้วยเหตุผลหรือเงื่อนไข

46
จากรูปที่เห็น ควรจะทำ cavity design แบบไหน มีแนวคิดในการตัดสินใจเลือกทำแบบไหนอย่างไร ด้วยเหตุผลหรือเงื่อนไข

47
จากรูป ควรทำ preparation แบบไหน จึงจะเหมาะสมที่สุด
Factors to for consideration (Function, conservative tooth preparation, access, able to do retention, and resistance form) Then compare advantage and disadvantage Sequence priority of advantage and disadvantage
48
Masticatory Force Tooth Molar Premolar Canine Incisor Force
127 lb (565 N) 65 lb (288 N) 47 lb (208 N) 35 lb (155 N)
 65 lb (288 N) 47 lb (208 N) 35 lb (155 N)")
49
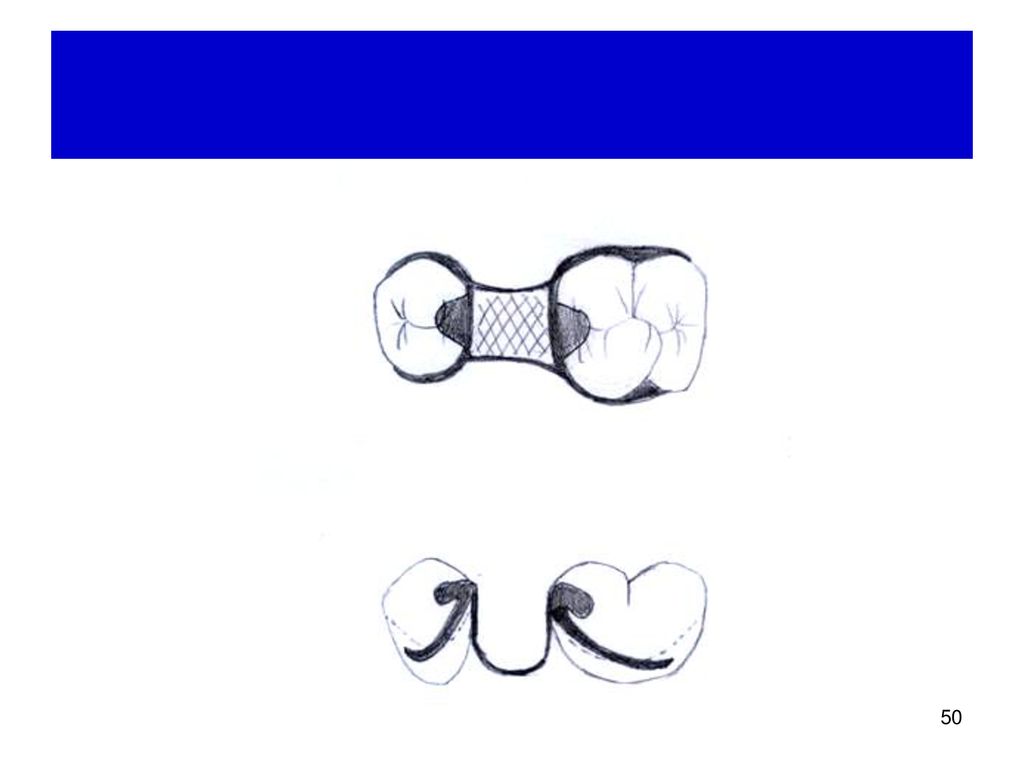
Class II (AF): Cavity Design
Direct Proximal box Dove tail M/D view

51
Prosthodontic Consideration
Rest Guiding plane Retentive tips: Clasp arms Reciprocal Force Wear Survey line

52
Design of Class II Amalgam Cavity Preparation
From: Soderholm et al (1998), Determinants of quality of operative dentistry, Crit Rev Oral Biol Med 9(4),
, Determinants of quality of operative dentistry, Crit Rev Oral Biol Med 9(4),")
53
Summary Cavosurface angle affects adaptation and marginal degradation of the amalgam restorations Depth of preparation Width of preparation: large >3:5 or 2/3: reduce strength of cusps narrow < 1 mm: poor condensation --> porosity and poor adaptation Margin roughness Proximal retentive grooves Internal line angle

54
Treatment of Tooth Defects

55
Tooth Preparation for a Resin Composite Restoration
Remove the fault, defect, old material, or friable tooth structure Creating prepared enamel margins of 90+ Creating 90 (butt-joint) cavosurface margins root surfaces Roughening the prepared tooth structure (enamel and dentin) with a diamond bur
 cavosurface margins root surfaces. Roughening the prepared tooth structure (enamel and dentin) with a diamond bur.")
56
Variation of Cavity Design for Class II Resin Composite
Box form ± bevel Divergent to external tooth surface Convergent to external tooth surface

57
Guidelines for CR Tooth Preparation
CR: less outline extension (adjacent suspicious or at-risk areas [grooves or pits] may be “sealed” rather than restored CR: an axial and/or pulpal wall of varying depth (not uniform) Incorporation of an enamel bevel at some areas (the width of which is dictated by the need for secondary retention) Tooth preparation walls being rough (to increase the surface area for bonding) Use of a diamond bur (to increase the roughness of the tooth preparation walls)
 Incorporation of an enamel bevel at some areas (the width of which is dictated by the need for secondary retention) Tooth preparation walls being rough (to increase the surface area for bonding) Use of a diamond bur (to increase the roughness of the tooth preparation walls)")
58
Indications for CR: Cl II
Small and moderate restorations, preferably with enamel margins Most premolar or first molar restorations, particularly when esthetics is considered A restoration that does not provide all of the occlusal contacts A restoration that does not have heavy occlusal contacts A restoration that can be appropriately isolated during the procedure Some restorations that may serve as foundations for crowns Some very large restorations that are used to strengthen remaining weakened tooth structure (for economic or interim use reason)
")
59
Contraindications for Posterior CR: Cl II
Operating sites cannot be appropriately isolated Heavy occlusal forces All the occlusal contacts only on composite In restorations that extend onto the root surface

60
Advantages of CR Esthetics Conservative tooth structure removal
Easier, less complex tooth preparation Economics (compared to crowns and indirect tooth colored restorations) Insulation Bonding benefits Decreased microleakage Decreased recurrent caries Decreased postoperative sensitivity Increased retention Increased strength of remaining tooth structure
 Insulation. Bonding benefits. Decreased microleakage. Decreased recurrent caries. Decreased postoperative sensitivity. Increased retention. Increased strength of remaining tooth structure.")
61
Disadvantages of CR Material related Require more time to place
Greater localized wear Polymerization shrinkage effects Linear coefficient of thermal expansion (LCTE) Biocompatibility of some components unknown Require more time to place More technique sensitive More expensive than amalgam restorations
 Biocompatibility of some components unknown. Require more time to place. More technique sensitive. More expensive than amalgam restorations.")
62
Disadvantages of CR as a Posterior Restorative Material
Secondary caries Polymerization shrinkage Water Sorption Variable degrees of polymerization Inconsistent dentin bonding (marginal leakage) Technique sensitivity Questionable durability
 Technique sensitivity. Questionable durability.")
63
Resin Composite

64
Class II: Posterior CR Lesion size: Lesion depth: Technique sensitive
Small size (<1/3 B-L cusp) Esthetics concern Avoid centric occlusal contacts Large size (support cusp fracture, tooth crack) Lesion depth: Mount site 1 size 1 = initial lesion (enamel caries) Technique sensitive Supragingival margin Depth of proximal box (occluso-gingival margin) Tooth hypersensitive
 Esthetics concern. Avoid centric occlusal contacts. Large size (support cusp fracture, tooth crack) Lesion depth: Mount site 1 size 1 = initial lesion (enamel caries) Technique sensitive. Supragingival margin. Depth of proximal box (occluso-gingival margin) Tooth hypersensitive.")
65
Variable Degrees of Polymerization
<75% polymerization when curing in air environment Degree of polymerization Formulation: monomer:resin:filler Curing light unit: watt intensity, distance between light tip and cavity Operator

67
CR-Technique Sensitive
LC unit α Light intensity Distance CR Thickness Shade Filler amount Other interference Access E,D

68
Polymerization Shrinkage of Resin Composite
C-factor: bonded surface/unbonded surface Usually < 8 MPa Class I > Class II Water soprtion

69
Greater C-factor increased internal stress
Configuration Factor Greater C-factor increased internal stress

70
Configuration Factor C.L. Davidson (1984)
C-factor = bonded surface unbonded surface Polymerization shrinkage: 1-2%: dependent on type of CR (filler/monomer ratio) Indicate internal stress of resin composite after polymerization Usually C-factor < 8 MPa
 Indicate internal stress of resin composite after polymerization. Usually C-factor < 8 MPa.")
71
Water Absorption of CR Increased dimension Gradual change

72
Retention of CR Restoration = bonding surface (area and etching) – polymerization shrinkage (C-factor) + water abs.
 – polymerization shrinkage (C-factor) + water abs.")
73
Durability of Resin Composite Restoration
Polymeric resin subjected to Hydrolysis Enzyme degradation: esterase

74
Surface Roughness of Resin Composite vs. Color Staining

75
Failure Load in Various Design of Class II Cavity Preparation for CR
Occlusal extension B-L width = 2.0 ± 0.25 mm O-Depth = 1.8 ± 0.30 mm Proximal: B-L width = 2.25 ± 0.25 mm, P-Depth = 2.75 ± 0.25 mm, O-G height of axial wall = 1.75 ± 0.25 mm 2. Slot: O-G: 3.25 ± 0.25 mm, Ging depth = 1.25 ± 0.25 mm 3. Retentive groove: 0.33 mm deep 297 ± 72 N Summittt et al. 1994, Quintessence Int 25,

76
Radiographic and SEM Evaluation of Class II Resin Composite
placed 144 CR (Clearfil Ray) in vivo 3 adhesives: Photobond, Scotchbond MP+, Linerbond2 3 Techniques: transparent matrix+ increment metal matrix (increment, bulk) 2 evaluator, faculty and dental senior student Opdam et al. (1998), J Dent 26,
 in vivo. 3 adhesives: Photobond, Scotchbond MP+, Linerbond2. 3 Techniques: transparent matrix+ increment. metal matrix (increment, bulk) 2 evaluator, faculty and dental senior student. Opdam et al. (1998), J Dent 26,")
77
Radiographic (underfilled)
")
78
SEM (Overfilled)
")
79
SEM (Overfilled & Underfilled)
")
80
SEM (Underfilled)
")
81
X-ray SEM Overfilled 4 44 Underfilled 33 25 Overhanged - 7 Flush DBA
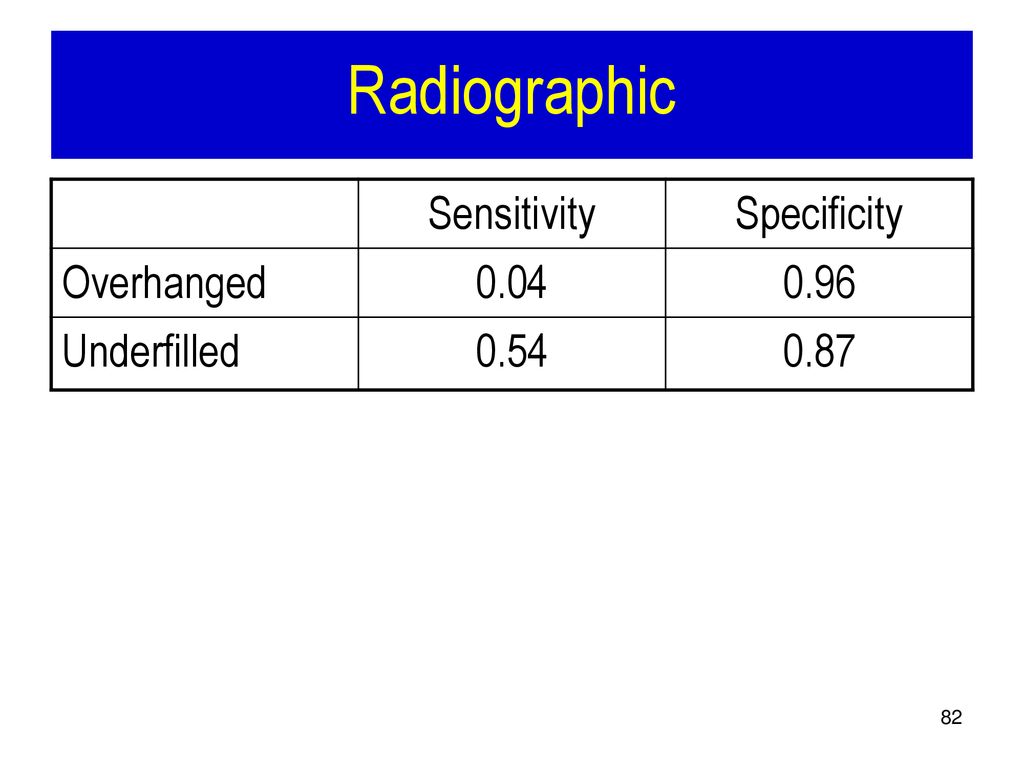
32 Overfilled CR was difficult to be seen in radiograph. Quality of cervical margin was not dependent on matrix system, filling procedure, and experience of operator

82
Radiographic Sensitivity Specificity Overhanged 0.04 0.96 Underfilled
0.54 0.87
83
Radiographic Analysis
Over filled Correct Under Mean SD Liner Bond 2 48 5 52 43 2.91± PhotoBond 2 91 7 3.65 Scotchbond MP 49 45 2.97

84
From: Raskin et alI (1999), Clinical evaluation of posterior composite 10-yr report, J Dent 27,
, Clinical evaluation of posterior composite 10-yr report, J Dent 27,")
85
From: Raskin et al (1999), Clinical evaluation of posterior composite 10-yr report, J Dent 27,
, Clinical evaluation of posterior composite 10-yr report, J Dent 27,")
86
From: Raskin et al (1999), Clinical evaluation of posterior composite 10-yr report, J Dent 27,
, Clinical evaluation of posterior composite 10-yr report, J Dent 27,")
87
From: Raskin et al (1999), Clinical evaluation of posterior composite 10-yr report, J Dent 27,
, Clinical evaluation of posterior composite 10-yr report, J Dent 27,")
88
Class II – Resin Composite
Sandwich technique

89
Sandwich Restoration Close sandwich Open sandwich

90
Durability of Resin Composite

91
Question If resin composite fails, predict the common location of failure. occlusal vs. gingival fracture of resin composite vs. fracture at the bonding interface

92
Class II – Glass Ionomer
Root caries: direct access Indirect access Tunnel preparation Sandwich technique

93
Class II – GI Restorations
Indications Root caries Contraindications Areas subjecting to compressive force Areas subjecting to wear

94
Tunnel Restoration

95
Tunnel Restoration N = 318 3.5 yr F/U Permanent Primary Success rate
74% 10% Failure 35%: MR fracture 31%: cavitation in approximal enamel 38%: recurrent caries 82%: MR fracture From: Hasselrot (1993), Tunnel restorations. A 3 1/2-year follow up study of Class I and II tunnel restorations in permanent and primary teeth, Swed Dent J 17(5),
, Tunnel restorations. A 3 1/2-year follow up study of Class I and II tunnel restorations in permanent and primary teeth, Swed Dent J 17(5),")
96
Factors Affecting Tooth Preparation
Operator Diagnosis: rationale for operative Tx Dental anatomy: Enamel rod, conservative tooth preparation Patient Age Economic status Complication: moisture control

97
Reasons for Replacements of Restorations
Amalgam (%) GI (%) CR(%) 2° caries 50 42.4 38.6 1° caries 6.5 4.9 2.5 Fractures 33.4 39.2 46.9 Esthetics 1.7 1.0 3.5 Others 8.4 12.6 8.5 Total No of Restoration 1827 309 1548 From: Forss H, Widstrom E (2001), From amalgam to composite: selection of restorative materials and restorative longevity in Finland, Acta Odontol Scand 59,
 GI (%) CR(%) 2° caries ° caries Fractures Esthetics Others Total No of Restoration From: Forss H, Widstrom E (2001), From amalgam to composite: selection of restorative materials and restorative longevity in Finland, Acta Odontol Scand 59,")
98
Longevity of Restorations
Age AF CR GI 20-39 yr 10.5 4 4.5 40+ yr 13.5 5.8 5

99
Life Expectancy of Restorations
From: Forss H, Widstrom E (2001), From amalgam to composite: selection of restorative materials and restorative longevity in Finland, Acta Odontol Scand 59,
, From amalgam to composite: selection of restorative materials and restorative longevity in Finland, Acta Odontol Scand 59,")
100
References Sturdevant’s Art and Science of Operative Dentistry, Chapter 13-14, p Schwartz, Summitt and Robbins (2001), Fundamentals of Operative Dentistry (2nd Ed), Quintessence Pub, Chicago.
, Fundamentals of Operative Dentistry (2nd Ed), Quintessence Pub, Chicago.")
101
Advantages of Reverse-S curve
Conservative tooth preparation / Preserve tooth structure Maintain retention form: Maintain resistance form: angle of departure ~ 90º

งานนำเสนอที่คล้ายกัน