ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Facilitator: Pawin Puapornpong
Case study 50 Facilitator: Pawin Puapornpong

2
CASE ผู้ป่วยหญิงไทยตั้งครรภ์อายุ 34 ปี มารับการตรวจที่แผนกฉุกเฉินด้วยเรื่อง มีเลือดออกจากช่องคลอดผิดปกติ ประวัติปัจจุบัน 1 day PTA มีเลือดออกจากช่องคลอดเป็นหยดๆ ไม่มีไข้ ปัสสาวะอุจจาระปกติ

3
CASE ประวัติทางสูติ-นรีเวช มีบุตร 2 คน คนโตอายุ 6 ปี คนเล็กอายุ 3 ปี ประจำเดือนมาทุกเดือน เดือนละ 3-5 วัน ใช้ผ้าอนามัยจำนวนปกติ ประจำเดือนครั้งสุดท้ายประมาณ 8 เดือนก่อน ประวัติโรคประจำตัว ประวัติส่วนตัวและครอบครัว ไม่มีประวัติโรคเลือด ไม่เคยมีจ้ำเลือดออกผิดปกติ ไม่มีประวัติแพ้ยาหรือกินยาชนิดใดเป็นประจำ ผู้ป่วยทำงานที่บ้าน ที่พักอยู่กับสามีและลูก 2 คน สามีอาชีพรับจ้าง

4
HISTORY TAKING เลือดที่ออกปริมาณเท่าไหร่ ระยะเวลา
ลักษณะของเลือดเป็นอย่างไร อาการเจ็บครรภ์ เจ็บช่องคลอด น้ำเดิน มีมูกเลือดผิดปกติร่วมด้วยหรือไม่ ลูกยังดิ้นดีหรือไม่ ไข้ ประวัติเกี่ยวกับเรื่อง Infection ตกขาวผิดปกติ ปัสสาวะอุจจาระปกติหรือไม่ ประวัติเกี่ยวกับการฝากครรภ์ ANC risk ประวัติการตั้งครรภ์ครั้งก่อน ภาวะความดันโลหิตสูงขณะตั้งครรภ์ ประวัติรกลอกตัวก่อนกำหนดในครรภ์ก่อน

5
ประวัติการได้รับบาดเจ็บบริเวณท้อง เนื้องอกมดลูก
HISTORY TAKING ประวัติการได้รับบาดเจ็บบริเวณท้อง เนื้องอกมดลูก ประวัติโรคประจำตัว เช่นโรคเลือด สูบบุหรี่ การเสพสารเสพติด ประวัติครอบครัว : พี่สาว/น้องสาวมีประวัติรกลอกตัวก่อนกำหนด

6
PV, PR : ห้ามตรวจจนกว่าจะสามารถ R/O placenta previa ได้
PHYSICAL EXAMINATION Vital signs Signs of shock HEENT Abdomen Fundal height : ทำเครื่องหมายสังเกตว่ามดลูกขนาดโตขึ้นอย่างรวดเร็วหรือไม่ Uterine contraction : duration, interval, intensity, tone and tenderness Leopold’s maneuver : lie, presentation, engagement, EFW FHR monitoring : NST, CST PV, PR : ห้ามตรวจจนกว่าจะสามารถ R/O placenta previa ได้ Extremities : pitting edema

7
Problem list Antepartum hemorrhage 1 day PTA Uncertain LMP FHS unclear The fetus is in transverse lie

8
Differential diagnosis
Placenta previa Abruptio placentae Ruptured vasa previa

9
CBC with platelet count
LAB INVESTIGATION CBC with platelet count Grouping and matching for whole blood or PRC 2-6 units Coagulogram : PT , PTT , INR Fibrinogen and D-dimer or fibrin degradation product(FDP) Venous clotting time(VCT) Ultrasound
 Venous clotting time(VCT) Ultrasound.")
10
Placenta previa

11
Placenta Previa Definition: Presence of placental tissue over or adjacent to the cervical os Total placenta previa Partial placenta previa Marginal placenta previa Low lying placenta previa

12
Placenta previa Obstetric emergency Preterm birth, Perinatal mortality Maternal morbidity and mortality

13
Placenta Previa Incidence 0.5% of pregnancy
Previous placenta previa-> 2-3% Prior ceasarean delivery -> 5% (grand multipara)
")
14
Placenta Previa Placental migration Near term
Increase lower uterine segment Trophoblastic tissue growth away from the fundus

15
Placenta Previa Risk factor Increasing Parity and/or Maternal age
age 35 yrs 1% , 40 yrs 2% ( normal 0.5) Maternal race Cigarette smoking (3 times) Residence of higher elevation Previous placenta previa Prior curettage Prior cesarean delivery MSAFP รกใหญ่หรือรกผิดปกติ
 Maternal race. Cigarette smoking (3 times) Residence of higher elevation. Previous placenta previa. Prior curettage. Prior cesarean delivery. MSAFP. รกใหญ่หรือรกผิดปกติ")
16
History and Physical Examination
Placenta Previa History and Physical Examination Painless third-trimester bleeding Anemia True labor paimuterine contraction Abnormal presentation Cephalic presentationno engagement Normal FHR

17
Transabdominal Ultrasound
Placenta Previa Radiology Transabdominal Ultrasound 95% False Positive : Bladder distension False negative : รกเกาะด้านบนแต่คลุมลงมาด้านล่าง Transvaginal Ultrasound 100% If can’t see in transabdominal Transperineal ultrasound MRI

18
Pervaginal examination
Placenta Previa Pervaginal examination Double set-up

19
Placenta Previa Management 3 FACTORS Fetal age and thus maturity Labor
Bleeding and its severity

20
Placenta Previa Early management Admit LR
Maternal monitoring: Vital sign, Urine input/output Fetal heart rate monitoring CBC Grouping and Matching for whole blood and PRC NPO, IV fluid

21
ตกเลือดจากรกเกาะต่ำ เลือดหยุด ผ่าท้องคลอด เลือดหยุดเอง เลือดออกมาก
ครรภ์ครบกำหนด ผ่าท้องคลอด ครรภ์ก่อนกำหนด หรือ น้อยกว่า 34 สัปดาห์ เลือดหยุดเอง - เฝ้ารอ - ให้ยา steroid เจ็บครรภ์ก่อนกำหนด - ให้ยา tocolysis เลือดหยุด เลือดออกมาก ทำการผ่าตัด เฝ้ารอครรภ์ครบกำหนดแล้วผ่าท้องคลอด เลือดออกมาก

22
Maternal complication
Placenta Previa Maternal complication Death: <1:1,000 Placenta accreta/increta/percreta Cesarean delivery 1 ครั้ง 20-25% 2 ครั้ง 50% Cesarean Hysterectomy Postpartum hemorrhage Infection

23
Neonatal complication
Placenta Previa Neonatal complication Preterm birth, Perinatal Mortility Birth Asphyxia

24
Abruptio placenta

26
Abruptio placenta Placental abruption, Ablatio placentae, Premature separation of the normally implanted placenta Definition

27
Abruptio placenta Cause and risk factor Gestational hypertension & Preeclampsia Prior abruption Old age maternal Race Family history Preterm premature rupture of membrane Smoking Cocaine Thrombophilias Traumatic abruption Leiomyoma Multifetal gestation Iatrogenic trauma Chorioamnionitis Shortened umbilicus Circumvillatte placenta

28
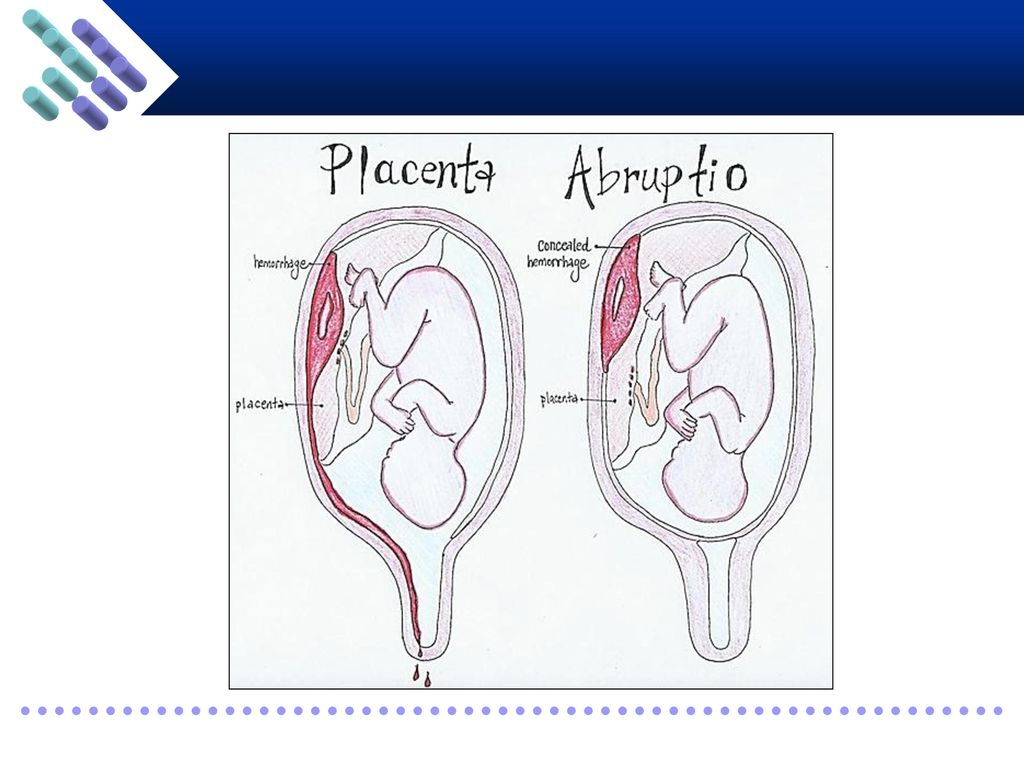
ข้อมูลตามพยาธิสภาพ Revealed Concealed อุบัติการณ์ 80-85% 15-20% จุดเริ่มของการลอกตัว ริมรก กลางรก อาการกับปริมาณเลือดที่ออก สัมพันธ์ ไม่สัมพันธ์ Uterine tenderness and hypertonicity ไม่เด่นชัด เด่นชัด Couvelaire uterus น้อย บ่อย Fetal distress Consumptive coagulopathy Fundal height คงที่ สูงขึ้นชัดเจน

29
Abruptio placenta Diagnosis History : sign & symptoms Ultrasound PV Examination of the placenta

30
Abruptio placenta Management Lab investigation : CBC, BUN/Cr, coagulogram, fibrionogen+FDP Correct anemia, hypovolemia, hypoxia, electrolyte imbalance Record input/output Consumptive coagulopathy -> FFP, cryoprecipitate, fresh whole blood

31
Abruptio placenta Management Termination of pregnancy C/S -> เมื่อมีindication เช่น fetal distress Conservative treatment -> GA<34 wk Tocolytic -> MgSo4

32
Abruptio placenta: Complication
แม่ ลูก Consumptive coagulopathy Renal failure Uteroplacental apoplexy (Couvelaire uterus) Postpartum hemorrhage Sheehan’s syndrome Endometritis Blood transfusion complicaiton Prematurity Asphyxia & fetal distress (uteroplacental insufficiency) Intrauterine fetal death Increase morbidity & mortality
 Postpartum hemorrhage. Sheehan’s syndrome. Endometritis. Blood transfusion complicaiton. Prematurity. Asphyxia & fetal distress (uteroplacental insufficiency) Intrauterine fetal death. Increase morbidity & mortality.")
33
Vasa previa

34
Velamentous cord insertion Vasa previa
Contents Placenta Velamentous cord insertion Pathogenesis Vasa previa Physical examination Diagnosis Management

35
Placenta

36
Velamentous cord insertion
Fetal blood vessels insert into area between amnion and chorion instead of placenta Unprotected by Wharton’s jelly

37
Velamentous cord insertion
1% of singleton gestation 15% of monochorionic twin gestations

38
Pathogenesis Remains unknown; most likely hypothesis is:
Cord initially inserts centrally Part of the placenta actively proliferates toward the well-vascularized uterine fundus (trophotropism); while the other part involutes Cord unable to follow the migration of the placenta Progressively becomes peripheral
; while the other part involutes Cord unable to follow the migration of the placenta Progressively becomes peripheral.")
39
Vasa previa Passage of blood vessels over the internal os below the presenting part of fetus “Velamentous insertion” over internal os

40
Vasa previa Very rare: 1 in 2500 pregnancy
Fetal mortality 60% if rupture Pathogenesis: similar to velamentous cord insertion Types Type 1: Occur with velamentous insertion Type 2: Occur with bilobed placenta or placenta with succenturiate lobe

41
Physical examination:
Vasa previa Physical examination: Rarely found Pulsatile vessel over cervical os Palpable on digital examination

42
Vasa previa Prenatal diagnosis: Perform if: Velamentous cord insertion
Pregnancies conceived following use of assisted reproductive technologies in vitro fertilization 2nd trimester low-lying placentas Placenta previa [even if it has resolved] Bilobed or succenturiate lobe placentas in the lower uterine segment Multiple gestations

43
Vasa previa Prenatal diagnosis:
Real-time transvaginal color Doppler ultrasound imaging Highly diagnostic Sensitivity 78% Specificity 91% MRI when diagnosis via Doppler ultrasound is uncertain

44
Vasa previa Transvaginal ultrasound images showing a posterior placenta with an anterior succinturiate lobe complicated by vasa previa

45
Vasa previa Clinical diagnosis:
Suspect when rupture of membrane occur with fetal bradycardia [particularly sinusoidal pattern or bradycardia] Due to fetal distress Need of immediate delivery Post-partum diagnosis by placental examination

46
Vasa previa Confirmation test:
To differentiate fetal blood from maternal blood e.g.: Apt test, Kleihauer-Betke test, Ogita’s test, Londersloot’s test, etc. Not done clinically due to time requirement

47
Vasa previa Apt test: “Alkali denaturation test” or “Apt–Downey test”
Mix blood with water for hemolysis mix with NaOH Positive test: fetal blood [remains pink] Negative test: maternal blood [turns to yellow-brown]

48
Vasa previa Treatment Requires Cesarean section for delivery
Always look for pulsatile vessels over cervical os before performing artificial rupture of membrane Emergency Cesarean delivery if: Premature rupture of membranes Repetitive variable decelerations refractory to tocolysis Vaginal bleeding accompanied by fetal tachycardia, a sinusoidal heart rate pattern, or evidence of pure fetal blood by Apt test or Kleihauer-Betke assessment

49
References and image sources
Drife J, Magowan BA. Clinical Obstetrics and Gynaecology. Edinburgh, UK: Saunders, 2004 ACOG, Beckmann CRB, Ling FW, Barzansky BM, Herbert WN, Laube DW, Smith RP. Obstetrics and Gynecology, 6th edition. Baltimore, MD: Lippincott Williams & Wilkins, 2010

งานนำเสนอที่คล้ายกัน

















 Facilitator: Pawin Puapornpong.>")

