ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
การรักษา Elderly Insomnia
โดย ผู้ช่วยศาสตราจารย์แพทย์หญิงรวิวรรณ นิวาตพันธุ์ ภาควิชาจิตเวชศาสตร์ คณะแพทยศาสตร์ จุฬาลงกรณ์มหาวิทยาลัย

2
อาการนอนไม่หลับ กว่าจะหลับได้ต้องใช้เวลานานมากกว่าปกติ 30-45 นาที
กว่าจะหลับได้ต้องใช้เวลานานมากกว่าปกติ นาที ตื่นกลางดึกหลาย ๆ ครั้งในแต่ละเดือน ตื่นเช้ากว่าปกติและไม่สามารถหลับต่อได้ ตื่นแล้วรู้สึกอ่อนเพลีย ไม่สดชื่นหรือรู้สึกว่านอนหลับได้ไม่เต็มอิ่ม เป็นปัญหาต่อหน้าที่การงานและหน้าที่ทางสังคม

3
ผลกระทบของการนอนไม่หลับ
อ่อนเพลีย ไม่มีแรง Slow reaction time สมาธิการทำงานไม่ดี การทรงตัวไม่ดี หงุดหงิด ซึมเศร้า ความจำแย่ลง ไม่ค่อยมีความสุขในชีวิต ไม่สบายมากขึ้น

4
สาเหตุการนอนไม่หลับในผู้สูงอายุ
โรคทางจิตเวช ที่พบบ่อยที่สุดคือ โรคซึมเศร้า นอกจากนี้ได้แก่ โรควิตกกังวล โรคจิต โรคการปรับตัว (Adjustment disorders), การสูญเสียบุคคลอันเป็นที่รัก โรคทางกาย ผู้สูงอายุมักจะมีโรคทางกายหลายโรค เช่น โรคปวดต่าง ๆ โรคหัวใจ โรคหอบ หรือเคลื่อนไหวลำบาก เส้นเลือดอุดตันในสมอง โรคพาร์กินสัน ทางเดินปัสสาวะอักเสบ โรคต่อมลูกหมากโต
, การสูญเสียบุคคลอันเป็นที่รัก. โรคทางกาย. ผู้สูงอายุมักจะมีโรคทางกายหลายโรค เช่น โรคปวดต่าง ๆ โรคหัวใจ โรคหอบ หรือเคลื่อนไหวลำบาก เส้นเลือดอุดตันในสมอง โรคพาร์กินสัน ทางเดินปัสสาวะอักเสบ โรคต่อมลูกหมากโต.")
5
ปัญหาพฤติกรรมที่ทำให้นอนไม่หลับ
สุขลักษณะการนอนไม่ดี กังวลเรื่องนอนมากไป พยายามที่จะนอนให้พอ ตามเวลาที่คิดว่าควรจะนอน ทำให้เกิดความกังวลและตื่นตัว

6
การซักประวัติ นอนไม่หลับ มานานแค่ไหน อาทิตย์หนึ่งนอนไม่หลับกี่ครั้ง
นอนไม่หลับ มานานแค่ไหน อาทิตย์หนึ่งนอนไม่หลับกี่ครั้ง พฤติกรรมก่อนที่จะมีปัญหาเรื่องนอนไม่หลับ ลักษณะการนอนปัจจุบัน หลับยาก หลับไม่สนิท ตื่นบ่อย หลับต่อยาก ตื่นเร็วกว่าปกติ ตื่นขึ้นมาไม่สดชื่น ลักษณะการนอนก่อนจะมีปัญหา

7
ซักประวัติเพื่อวินิจฉัยชนิดของโรคนอนไม่หลับ จากผู้ป่วยและญาติ
ผลกระทบของการนอนต่อการใช้ชีวิตประวัติวัน ผู้ป่วยรู้สึกเองหรือคนที่นอนด้วยรู้สึก ขากระตุกบ่อย นอนกรนมาก และหยุดหายใจเป็นระยะ รู้สึกว่าปวดขา กระสับกระส่าย นอนไม่ได้ ลุกเดินแล้วดีขึ้น (periodic limb movement disorder, vertless leg syndrome)
")
8
Management elderly insomnia
Insomnia classification Based on the duration of symptoms Transient or acute - few days to 2-4 weeks Chronic - Persisting for more than 1-3 months

9
Pharmacological Therapies
Benzodiazepines Non-benzodiazepine hypnotics Melatonin receptor agonist Antidepressants Antipsychotics antihistamines

10
จะต้องคำนึงถึงประโยชน์และโทษของยา ต่อคุณภาพชีวิตของผู้สูงอายุนอนไม่หลับที่มีผลกระทบต่อการใช้ชีวิตมาก จะได้ประโยชน์จากการรักษามาก

11
จุดประสงค์ของการรักษาด้วยยา
ผู้ป่วยรู้สึกว่าได้นอนหลับสนิทและตื่นขึ้นมาสดชื่น ไม่มีผลข้างเคียงจากยา ง่วงนอน สลึมสลือ ใช้ยาได้นาน ไม่ดื้อยา

12
อุปสรรคที่ทำให้การให้ยาไม่ได้ผล
ความเชื่อของคน ปัญหาสุขภาพของแต่ละบุคคล สรีระเปลี่ยนแปลงเนื่องจากอายุ และโรค

13
Benzodiazepine receptor agonist
lorazepam (10.5 mg - 1 mg), clonazepam (0.25 mg – 1 mg), alprazolam (0.25 mg – 0.5 mg)
, clonazepam (0.25 mg – 1 mg), alprazolam (0.25 mg – 0.5 mg)")
14
Side Effect Drowsiness, dizziness, unsteadiness of gait, rebound insomnia and memory impairment have been reported. Decresore reaction time ดื้อยามากขึ้น หยุดยา ทำให้นอนไม่หลับ อาจมีผลทำให้สุขภาพแย่ลง เสี่ยงต่อการใช้ยาเกินขนาด

15
ประโยชน์ ช่วยให้นอนหลับเร็ว ลดความวิตกกังวล ทำให้กล้ามเนื้อผ่อนคลาย

16
Non Benzodoazepine zolpidem (2.5 – 7.5 mg)
BZI agonist No muscle relaxant Short half life (5 hrs) No daytime sleepiness at dose of 10 mg No rebound insomnia Risk of amnesia
 No daytime sleepiness at dose of 10 mg. No rebound insomnia. Risk of amnesia.")
17
Antidepressants Commonly used for insomnia but are not FDA approved
Trazodone Doxepin (Sinequar) Amitriptyline mirtazapine
 Amitriptyline. mirtazapine.")
18
The Tricyclics Amitriptyline (strong anticholinogic) (10 mg)
Doxepin (Sinequan) (25 mg) Side effects : dry mouth, urinary retention, dizziness, daytime sedation Memory impairment
 (25 mg) Side effects : dry mouth, urinary retention, dizziness, daytime sedation. Memory impairment.")
19
Trazodone Dose range 50-100 mg
The most commonly prescribed agent for treating insomnia cross all classes of medications Major side effects : sedation, dizziness, dry mouth, orthostatic hypotension, priapism (rare) No tolerance dependence and no risk of abuse
 No tolerance dependence and no risk of abuse.")
20
Mertazapine ( mg) Central alpha 2 noradrenergic antagonist , antagonist H1 Side effect, weight gain, increase, appetite, daytime sedation and dizziness No risk abuse

21
Antihistramines Diphenhydramine (Benadryl, Tylenol PM) an Doxylamine (Unisom), hydroxyzine Little evidence to support their use Side effects : dry mouth, urinary retention, blurred vision, dizziness, sedation Cognitive impairment ดื้อยาง่าย

22
Antipsychotic (serequel)
Not approved for insomnia Side effect : fall, metabolic syndrome No data on tolerance

23
How to keep track of your sleep
Daily sleep diary or sleep log Bedtime Falling asleep time Nighttime awakenings Time to get back to sleep Waking up time Getting out of bed time Naps

24
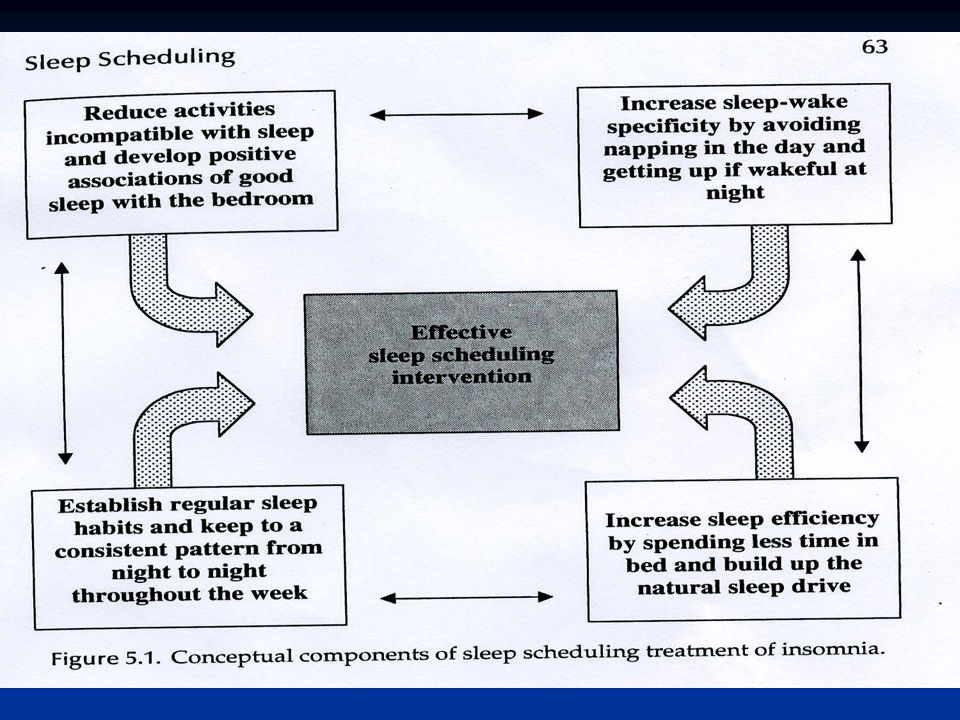
Non-drug treatments Cognitive-behavioral therapy (CBT)
Stimulus control Cognitive therapy Sleep restriction Relaxation training Sleep hygiene

25
Cognitive Behavioral Therapy (CBT) for Insomnia
CBT is as successful as medications in the acute treatment (4-8 weeks) of insomnia It is more effective than medications in the long term Average of 50-60% improvement
 of insomnia. It is more effective than medications in the long term. Average of 50-60% improvement.")
26
Cognitive Therapy Identify beliefs about sleep that are incorrect
Challenge their truthfulness Substitute realistic thoughts

27
Cycle of Persistent Insomnia

28
False beliefs about insomnia
Misconceptions about causes of insomnia “Insomnia is a normal part of aging.” Unrealistic expectations re: sleep needs “I must have 8 hours of sleep each night.” Faulty beliefs about insomnia consequences “Insomnia can make me sick or cause a mental breakdown.” Misattributions of daytime impairments “I’ve had a bad day because of my insomnia.” I can’t have a normal day after a sleepless night.”

29
More common myths about insomnia
Misconceptions about control and predictability of sleep “I can’t predict when I’ll sleep well or badly.” Myths about what behaviors lead to good sleep “When I have trouble getting to sleep, I should stay in bed and try harder.”

30
Sleep Restriction - best if done with a professional
Cut bedtime to the actual amount of time you spend asleep (not in bed), but no less than 4 hours per night No additional sleep is allowed outside these hours Record on your daily sleep log the actual amount of sleep obtained
, but no less than 4 hours per night. No additional sleep is allowed outside these hours. Record on your daily sleep log the actual amount of sleep obtained.")
31
Sleep Restriction (cont’d)
Compute sleep efficiency (total time asleep divided by total time in bed) Based on average of 5 nights’ sleep efficiency, increase sleep time by 15 minutes if efficiency is >85% With elderly, increase sleep time if efficiency >80% and allow 30 minute nap.
 Based on average of 5 nights’ sleep efficiency, increase sleep time by 15 minutes if efficiency is >85% With elderly, increase sleep time if efficiency >80% and allow 30 minute nap.")
32
Stimulus Control - You can do this on your own
Go to bed only when sleepy Use the bed only for sleeping If unable to sleep, move to another room Return to bed only when sleepy Repeat the above as often as necessary Get up at the same time every morning Do not nap

33
Phototherapy- Light Therapy
For DSPS- The patient sits in front of 10,000 lux light for 30 to 40 minutes upon awakening; in addition, room lighting has to be markedly reduced in the evening to achieve the desired results. Response is generally evident after a two to three week period, but frequently requires indefinite treatment to maintain In patients with ASPS, bright light exposure in the evening has been successful in delaying sleep onset.

งานนำเสนอที่คล้ายกัน





 /loʊd/ –to put a large quantity of something into a vehicle or container. –( บรรทุก )>")









>")

 การคมนาคม และการขนส่ง How can I get to the police station ? By taking the white bus. How did she walk ? slowly.>")
 น. พ. นภดล สุชาติ พ. บ. M.P.H.>")

