ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Endocrinology for Comprehensive Exam 2011
Ampha Suthijumroon MD. 6 January 2011

2
Outline DM emergency: Hypoglycemia DKA, HHNS Rx: OHA, insulin
complications Categories risk of DM IFG IGT Thyroid Hyperthyroidism Hypothyroidism Thyroid nodule Hypoglycemia(# DM) Hypercalcemia Dyslipidemia Metabolic syndrome Obesity Adrenal diseases
 Hypercalcemia. Dyslipidemia. Metabolic syndrome. Obesity. Adrenal diseases.")
3
Hypoglycemia in DM Criteria of diagnosis: Whipple's triad
1. Symptoms known caused by hypoglycemia 2. Low plasma glucose at time symptoms occur 3. Reversal or improvement of symptoms or problems when glucose is restored to normal Most healthy adults: maintain fasting glucose levels > 70 mg/dL symptoms of hypoglycemia: glucose falls < 55 mg/dL Hypoglycemia in DM: Plasma glucose <70 mg/dL ADA recommendation. Diabetes Care 2010

4
Pathogenesis of DKA and HHS
Hyperglycemia Glucose utilization Gluconeogenesis Glycogenolysis Glucagon Catecholamines Cortisol Growth hormone Proteolysis Protein synthesis Gluconeogenic substrates ++ Hyperlipidemia Triacylglycerol Absolute insulin deficiency Ketoacidosis lipolysis FFA* to liver Ketogenesis Alkali reserve Relative insulin deficiency Absent or minimal Ketogenesis Hyperosmolarity Glucosuria (osmotic diuresis) Loss of water and electrolytes Dehydration Impaired renal function Decrease Fluid intake HHNS DKA Adapted from Kitabchi A. Diabetes Care 2009;32:
 Loss of water and electrolytes. Dehydration. Impaired renal function. Decrease. Fluid intake. HHNS. DKA. Adapted from Kitabchi A. Diabetes Care 2009;32:")
5
Criteria Diagnosis of DKA
Diabetes Plasma glucose > 250 mg/dL Urine ketone > 3+ ( large ) Ketone Serum ketone > 2+ (moderate) undiluted still positive with 1:2 dilution Total serum ketone > 3 mmol/L Arterial pH < 7.3 Acidosis Serum CO2 < 18 mEq/L Anion gap > 14 mEq/L( >10-12) Adapted from Kitabchi A. Diabetes Care 2009;32:
 Ketone. Serum ketone > 2+ (moderate) undiluted. still positive with 1:2 dilution. Total serum ketone > 3 mmol/L. Arterial pH < 7.3. Acidosis. Serum CO2 < 18 mEq/L. Anion gap > 14 mEq/L( >10-12) Adapted from Kitabchi A. Diabetes Care 2009;32:")
6
Criteria diagnosis of HHNS
Diabetes Plasma glucose >600 mg/dL Ketone Urine ketone – small Serum ketone- small Serum CO > 18 mEq/L Effective serum osmolality >320 mOsm/kg Adapted from Kitabchi A. Diabetes Care 2009;32:

7
DKA HHNS Plasma glucose (mg/dL) > 250 >600 Urine ketone positive
small Serum ketone Serum bicarbonate(mEq/L) <18 - <10 >18 Arterial pH <7.30 >7.30 Anion gap > 10 variable Effective serum osmolality >320 mOsm/kg Mental status Alert to coma Stupor/coma Adapted from Kitabchi A. Diabetes Care 2009;32:
 <18 - <10. >18. Arterial pH. <7.30. >7.30. Anion gap. > 10. variable. Effective serum osmolality. >320 mOsm/kg. Mental status. Alert to coma. Stupor/coma. Adapted from Kitabchi A. Diabetes Care 2009;32:")
8
Management of Patients with DKA
Complete initial evaluation. Start IVF of 0.9% NaCl 1 liter/hr initially IVF Severe hypovolemia Mild dehydration Cardiogenic shock NSS Hemodynamic monitoring Evaluate corrected serum Na High Normal Low 250 - 500 ml/hr BG > 200: change to 5%D/N/2 at 150 250 ml/hr Insulin IV route Uncomplicated DKA SC. route RI 0.1 u/kg bolus IV, RA insulin 0.3 u/kg, 0.2 u/kg 1 hr later, then 0.2 u/kg q 2 hr BG 50 70 mg/dl: double insulin bolus BG > 200: RI to 0.05 0.1 u / kg hr IV Keep BG 150 200, until resolution DKA Check electrolytes, BUN,Cr,glucose q hr patient is able to eat: initiate SC multidose insulin regimen, start at U/kg/day 0.1 u/kg/hr IV infusion or RA insulin 0.1 u/kg SC q 2 hr RI = Regular insulin RA = Rapid acting insulin Adapted from Kitabchi A. Diabetes Care 2009;32:

9
Decreased Glucose Uptake Neurotransmitter Dysfunction
Ominous OCTET Decreased Incretin Effect Decreased Insulin Secretion Increased Lipolysis Islet α-cell Hyperglycemia Increased Glucose Reabsorption Increased Glucagon Secretion Increased HGP Decreased Glucose Uptake Neurotransmitter Dysfunction

10
Anti diabetic drugs Insulin sensitizers: biguanides- metformin
thiazolidinedione- pioglitazone Insulin secretagogues Sulfonylureas- glibenclamide, glipizide, gliclazide Meglitinides- repaglinide GLP-1 analogs- Exenatide, liraglutide, etc. DPP4 inhibitors- Sitagliptin, vildagliptin, etc. Insulins Others: Alpha glucosidase inhibitor- acarbose Amylin analog- Pramlintide SGLT2 inhibitors- Dapaglifozin

11
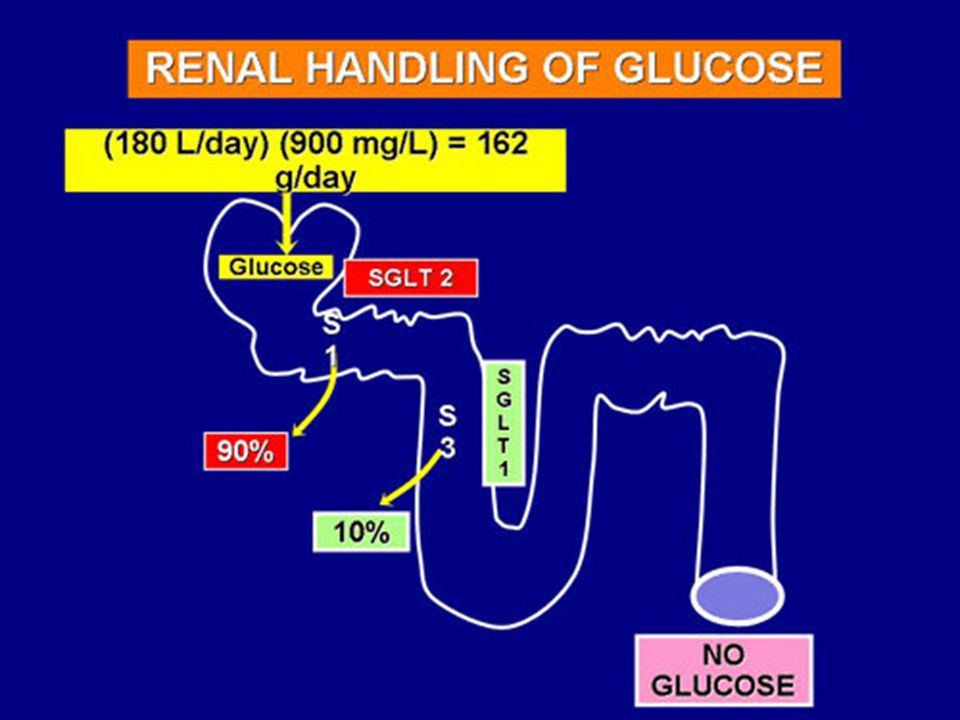
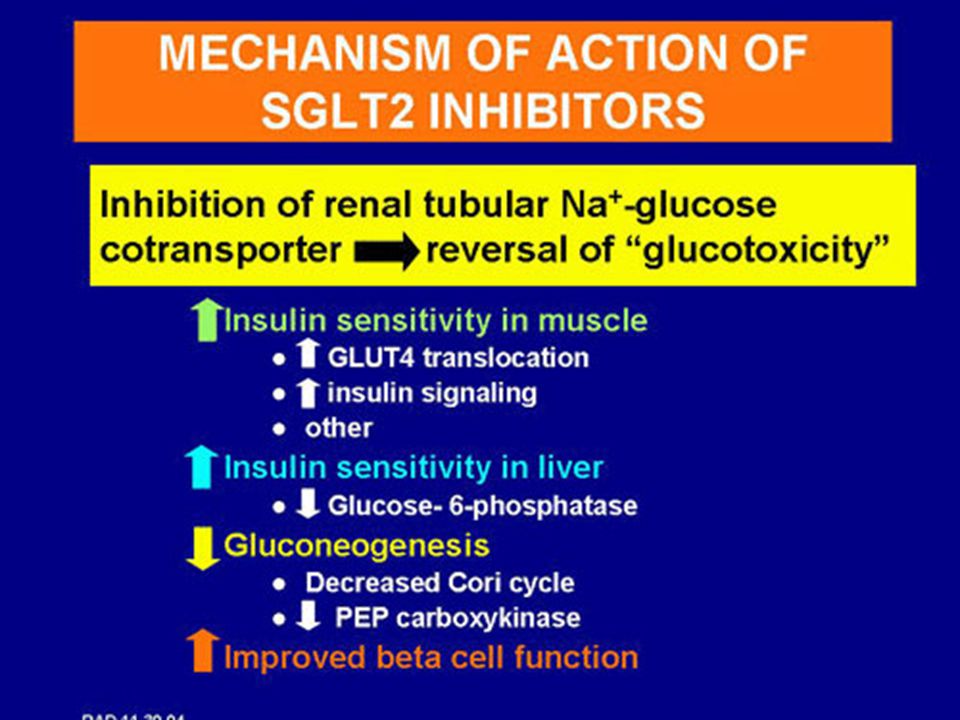
SGLT2 inhibitor

12
Incretins and DPP4 inhibitor
Incretin action Pancreas GLP-1, GIP GI tract Increased insulin release Meal ingestion Cellular glucose uptake Secretion of active GLP-1, GIP β-cell Liver Hepatic glucose output α- cell GLP-1 Suppressed glucose production Suppressed glucagon release DPP 4 inhibitor DPP4 Inactive GLP-1 and GIP

13
Sodium-glucose transporter-2(SGLT2) = “ transporter protein” in Kidneys
 = transporter protein in Kidneys")
14
Glucose in urine Polyuria Urine Urine

17
Diabetic Complications

18
เป้าหมายการควบคุมเบาหวานและปัจจัยเสี่ยงสำหรับผู้ใหญ่
การควบคุม /การปฏิบัติตัว เป้าหมาย การควบคุมเบาหวาน: A1C < 7.0 % (6.5) ระดับไขมันในเลือด: LDL < 100 ( <70* ) มก./ดล. ความดันโลหิต < 130/80 มม.ปรอท น้ำหนักตัว: รอบเอว < 90 (ชาย), < 80 (หญิง) ซม. การสูบบุหรี่ ไม่สูบและหลีกเลี่ยงการรับควันบุหรี่ การออกกำลังกาย ตามคำแนะนำของแพทย์ * ผู้ที่มีโรคหัวใจ แนวทางเวชปฏิบัติสำหรับโรคเบาหวาน พ.ศ (รอการตีพิมพ์)
 ระดับไขมันในเลือด: LDL. < 100 ( <70* ) มก./ดล. ความดันโลหิต. < 130/80 มม.ปรอท. น้ำหนักตัว: รอบเอว. < 90 (ชาย), < 80 (หญิง) ซม. การสูบบุหรี่ ไม่สูบและหลีกเลี่ยงการรับควันบุหรี่ การออกกำลังกาย. ตามคำแนะนำของแพทย์ * ผู้ที่มีโรคหัวใจ. แนวทางเวชปฏิบัติสำหรับโรคเบาหวาน พ.ศ (รอการตีพิมพ์)")
19
ข้อดีของการลดน้ำตาลสะสม (A1C) ช่วยลดความเสี่ยงต่อการเกิดภาวะแทรกซ้อนเรื้อรังของเบาหวาน
16 12 of Complications Relative Risk 8 4 Hemoglobin A1c(%) 6 7 8 9 10 11 12 Average Glucose (mg./dl) 120 150 180 210 240 270 300 UKPDS 33: Lancet 1998; 352, DCCT Study Group. N Engl J Med 329:977, 1993
 Average Glucose. (mg./dl) UKPDS 33: Lancet 1998; 352, DCCT Study Group. N Engl J Med 329:977,")
20
การประเมินผลการรักษาเบาหวาน
12 298 11 269 10 240 9 212 8 183 7 154 6 126 4 65 ระดับน้ำตาลเฉลี่ย(มก./ดล.) Average glucose ระดับน้ำตาลเฉลี่ยสะสม(%) ฮีโมโกบิน เอวันซี (HbA1c or A1C) ค่า A1C น้อยกว่า 7% คุมเบาหวานได้ดี 7-8% คุมเบาหวานได้พอใช้ มากกว่า 8%ขึ้นไป คุมเบาหวานได้ไม่ดี เสี่ยงต่อการเกิดภาวะแทรกซ้อนจากเบาหวาน Adapted from 1. ADA. Diabetes Care 2010:33(Suppl 1);S19 2.Nathan DM, et al. Diabetes care 2008:31;
 Average glucose. ระดับน้ำตาลเฉลี่ยสะสม(%) ฮีโมโกบิน. เอวันซี (HbA1c or A1C) ค่า A1C. น้อยกว่า 7% คุมเบาหวานได้ดี 7-8% คุมเบาหวานได้พอใช้ มากกว่า 8%ขึ้นไป คุมเบาหวานได้ไม่ดี เสี่ยงต่อการเกิดภาวะแทรกซ้อนจากเบาหวาน. Adapted from 1. ADA. Diabetes Care 2010:33(Suppl 1);S19. 2.Nathan DM, et al. Diabetes care 2008:31;")
21
ภาวะแทรกซ้อนเรื้อรังของเบาหวาน
หลอดเลือดแดงเล็ก หลอดเลือดแดงใหญ่ เบาหวานขึ้นตา โรคหัวใจ โรคสมอง ไตเสื่อมจากเบาหวาน โรคหลอดเลือดส่วนปลายตีบ (PAD) ระบบประสาทเสื่อมจากเบาหวาน
 ระบบประสาทเสื่อมจากเบาหวาน.")
22
การตรวจภาวะแทรกซ้อนของโรคเบาหวาน
เบาหวานขึ้นตา โรคไต จากเบาหวาน การตรวจเท้า ผู้เป็นเบาหวานชนิดที่ 1 ครั้งแรก เมื่อเป็นเบาหวานได้ 5 ปี เมื่อเริ่มเป็นโรค ครั้งต่อไป ตามแพทย์นัด ผู้เป็นเบาหวานชนิดที่ 2

23
เกณฑ์การวินิจฉัยโรคเบาหวาน
Criteria of Diagnosis Diabetes Mellitus เกณฑ์การวินิจฉัยโรคเบาหวาน ระดับน้ำตาลปกติ (มก./ดล.) ผู้เสี่ยงต่อโรคเบาหวาน IFG หรือ IGT เป็นโรคเบาหวาน FPG 70-99 2hr PG <140 FPG (IFG) 2hr PG (IGT) FPG >126 2hr PG >200 มีอาการของโรคเบาหวาน และระดับพลาสมากลูโคสเวลาใดก็ตาม >200 IFG = Impaired fasting glucose (ระดับน้ำตาลหลังอดอาหารผิดปกติ) IGT = Impaired glucose tolerance (ความทนของน้ำตาลกลูโคสผิดปกติ) แนวทางเวชปฏิบัติสำหรับโรคเบาหวาน พ.ศ (รอการตีพิมพ์)
 ผู้เสี่ยงต่อโรคเบาหวาน. IFG หรือ IGT. เป็นโรคเบาหวาน. FPG hr PG <140. FPG (IFG) 2hr PG (IGT) FPG >126. 2hr PG >200. มีอาการของโรคเบาหวาน และระดับพลาสมากลูโคสเวลาใดก็ตาม >200. IFG = Impaired fasting glucose (ระดับน้ำตาลหลังอดอาหารผิดปกติ) IGT = Impaired glucose tolerance (ความทนของน้ำตาลกลูโคสผิดปกติ) แนวทางเวชปฏิบัติสำหรับโรคเบาหวาน พ.ศ (รอการตีพิมพ์)")
24
Regulation of Thyroid hormons
24

25
Hypothyroidism: FT4, TSH Anti-TPO( thyroid peroxidase)
25

26
I- Lithium Lugol SSKI Perchlorate MMI,PTU B-blocker T4 T3 Target
Organs Amiodarone PTU high dose B-blocker Steroid 26

27
Antithyroid drug comparision
Factor Propylthiouracil (PTU) Methimazole (MMI) Response time Slower Faster Toxicity Idiosyncracy Hepatitis, vasculitis Dose-related Less common SE Compliance worse better Effect on radioiodine outcome Decrease effect No effect Adapted from Uptodate 17.3,2009 27
 Methimazole. (MMI) Response time. Slower. Faster. Toxicity. Idiosyncracy. Hepatitis, vasculitis. Dose-related. Less common SE. Compliance. worse. better. Effect on radioiodine outcome. Decrease effect. No effect. Adapted from Uptodate 17.3,")
28
Side effect of antithyroid drug
28

29
Hypothyroidism: Laboratory Evaluation
Thyroid hormone Primary hypothyroidism Overt : ↑ TSH , ↓ FT4 Subclinical : ↑ TSH , ↔ FT4 Secondary hypothyroidism ↔ or ↓ TSH , ↓ FT4

30
Laboratory Evaluation
Hypothyroidism: Laboratory Evaluation Laboratory Evaluation Antithyroid peroxidase (anti-TPO) (Antimicrosomal antibodies (AMA)) For diagnosis autoimmune thyroiditis 95% +ve in Hashimoto ‘s thyroiditis
 (Antimicrosomal antibodies (AMA)) For diagnosis autoimmune thyroiditis. 95% +ve in Hashimoto ‘s thyroiditis.")
31
Kronenberg: Williams Textbook of Endocrinology, 11th ed.2008

32
Thyroid Nodules American Thyroid Association (ATA)
Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer THYROID 2009;19(11):
:")
33
American Thyroid Association (ATA) Guidelines Taskforce
on Thyroid Nodules and Differentiated Thyroid Cancer. THYROID 2009;19(11):
:")
34
American Thyroid Association (ATA) Guidelines Taskforce
on Thyroid Nodules and Differentiated Thyroid Cancer. THYROID 2009;19(11):
:")
35
Calciotropic hormone levels
Disease Ca PO4 iPTH 25OHD 1,25(OH)2D Primary hyperparathyroidism N to Malignancy : Solid to N N Myleoma Lymphoma toN Granuloma Vitamin D or 25OHD toxicity 1(OH)D or 1,25(OH)2D toxicity v Pattanaungkul S, Royal Thai Army Medical Journal 52, 1999
2D. Primary hyperparathyroidism. N to. Malignancy : Solid. to N. N. Myleoma. Lymphoma. toN. Granuloma. Vitamin D or 25OHD toxicity. 1(OH)D or 1,25(OH)2D toxicity. v. Pattanaungkul S, Royal Thai Army Medical Journal 52,")
36
Evaluation of patient with hypercalcemia
Harrison’s 17th edition

37
Treatment of Hypercalcemia
Onset of action Duration of action Hydration: NSS Hours During treatment Forced diuresis : NSS + Loop diuretic Calcitonin 2-4 hrs 1-2 days Tachyphylaxis Bisphosphonate 2nd gen: Pamidronate 1-2 days 2-4 wks 3rd gen: Zolendronate 4-6 wks Glucocorticoids Days Days, weeks Dialysis (HD or PD) During treatment – 2 days Harrison’s 17th edition
 During treatment – 2 days. Harrison’s 17th edition.")
38
Treatment of Hypercalcemia
Williams textbook of endocrinology, 11th edition,2008

39
Bisphosphonates in HHM
Creatinine Clearance Drug/Dose CrCl> 60ml/min Pamidronate 90 mg over 3 hr Zoledronate 4 mg over 15 min CrCl< 60ml/min Zoledronate : ruduced dose CrCl< 30ml/min Pamidronate 90 mg over 6 hr Zoledronate : not recommended Kidney International doi: /ki

40
Evaluation of hypocalcemia

41
Treatment of Hypocalcemia
Depends upon: severity , underlying cause, rate of decrease of serum calcium Intravenous calcium Oral calcium supplementation Vitamin D

42
% Elemental calcium in calcium medications
Form of Ca 40 Calcium carbonate 9 Calcium gluconate 13 Calcium lactate 21 Calcium citrate 27 Calcium chloride 23-40 Calcium phosphate Pattanaungkul S, Royal Thai Army Medical Journal 52, 1999

43
Vitamin D supplement Vitamin D Calcitriol Vitamin D analogues
UpToDate 18.1, 2010

44
Vitamin D form Name Dose Dose/day Vitamin D2 20,000 IU 40,000-100,000
One alpha (1(OH)D3) 0.25 µg, 1 µg µg/day Alpha D3 (1(OH)D3) 0.25 µg, 1 µg Bon-one (1(OH)D3) 0.25 µg, 0.5 µg Rocaltriol (1,25(OH)2D3) 0.25 µg Pattanaungkul S, Royal Thai Army Medical Journal 52, 1999
D3) 0.25 µg, 1 µg µg/day. Alpha D3 (1(OH)D3) 0.25 µg, 1 µg. Bon-one (1(OH)D3) 0.25 µg, 0.5 µg. Rocaltriol (1,25(OH)2D3) 0.25 µg. Pattanaungkul S, Royal Thai Army Medical Journal 52,")
45
Outline DM emergency: Hypoglycemia DKA, HHNS Rx: OHA, insulin
complications Categories risk of DM IFG IGT Thyroid Hyperthyroidism Hypothyroidism Thyroid nodule Hypoglycemia(# DM) Hypercalcemia Dyslipidemia Metabolic syndrome Obesity Adrenal diseases
 Hypercalcemia. Dyslipidemia. Metabolic syndrome. Obesity. Adrenal diseases.")
46
Role of LDL in Inflammation
LDL Readily Enter the Artery Wall Where They May be Modified Vessel Lumen LDL Endothelium LDL Oxidation of Lipids and ApoB Hydrolysis of Phosphatidylcholine to Lysophosphatidylcholine Aggregation Other Chemical Modifications Role of LDL in inflammation LDL readily enters the artery wall by crossing the endothelial membrane. Once in the arterial wall, if LDL accumulates, it is subject to a variety of modifications. The best known of these is oxidation, both of the lipids and of the apo B. LDL is also subject to aggregation, and its phospholipids are subject to hydrolysis by phospholipases to form lysophosphatidylcholine. Several other chemical modifications have also been reported. The net effect of these changes is the production of a variety of modified LDL particles, and the evidence is now very strong that these modified LDL particles are proinflammatory. Reference: Steinberg D, Parthasarathy S, Carew TE, Khoo JC, Witztum JL. Beyond cholesterol: modifications of low-density lipoprotein that increase its atherogenicity. N Engl J Med 1989;320: Modified LDL Modified LDL are Proinflammatory Intima Adapted from Steinberg D et al. N Engl J Med 1989;320:

47
LDL is Proinflammatory
Monocyte Vessel Lumen LDL Adhesion Molecules Endothelium MCP-1 LDL Intima Modified LDL Macrophages and foam cells express growth factors and proteinases Once the macrophage has taken up lipid and been converted into a foam cell, all the cell types necessary for the inflammatory process that leads to atherosclerosis are present. Macrophages and foam cells produce not only cytokines but also a variety of growth factors that lead to cell proliferation and matrix production, and metalloproteinases that lead to matrix degeneration. Thus, macrophages and foam cells both contribute to lesion growth and may contribute to instability and thrombotic events. Reference: Ross R. Atherosclerosis--an inflammatory disease. N Engl J Med 1999;340: Cytokines Growth Factors Metalloproteinases Macrophage Cell Proliferation Matrix Degradation Foam Cell Adapted from Ross R. N Engl J Med 1999;340:

48
Remnants of VLDL and Chylomicrons are also Proinflammatory
Vessel Lumen Monocyte Remnant Lipoproteins Adhesion Molecules Endothelium MCP-1 Remnants Intima Modified Remnants The remnants of VLDL and chylomicrons are also pro-inflammatory VLDL remnants and chylomicron remnants behave in much the same way as LDL. They enter the subendothelial space, where they become modified, and the modified remnants stimulate MCP-1, promote the differentiation of monocytes into macrophages, and are taken up by the macrophages to form foam cells. Like LDL, the remnant lipoproteins are proinflammatory and proatherogenic. References: Doi H, Kugiyama K, Oka H, Sugiyama S, Ogata N, Koide SI, Nakamura SI, Yasue H. Remnant lipoproteins induce proatherothrombogenic molecules in endothelial cells through a redox-sensitive mechanism. Circulation 2000;102: Cytokines Growth Factors Metalloproteinases Macrophage Cell Proliferation Matrix Degradation Foam Cell Adapted from Doi H et al. Circulation 2000;102:

49
New Paradigm of Atherothrombosis
healthy subclinical symptomatic Threshold Decades Years-Months Months-Days Intima Media Plaque Thrombus Lumen Unstable angina Unstable plaque no narrowing Difficult to diagnose (IVUS, MRI) Frequent MI with sudden death Easy to prevent More recently, atherogenesis has been revealed as a complex process and is preceded and accompanied by inflammation. The endothelium responds to damage by inducing a protective response, eventually leading to the formation of the atherosclerotic plaque. Over time, the plaque may grow or reduce in size, and may or may not encroach into the lumen of the artery. The clinical outcome often depends on the stability of the plaque.1 The less stable the plaque, the more susceptible it is to erosion or rupture. Both erosion and rupture can lead to thrombus formation on the site of the plaque and vessel occlusion, culminating in unstable angina or myocardial infarction.1 Treatment with statins, in addition to dietary and lifestyle changes, may result in regression of atherosclerotic plaques. Reference 1. Ross R. Nature 1993:362:801–809.
 Frequent MI with sudden death. Easy to prevent. More recently, atherogenesis has been revealed as a complex process and is preceded and accompanied by inflammation. The endothelium responds to damage by inducing a protective response, eventually leading to the formation of the atherosclerotic plaque. Over time, the plaque may grow or reduce in size, and may or may not encroach into the lumen of the artery. The clinical outcome often depends on the stability of the plaque.1 The less stable the plaque, the more susceptible it is to erosion or rupture. Both erosion and rupture can lead to thrombus formation on the site of the plaque and vessel occlusion, culminating in unstable angina or myocardial infarction.1 Treatment with statins, in addition to dietary and lifestyle changes, may result in regression of atherosclerotic plaques. Reference. 1. Ross R. Nature 1993:362:801–809.")
50
NCEP ATP III: LDL-C Goals (2004 proposed modifications)
High Risk CHD or CHD risk equivalents (10-yr risk >20%) LDL-C level 100 - 160 - 130 - 190 - Lower Risk < 2 risk factors Moderately High Risk ≥ 2 risk factors (10-yr risk 10-20%) goal 160 mg/dL 130 70 - 100 or optional 70 mg/dL* Moderate Risk (10-yr risk <10%) 100 mg/dL* Based on recent clinical trial evidence, an NCEP report1 has been published recommending tighter control of cholesterol management. The trials support an LDL-C goal of <100 mg/dL in high-risk patients, and the inclusion of diabetes in the high-risk category. All patients with CHD or CHD risk equivalents are at high-risk. Therapeutic lifestyle changes (TLC) remain an essential part of clinical management. In patients at high risk (CHD and CHD risk equivalents, 10-year risk >20%), the recommended LDL-C goal is <100 mg/dL, but when risk is very high, an LDL-C goal of <70 mg/dL (1.8 mmol/dL) is a proposed therapeutic option. Patients at very high risk are those with established CVD plus: multiple major risk factors (especially diabetes); severe and poorly controlled risk factors (especially continued cigarette smoking); multiple risk factors of the metabolic syndrome and patients with acute coronary syndrome. The recommended point at which TLC should be initiated is an LDL-C level of 100 mg/dL (2.6 mmol/L). The guidelines recommend that drug therapy be considered in this category simultaneously with TLC in persons whose LDL-C levels are 100 mg/dL (2.6 mmol/L). In patients at moderately high risk (2 risk factors and 10-year CHD risk of 10–20%) the guidelines recommend that TLC are initiated at LDL-C levels of 130 mg/dL (3.4 mmol/L), with the aim of <130 mg/dL (3.4 mmol/L), but an LDL-C goal of <100 mg/dL (2.6 mmol/L) is a therapeutic option based on clinical trial evidence. This also applies to patients with a baseline LDL-C of mg/dL. Drug therapy should be considered if LDL-C levels remain 130 mg/dL (3.4 mmol/L), after 3 months of TLC. In patients at moderate risk (2 risk factors and 10-year CHD risk of <10%) the guidelines recommend that TLC are initiated at LDL-C levels of 130 mg/dL (3.4 mmol/L), with the aim of <130 mg/dL (3.4 mmol/L). In this group drug therapy should be considered at LDL-C levels 160 mg/dL (4.1 mmol/L). In individuals at lower risk (<2 risk factors) and whose LDL-C levels are 160 mg/dL (4.1 mmol/L), TLC are recommended. Drug therapy should be considered when LDL-C levels are 190 mg/dL (5 mmol/L) despite TLC, and is optional depending on clinical judgement at LDL-C levels of 160–189 mg/dL (4.1-5 mmol/L). The goal for LDL-C in this risk category is <160 mg/dL (4.1 mmol/L). When LDL-C lowering drug therapy is employed in high-risk or moderately high-risk patients, it is advised that intensity of therapy be sufficient to achieve at least a 30% to 40% reduction in LDL-C levels. Moreover, any person at high risk or moderately high risk who has life-style related risk factors (eg obesity, physical inactivity, elevated TG, low HDL-C or the metabolic syndrome) is a candidate for TLC to modify these risk factors regardless of LDL-C level. Reference 1. Grundy SM, Cleeman JI, Merz NB et al. Circulation 2004;110:227–239. Existing LDL-C goals Proposed LDL-C goals *Therapeutic option Adapted from Grundy S, et al. Circulation 2004;110:
 LDL-C level Lower Risk. < 2 risk factors. Moderately High Risk. ≥ 2 risk factors. (10-yr risk 10-20%) goal mg/dL or optional. 70 mg/dL* Moderate Risk. (10-yr risk <10%) 100 mg/dL* Based on recent clinical trial evidence, an NCEP report1 has been published recommending tighter control of cholesterol management. The trials support an LDL-C goal of <100 mg/dL in high-risk patients, and the inclusion of diabetes in the high-risk category. All patients with CHD or CHD risk equivalents are at high-risk. Therapeutic lifestyle changes (TLC) remain an essential part of clinical management. In patients at high risk (CHD and CHD risk equivalents, 10-year risk >20%), the recommended LDL-C goal is <100 mg/dL, but when risk is very high, an LDL-C goal of <70 mg/dL (1.8 mmol/dL) is a proposed therapeutic option. Patients at very high risk are those with established CVD plus: multiple major risk factors (especially diabetes); severe and poorly controlled risk factors (especially continued cigarette smoking); multiple risk factors of the metabolic syndrome and patients with acute coronary syndrome. The recommended point at which TLC should be initiated is an LDL-C level of 100 mg/dL (2.6 mmol/L). The guidelines recommend that drug therapy be considered in this category simultaneously with TLC in persons whose LDL-C levels are 100 mg/dL (2.6 mmol/L). In patients at moderately high risk (2 risk factors and 10-year CHD risk of 10–20%) the guidelines recommend that TLC are initiated at LDL-C levels of 130 mg/dL (3.4 mmol/L), with the aim of <130 mg/dL (3.4 mmol/L), but an LDL-C goal of <100 mg/dL (2.6 mmol/L) is a therapeutic option based on clinical trial evidence. This also applies to patients with a baseline LDL-C of mg/dL. Drug therapy should be considered if LDL-C levels remain 130 mg/dL (3.4 mmol/L), after 3 months of TLC. In patients at moderate risk (2 risk factors and 10-year CHD risk of <10%) the guidelines recommend that TLC are initiated at LDL-C levels of 130 mg/dL (3.4 mmol/L), with the aim of <130 mg/dL (3.4 mmol/L). In this group drug therapy should be considered at LDL-C levels 160 mg/dL (4.1 mmol/L). In individuals at lower risk (<2 risk factors) and whose LDL-C levels are 160 mg/dL (4.1 mmol/L), TLC are recommended. Drug therapy should be considered when LDL-C levels are 190 mg/dL (5 mmol/L) despite TLC, and is optional depending on clinical judgement at LDL-C levels of 160–189 mg/dL (4.1-5 mmol/L). The goal for LDL-C in this risk category is <160 mg/dL (4.1 mmol/L). When LDL-C lowering drug therapy is employed in high-risk or moderately high-risk patients, it is advised that intensity of therapy be sufficient to achieve at least a 30% to 40% reduction in LDL-C levels. Moreover, any person at high risk or moderately high risk who has life-style related risk factors (eg obesity, physical inactivity, elevated TG, low HDL-C or the metabolic syndrome) is a candidate for TLC to modify these risk factors regardless of LDL-C level. Reference. 1. Grundy SM, Cleeman JI, Merz NB et al. Circulation 2004;110:227–239. Existing LDL-C goals. Proposed LDL-C goals. *Therapeutic option. Adapted from Grundy S, et al. Circulation 2004;110:")
51
<100 mg/dL <70 mg/dL Recommended LDL-C treatment goals 2006
Update ATP III Update 2004 <100 mg/dL: Patients with CHD or CHD risk equivalents (10 year risk >20%) <70 mg/dL: Therapeutic option for very high risk patients <100 mg/dL AHA/ACC guidelines for patients with CHD: <100 mg/dL: Goal for all patients with CHD <70 mg/dL: A reasonable goal for all patients with CHD If it is not possible to attain LDL-C <70 mg/dL because of a high baseline LDL-C, it generally is possible to achieve LDL-C reductions of >50% with more intensive LDL-C lowering therapy, including drug combinations <70 mg/dL
 <70 mg/dL: Therapeutic. option for very. high risk patients. <100 mg/dL. AHA/ACC guidelines. for patients with CHD: <100 mg/dL: Goal for all. patients with CHD. <70 mg/dL: A reasonable. goal for all patients. with CHD. If it is not possible to attain LDL-C <70 mg/dL. because of a high baseline LDL-C, it generally is. possible to achieve LDL-C reductions of >50% with more intensive LDL-C lowering therapy, including drug combinations. <70 mg/dL.")
52
Treatment of Dyslipidemia
Nonpharmachologic therapy Dietary treatment Weight loss and exercise therapy Pharmachologic therapy

53
Summary of Major drugs used for Treatment of Dyslipidemia
Mechanism Common Side Effects HMG-CoA reductase inhibitors (statins) ↓Cholesterol synthesis, ↑hepatic LDL receptors, ↓VLDL production Myalgias, arthralgias, ↑ transaminases, dyspepsia Cholesterol absorption inhibitors ↓ Intestinal cholesterol absorption ↑ transaminases Bile acid sequestrants ↑ Bile acid excretion and ↑ LDL receptors Bloating, constipation, ↑ triglycerides Nicotinic acid ↓ VLDL hepatic synthesis Cutaneous flushing, GI upset, ↑ glucose, uric acid, liver function tests Fibric acid derivatives ↑ LPL, ↓ VLDL synthesis Dyspepsia, myalgia, gallstones, Omega 3 fatty acids ↑ TG catabolism Dyspepsia, diarrhea, fishy odor to breath Adapted from Harrison’s Internal Medicine 17th ed., 2007; p 2428
 ↓Cholesterol synthesis, ↑hepatic LDL receptors, ↓VLDL production Myalgias, arthralgias, ↑ transaminases, dyspepsia. Cholesterol absorption inhibitors. ↓ Intestinal cholesterol absorption ↑ transaminases. Bile acid sequestrants. ↑ Bile acid excretion and. ↑ LDL receptors Bloating, constipation, ↑ triglycerides. Nicotinic acid. ↓ VLDL hepatic synthesis. Cutaneous flushing, GI upset, ↑ glucose, uric acid, liver function tests. Fibric acid derivatives. ↑ LPL, ↓ VLDL synthesis Dyspepsia, myalgia, gallstones, Omega 3 fatty acids. ↑ TG catabolism. Dyspepsia, diarrhea, fishy odor to breath. Adapted from Harrison’s Internal Medicine 17th ed., 2007; p")
54
Summary of Major drugs used for treatment of Dyslipidemia
Major Indications Starting Dose Maximal Dose HMG-CoA reductase inhibitors (statins) Elevated LDL-C Lovastatin 20 mg daily 80 mg daily Pravastatin 40 mg q hs 80 mg q hs Simvastatin 20 mg q hs Fluvastatin Atorvastatin 10 mg q hs Rosuvastatin Adapted from Harrison’s Internal Medicine 17th ed., 2007; p 2428
 Elevated LDL-C. Lovastatin. 20 mg daily. 80 mg daily. Pravastatin. 40 mg q hs. 80 mg q hs. Simvastatin. 20 mg q hs. Fluvastatin. Atorvastatin. 10 mg q hs. Rosuvastatin. Adapted from Harrison’s Internal Medicine 17th ed., 2007; p")
55
Summary of Major drugs used for Treatment of Dyslipidemia
Major Indications Starting Dose Maximal Dose Cholesterol absorption inhibitors Ezetimibe Elevated LDL-C 10 mg daily Bile acid sequestrants Cholestyramine 4 g daily 32 g daily Colestipol 5 g daily 40 g daily Colesevelam 3750 mg daily 4375 mg daily Adapted from Harrison’s Internal Medicine 17th ed., 2007; p 2428

56
Summary of Major drugs used for Treatment of Dyslipidemia
Major Indications Starting Dose Maximal Dose Nicotinic acid ↑ LDL-C, ↓ HDL-C, ↑ TG Immediate-release 100 mg tid 1 g tid Sustained-release 250 mg bid 1.5 g bid Extended-release 500 mg q hs 2 g q hs Fibric acid derivatives ↑ TG, ↑ remnants Gemfibrozil 600 mg bid Fenofibrate 145 mg qd Omega 3 fatty acids ↑ TG 3 g daily 6 g daily Adapted from Harrison’s Internal Medicine 17th ed., 2007; p 2428

57
Metabolic Syndrome (โรคอ้วนลงพุง):
กลุ่มปัจจัยเสี่ยงทางหัวใจและเมตะบอลิสม ที่ทำให้เกิดโรคหลอดเลือดหัวใจ และโรคเบาหวาน ( A cluster of cardiometabolic risk factors that significantly increase atherosclerotic cardiovascular disease (& type 2 DM)) NCEP ATP III. Circulation 2002;106:3143 and Alberti K.2006
) NCEP ATP III. Circulation 2002;106:3143. and Alberti K")
58
อ้วนลงพุง (ไขมันในช่องท้องเพิ่มขึ้น)
อ้วนลงพุง (ไขมันในช่องท้องเพิ่มขึ้น) ไขมันบริเวณสะโพกเพิ่มขึ้น Gynoid obesity Android obesity อ้วน (Obesity) = ดัชนีมวลกาย > 25 กก./ตารางเมตร ดัชนีมวลกาย (BMI) = น้ำหนัก (กก.)/ความสูง (เมตร) 2
 ไขมันบริเวณสะโพกเพิ่มขึ้น. Gynoid obesity. Android obesity. อ้วน (Obesity) = ดัชนีมวลกาย > 25 กก./ตารางเมตร. ดัชนีมวลกาย (BMI) = น้ำหนัก (กก.)/ความสูง (เมตร) 2.")
59
IDF 2005 : Metabolic syndrome
Increased waist circumference by ethnic/country specific* plus at least 2 of the followings 1. Triglyceride > 150 mg/dL 2. HDL-C < 40 (men), < 50 mg/dL (women) or on HDL-C Rx 3. SBP > 130 and or DBP > 85 mmHg 4. FPG > 100 mg/dl or IGT or known diabetes *NCEP: M > 102, F > 88 cm. Europids: M > 94, F > 80 cm. Asians: M > 90, F > 80 cm. (except Japanese: M > 85, F > 90 cm.) Adapted from Alberti K. Diabet Med 2006;23:469-80
, < 50 mg/dL (women) or on HDL-C Rx. 3. SBP > 130 and or DBP > 85 mmHg. 4. FPG > 100 mg/dl or IGT or known diabetes. *NCEP: M > 102, F > 88 cm. Europids: M > 94, F > 80 cm. Asians: M > 90, F > 80 cm. (except Japanese: M > 85, F > 90 cm.) Adapted from Alberti K. Diabet Med 2006;23:")
60
วิธีการรักษาองค์ประกอบของ Metabolic Syndrome
โรคอ้วน (obesity) Lifestyle modification ±drug: orlistat ภาวะดื้อต่ออินซูลิน (Insulin resistance and hyperglycemia): insulin sensitizers – metformin, thiazolidinediones ไขมันผิดปกติในเลือด(dyslipidemia): fibrates, statins HDL raising agents – Niacin, CETP inhibitor ความดันโลหิตสูง (elevated BP) : ACEI/ARB, ( CCB )
 Lifestyle modification. ±drug: orlistat. ภาวะดื้อต่ออินซูลิน (Insulin resistance and hyperglycemia): insulin sensitizers – metformin, thiazolidinediones. ไขมันผิดปกติในเลือด(dyslipidemia): fibrates, statins. HDL raising agents – Niacin, CETP inhibitor. ความดันโลหิตสูง (elevated BP) : ACEI/ARB, ( CCB )")
61
ผลการรักษาMetabolic Syndrome ( Diabetes Prevention Program, DPP)
0.75 0.60 0.45 0.30 0.15 0.00 ระยะเวลาที่ศึกษา(ปี) การหายจากMetabolic Syndrome Placebo group (n=490) Metformin group (n=503) Lifestyle group (n=530) 41% 17% Adapted from DPP. Ann Intern Med 2005;142:
 การหายจากMetabolic Syndrome. Placebo group (n=490) Metformin group (n=503) Lifestyle group (n=530) 41% 17% Adapted from DPP. Ann Intern Med 2005;142:")
62
ไขมันใต้ผิวหนัง สูง ความเสี่ยงต่อการเกิดโรคหัวใจ ต่ำ
- น้ำหนักตัวลดลง 5-10% ไขมันในช่องท้องลดลง~ 30 % ( diet, physical activity, drug ) ไขมันในช่องท้อง เลว ระดับไขมันในเลือด ดีขึ้น ไม่ดี ความไวต่ออินซูลิน ดีขึ้น ระดับน้ำตาลในเลือด หลอดเลือดแข็งตัวง่ายขึ้น สารที่เกิดจากการอักเสบ ไม่ดี หลอดเลือดชั้นในทำงานผิดปกติ ดีขึ้น ผอมลง ( เส้นรอบเอว < 90 ซม.) อ้วนกลางลำตัว(เส้นรอบเอว > 90 ซม.) สูง ความเสี่ยงต่อการเกิดโรคหัวใจ ต่ำ
 ไขมันในช่องท้อง. เลว ระดับไขมันในเลือด ดีขึ้น. ไม่ดี ความไวต่ออินซูลิน ดีขึ้น. ระดับน้ำตาลในเลือด. หลอดเลือดแข็งตัวง่ายขึ้น. สารที่เกิดจากการอักเสบ. ไม่ดี หลอดเลือดชั้นในทำงานผิดปกติ ดีขึ้น. ผอมลง. ( เส้นรอบเอว < 90 ซม.) อ้วนกลางลำตัว(เส้นรอบเอว > 90 ซม.) สูง ความเสี่ยงต่อการเกิดโรคหัวใจ ต่ำ.")
63
Outline DM emergency: Hypoglycemia DKA, HHNS Rx: OHA, insulin
complications Categories risk of DM IFG IGT Thyroid Hyperthyroidism Hypothyroidism Thyroid nodule Hypoglycemia(# DM) Hypercalcemia Dyslipidemia Metabolic syndrome Obesity Adrenal diseases
 Hypercalcemia. Dyslipidemia. Metabolic syndrome. Obesity. Adrenal diseases.")
64
The Diagnosis of Cushing’s Syndrome: An Endocrine Society Clinical Practice Guideline
Accessed from on 29/9/2009

65
The Diagnosis of Cushing’s Syndrome: An Endocrine Society Clinical Practice Guideline
Accessed from on 29/9/2009

66
J Clin Endocrinol Metab 93: 3266–3281, 2008
Algorithm for the detection, confirmation, subtype testing, and treatment of primary aldosteronism (PA). We recommend the case detection of PA in patient groups with relatively high prevalence of PA (1| )—these include patients with moderate, severe, or resistant hypertension, spontaneous or diuretic-induced hypokalemia, hypertension with adrenal incidentaloma, or a family history of early onset hypertension or cerebrovascular accident at a young age (<40 years). We recommend use of the plasma aldosterone:renin ratio (ARR) to detect cases of PA in these patient groups (1| ). We recommend that patients with a positive ARR undergo testing, using any of four confirmatory tests, to definitively confirm or exclude the diagnosis (1| ). We recommend that, all patients with PA undergo an adrenal CT scan as the initial study in subtype testing and to exclude adrenocortical carcinoma (1| ). When surgical treatment is practicable and desired by the patient, the distinction between unilateral and bilateral adrenal disease should be made by adrenal venous sampling (AVS) (1| ). We recommend that treatment by unilateral laparoscopic adrenalectomy be offered to patients with AVS-documented unilateral aldosterone-producing adenoma (1| ). If a patient is unable or unwilling to undergo surgery, we recommend medical treatment with an mineralocorticoid receptor (MR) antagonist (1| ) In patients with PA due to bilateral adrenal disease, we recommend medical treatment with an MR antagonist (1| ). *In patients with confirmed PA who have a family history of PA or of strokes at young age (<40 years), or with onset of hypertension earlier than at 20 years of age, we suggest genetic testing for glucocorticoid-remediable aldosteronism (GRA) (2| ). In patients with GRA, we recommend the use of the lowest dose of glucocorticoid receptor (GR) agonist that can normalize blood pressure and serum potassium levels (1| ). J Clin Endocrinol Metab 93: 3266–3281, 2008 66
. We recommend the. case detection of PA in patient groups with relatively high prevalence of PA (1| )—these include patients with moderate, severe, or resistant hypertension, spontaneous or diuretic-induced hypokalemia, hypertension with adrenal incidentaloma, or a family history of. early onset hypertension or cerebrovascular accident at a young age (<40 years). We recommend use of the plasma aldosterone:renin. ratio (ARR) to detect cases of PA in these patient groups (1| ). We recommend that patients with a positive ARR undergo testing, using any of four confirmatory tests, to definitively confirm or exclude the diagnosis (1| ). We recommend that, all patients with. PA undergo an adrenal CT scan as the initial study in subtype testing and to exclude adrenocortical carcinoma (1| ). When. surgical treatment is practicable and desired by the patient, the distinction between unilateral and bilateral adrenal disease should be. made by adrenal venous sampling (AVS) (1| ). We recommend that treatment by unilateral laparoscopic adrenalectomy be. offered to patients with AVS-documented unilateral aldosterone-producing adenoma (1| ). If a patient is unable or unwilling to. undergo surgery, we recommend medical treatment with an mineralocorticoid receptor (MR) antagonist (1| ) In patients with PA. due to bilateral adrenal disease, we recommend medical treatment with an MR antagonist (1| ). *In patients with confirmed PA who have a family history of PA or of strokes at young age (<40 years), or with onset of hypertension. earlier than at 20 years of age, we suggest genetic testing for glucocorticoid-remediable aldosteronism (GRA) (2| ). In patients. with GRA, we recommend the use of the lowest dose of glucocorticoid receptor (GR) agonist that can normalize blood pressure and. serum potassium levels (1| ). J Clin Endocrinol Metab 93: 3266–3281,")
67
Williams Textbook of Endocrinology, 11th ed. 2008

68
Adrenal Incidentaloma
Definition: Adrenal masses are found incidentally when CT or MRI is done for other reasons Importance: Raises two questions to determine degree of evaluation and need for therapy 1) Is it malignant? 2) Is it functioning?
 Is it malignant 2) Is it functioning")
69
Adrenal Incidentaloma
Prevalence 4.4% Causes benign - adrenal adenoma - pheochromocytoma - Cushing ‘ s syndrome - 1ry aldosteronism malignant - metastatic cancers Investigations: - Size of mass - Serum electrolytes - 24 hr urine metanephrine - Overnight 1 mg dexamethasone suppression test

70
Adrenal Adapted from Harrison’ s Principle of Internal Medicine 17 th Ed.(2008) :
 :")
71
Thank you

72
Sites of action of antidiabetic agents
Carbohydrate Stomach -glucosidase inhibitors Gut I Sulphonylureas and meglitinides Glucose G I Adipose tissue I G Insulin G G I G TZDs Pancreas I G I G I Different antidiabetic agents target distinct sites as part of their primary mechanism of action in reducing hyperglycaemia. Sulphonylureas (e.g. glyburide) and meglitinides (e.g. repaglinide) stimulate insulin release from the pancreas. Biguanides (e.g. metformin) mainly suppress hepatic glucose output. -glucosidase inhibitors (e.g. acarbose) delay digestion and absorption of carbohydrates in the gastrointestinal tract. TZDs (e.g. rosiglitazone) decrease IR in adipose tissue, skeletal muscle and liver. In addition, these agents may have a beneficial effect on β-cell function. Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl 1): S32–40. G G I G I I G Muscle G Liver TZDs Biguanides Adapted from Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl 1): S32–40.
 and meglitinides (e.g. repaglinide) stimulate insulin release from the pancreas. Biguanides (e.g. metformin) mainly suppress hepatic glucose output. -glucosidase inhibitors (e.g. acarbose) delay digestion and absorption of carbohydrates in the gastrointestinal tract. TZDs (e.g. rosiglitazone) decrease IR in adipose tissue, skeletal muscle and liver. In addition, these agents may have a beneficial effect on β-cell function. Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl 1): S32–40. G. G. I. G. I. I. G. Muscle. G. Liver. TZDs. Biguanides. Adapted from Kobayashi M. Diabetes Obes Metab 1999; 1 (Suppl 1): S32–40.")
73
DPP4 inhibitor: Gliptin

งานนำเสนอที่คล้ายกัน







>")






 98.08% 100.02% จังหวัด.>")


 MICU 68% CCU 32%>")

>")