ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
เครือข่ายสุขภาพ และ การประเมินผลสัมฤทธิ์
รศ.ดร.นพ.องอาจ วิพุธศิริ เครือข่ายสุขภาพ และ การประเมินผลสัมฤทธิ์ 16th August 2011

2
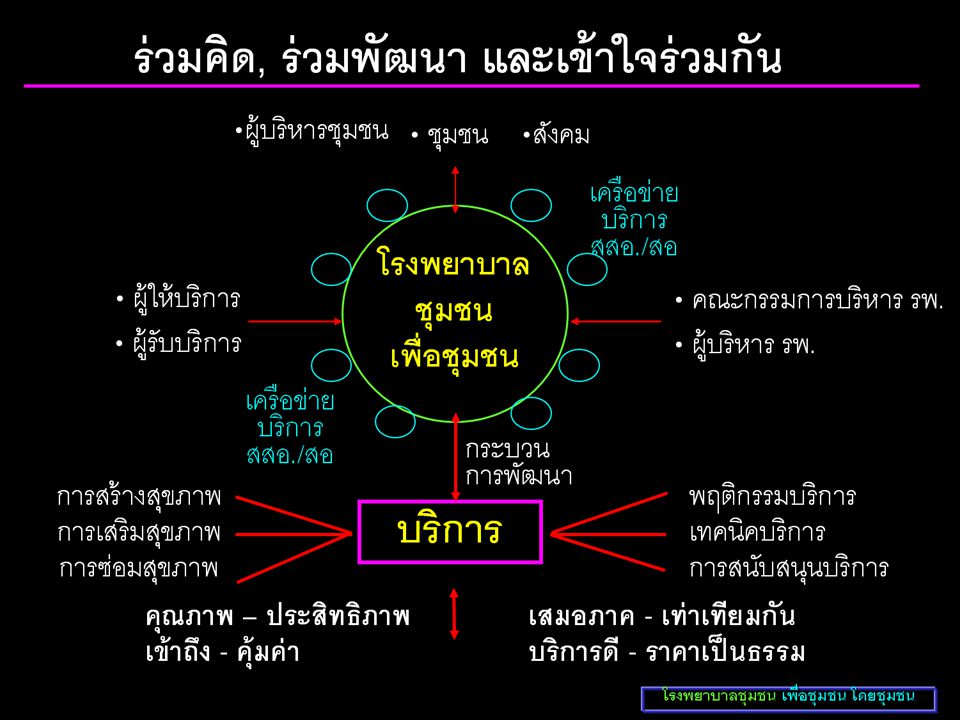
เป็นกระบวนการพัฒนาความสัมพันธ์ระหว่างมนุษย์กับมนุษย์
เครือข่าย (Network) L I N K Learn มีการเรียนรู้ Invest การลงทุน Nurture การฟูมฟักบำรุง Keep relationship การรักษาสัมพันธภาพ รศ.ดร.นพ.องอาจ วิพุธศิริ
 L. I. N. K. Learn. มีการเรียนรู้ Invest. การลงทุน. Nurture. การฟูมฟักบำรุง. Keep. relationship. การรักษาสัมพันธภาพ. รศ.ดร.นพ.องอาจ วิพุธศิริ")
3
Value of networking The value of networking involves more than just connecting with people in your field

4
ประโยชน์ของเครือข่าย
ช่วยให้มีการแลกเปลี่ยนข้อมูลข่าวสาร ทักษะ ความรู้ ประสบการณ์ ช่วยลดการทำงาน และการใช้ทรัพยากรซ้ำซ้อน เชื่อมโยงคนที่อยู่ในระดับต่างกัน วิธีการทำงาน การจัดองค์กร และมีภูมิหลังต่างกันที่ไม่มีโอกาสต่อกัน เข้าด้วยกันได้อย่างมีประสิทธิภาพ ทำให้คนและองค์กรที่ไม่มีความสัมพันธ์กันมาสนใจทำงานในเรื่องเดียวกัน และเผชิญปัญหาร่วมกัน รศ.ดร.นพ.องอาจ วิพุธศิริ

5
ประโยชน์ของเครือข่าย
ทำให้ความต้องการของประชาชนได้รับการสนองตอบจากรัฐ ชี้ให้เห็นปัญหาและประเด็นการพัฒนาที่ซับซ้อนและท่วมท้นในหมู่บ้าน เชื่อมหน่วยงานวิชาการและแหล่งทุนกับผู้ที่ต้องการความช่วยเหลือ ทำให้คนและองค์กรได้รับความช่วยเหลือจากเพื่อน ได้รับกำลังใจ การจูงใจ และการยอมรับ ฯ รศ.ดร.นพ.องอาจ วิพุธศิริ

6
ปัญหาทั่วไปของเครือข่าย
Staykey,1997 1. การขาดวัตถุประสงค์ที่ชัดเจน 2. ความไม่เท่าเทียมกันของสมาชิก 3. การขาดทรัพยากร 4.การจัดการทรัพยากรของเครือข่าย 5.ข้อมูลข่าวสารผิด ๆ ในเครือข่าย

7
ปัญหาทั่วไปของเครือข่าย
Staykey,1997 6.การแข่งขัน ทับซ้อน 7.การแทรกแซงของแหล่งทุน 8.การติดตามและประเมินผล 9.ข้อจำกัดทางการเมือง ฯ รศ.ดร.นพ.องอาจ วิพุธศิริ

8
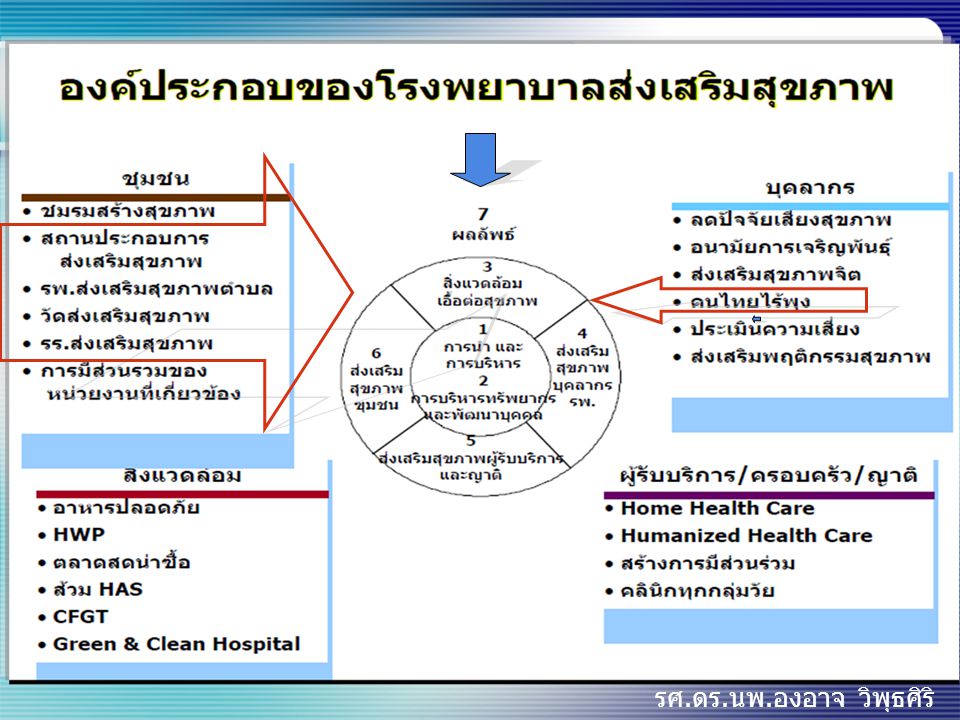
เครือข่ายสุขภาพที่มีประสิทธิภาพ
มี 7 องค์ประกอบ เครือข่ายสุขภาพที่มีประสิทธิภาพ เสริมสร้างซึ่งกันและกัน Complementary relationship รับรู้มุมมองร่วมกัน Common perception เกิดประโยชน์และความสนใจร่วมกัน Mutual interests/benefits ปฏิสัมพันธ์เชิงแลกเปลี่ยน Interaction มีส่วนร่วมของสมาชิกในเครือข่าย All stakeholders participation มีวิสัยทัศน์ร่วมกัน Common vision เครือ ข่าย การพึ่งพิงกัน Interdependence รศ.ดร.นพ.องอาจ วิพุธศิริ

9
Networking will always lead to success
See your goal Understand the obstacles Clear your mind of doubt Create a positive mental picture Embrace the challenge Stay on track Show the world you can do it!!!

10
Specific Measurable Accurate or Approved Realistic Time bound
SMART network purpose Specific Measurable Accurate or Approved Realistic Time bound

11
แนวทางการพัฒนาเครือข่าย สู่ความยั่งยืน
จัดหา ทรัพยากร จัดกิจกรรมอย่างต่อเนื่อง รักษา สัมพันธ์ภาพที่ดี กำหนดแรงระบบจูงใจ ช่วยเหลือและ ช่วยแก้ไขปัญหา สร้างผู้นำรุ่นใหม่ อย่างต่อเนื่อง รศ.ดร.นพ.องอาจ วิพุธศิริ

12
การประเมินผลสัมฤทธิ์
เครือข่ายสุขภาพที่มีประสิทธิภาพ LINK KPI ความพึงพอใจ การบริหารจัดการ ชุมชน รศ.ดร.นพ.องอาจ วิพุธศิริ

13
KPI In hospital In community

14
How Can Health Be Measured?

15
Process of Benefit Assessment

16
Issues in Assessing Benefits for CEA

17
Efficacy Vs Effectiveness Vs Efficiency

18
Intermediate Vs Final Outcome Measures

19
ในรอบทศวรรษที่ผ่านมา
คนไทยอายุ 20 – 29 ปีมีภาวะโรคอ้วน เพิ่มจาก ร้อยละ 2.9 เป็นร้อยละ 21.7 (7.5 เท่า) คนไทยอายุ 40 – 49 ปี อ้วนเพิ่ม 1.7 เท่า ในเด็กประถมมีภาวะโภชนาการเกิน ร้อยละ 13.4เพิ่มขึ้นทุกปี
 คนไทยอายุ 40 – 49 ปี อ้วนเพิ่ม 1.7 เท่า. ในเด็กประถมมีภาวะโภชนาการเกิน ร้อยละ 13.4เพิ่มขึ้นทุกปี")
20
มีผู้รูปร่าง ท่วม ถึง อ้วน
ปัจจุบันประเทศไทย มีผู้รูปร่าง ท่วม ถึง อ้วน สูงถึง 10 ล้านคน

21
เด็กนักเรียนอ้วนระดับประเทศ
ร้อยละ พ.ศ. ที่มา : กองโภชนาการ

22
ระดับอินซูลินในเลือดสูง
เมตะบอลิก ซินโดรม คือกลุ่มของปัจจัยเสี่ยงต่อการเกิดโรคหัวใจและหลอดเลือด ซึ่งเป็นผลจากไขมันในช่องท้องเกิน อ้วน ภาวะดื้อต่อ อินซูลิน ความดันโลหิตสูง ระดับอินซูลินในเลือดสูง ไขมันในเลือดสูง ( HDL, TG) Type 2 เบาหวาน โรคหลอดเลือดและหัวใจ
 Type 2. เบาหวาน. โรคหลอดเลือดและหัวใจ.")
23
Visceral Fat & Waist Circ. บุคลากร กรมอนามัย
ร้อยละ Visceral Fat Normal <100 ตารางซม. รอบเอว ปกติ < 90 ซม.ในเพศชาย <80 ซม.ในเพศหญิง 71.6 62.5 64.4 50.5 49.5 37.5 35.6 28.4 = คน = 436 คน เกินเกณฑ์ Abnormal เส้นรอบเอว Visceral Fat แหล่งข้อมูล : กองโภชนาการ กรมอนามัย 2550

24
“Reform primary health care through networking”
“Deliver the best care, in the best way, on time, every time.” Principles: Access Continuity and Comprehensiveness Quality Care Safety and Reliability

25
Redesign GOALS for primary care
Access Reduce delay for appointments to same day Reduce delays within the appointment x 30% Continuity Increase continuity of care x 90% Increase capacity (panel size) x 10% Quality Outcomes Increase utilization of selected protocols and guidelines Improve interdisciplinary team utilization and function. Safety and Reliability Continuous Measurement of this process and outcomes
 x 10% Quality Outcomes. Increase utilization of selected protocols and guidelines. Improve interdisciplinary team utilization and function. Safety and Reliability. Continuous Measurement of this process and outcomes.")
26
Goals of Primary Care Renewal
Improving frontline access to healthcare Ensuring the continuity and comprehensiveness of care for patients Increasing patient and provider satisfaction Improving the quality of care for patients Increasing the cost-effectiveness of healthcare services. Preserving the doctor-patient relationship as central

27
National/Provincial Primary Care Initiative Objectives
Increase the proportion of residents with ready access to primary care. Provide coordinated 24-hour, 7-day-per-week management of access to appropriate primary care services. Increase the emphasis on health promotion, disease and injury prevention, care of the medically complex patient and care of patients with chronic diseases. Improve coordination and integration with other health care services including secondary, tertiary and long-term care through specialty care linkages to primary care. Facilitate the greater use of multidisciplinary teams to provide comprehensive care.

28
Overloaded & staff shortage

29
“Without access there is no quality.”
Principle: ACCESS “Without access there is no quality.”

30
Principle: Continuity and Comprehensiveness
See your own patients. Don’t make them wait. (Goal: increase capacity x 10%) The most valued qualities: “human relationships” “time to care” the “opportunity to share decisions”.
 The most valued qualities: human relationships time to care the opportunity to share decisions .")
31
Principle: Quality of Care
Quality clinical care is not doctor work, it is team work.” “The best clinical care is not delivered by physician visits alone”

32
Principle: Reliability and Safety
“Safety is connected to Delay”

33
Outcome Measures Access measures: Continuity measures:
Time to third next available appointment Continuity measures: % of patients that see their own doctor Preventive Measures: Screening for Breast, Cervical, and Colon cancers Clinical Measures: hypertension Diabetes Smoking cessation Immunizations

34
Challenges Access Capacity Quality of Care Cultural Competency
Data Quality and Integrity Public Education and Outreach Organizational and Infrastructure Development Networking

35
Improving Patient Care Program

36
Morbidity, Disabilty, Mortality

39
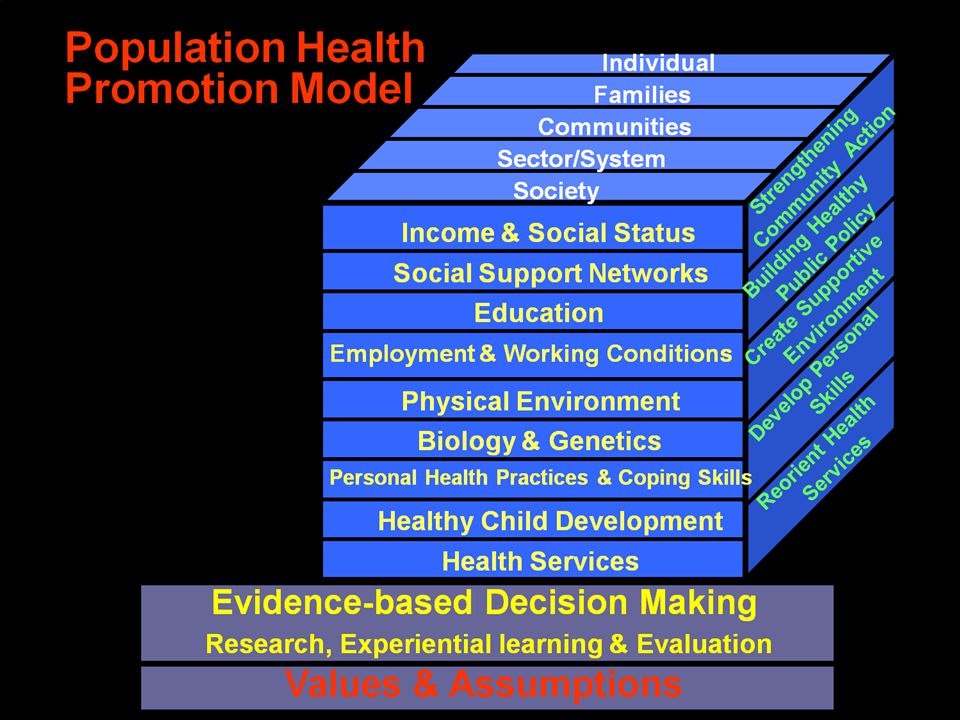
Six principles for second generation objectives:
Social model of health Investment goals Reducing health gaps and social gradients Policy relevant data indices Partnerships and alliances International and sustainable development dimensions

54
Types & Sources of Evidence
Journal literature: Source: Guide to Research Methods: The Evidence Pyramid: <

55
Evidence spectrum Weak Strong No evidence/ case reports
Local needs assessment Meta analysis/ Systematic review/ Evidence-based guidelines Research Best Practices

56
1980 2000 Deaths averted Evidence showed (Research evidence)
Risk factors worse +13% Obesity +3.5% Diabetes +4.8% Less physical activity +4.4% -20,000 -40,000 -60,000 -80,000 1980 2000 Treatments -42% AMI treatments -8% Secondary prevention -11% Heart failure -12% Angina: CABG/PCI -4% Angina: drugs -5% BP treatment -3% Risk factors better -71% Smoking -41% Cholesterol -9% Popul’n BP fall -9% Deprivation -3% Other factors -8% Evidence showed (Research evidence) 68,230 fewer deaths in 2000 Redrawn from Capewell and colleagues
 68,230 fewer. deaths in Redrawn from Capewell and colleagues.")
57
FOUR INTERRELATED THEMES
Ensuring accessibility/equity in health Adding life to years Adding health to life Adding years to life

58
รศ.ดร.นพ.องอาจ วิพุธศิริ
Thank You ! รศ.ดร.นพ.องอาจ วิพุธศิริ

งานนำเสนอที่คล้ายกัน