ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
International Health Policy Program -Thailand 1 การบริหารจัดการงานวิจัยเชิงระบบและเชิงนโยบาย Health system and policy research management Dr Phusit Prakongsai, M.D. Ph.D. International Health Policy Program (IHPP) Ministry of Public Health, Thailand 23 December 2010
 Ministry of Public Health, Thailand 23 December")
2
International Health Policy Program -Thailand 2 การบริหารจัดการงานวิจัยระบบสุขภาพ เป็นเครื่องมือในการขับเคลื่อนและบูรณาการงานวิจัย ซึ่งรวมถึงนักวิจัย และสถาบันวิจัยสุขภาพ เข้าเป็นวิถีของกระบวนการนโยบายและการ ปฏิรูประบบสุขภาพ Commission on Health Research for Development เสนอแนวคิดให้ การวิจัยทางสุขภาพเป็นเครื่องมือมุ่งสู่สุขภาวะที่เท่าเทียมและเป็นธรรม รายงาน Health Research: essential link to equity in development (1990) เกิดแนวคิดการพัฒนา Essential National Health Research (ENHR) Council on Health Research for Development (COHRED) ถ่ายทอดแนวคิด ENHR ไปสู่ประเทศกำลังพัฒนาทั่วโลก แนวร่วมวิจัยนโยบายและระบบสุขภาพ (Alliance for Health Policy Systems Research - AHPSR) in 1996
 เกิดแนวคิดการพัฒนา Essential National Health Research (ENHR) Council on Health Research for Development (COHRED) ถ่ายทอดแนวคิด ENHR ไปสู่ประเทศกำลังพัฒนาทั่วโลก แนวร่วมวิจัยนโยบายและระบบสุขภาพ (Alliance for Health Policy Systems Research - AHPSR) in 1996")
3
International Health Policy Program -Thailand 3 บทบาทและหน้าที่ Essential National Health Research (ENHR) การประสานนโยบายการวิจัย (Stewardship) การจัดลำดับความสำคัญ (prioritization) การสร้างสมรรถนะ (capacity building) การสร้างความรู้ (knowledge generation) การใช้ประโยชน์ความรู้จากงานวิจัย (knowledge management) การระดมทรัพยากร (resource mobilization)
 การประสานนโยบายการวิจัย (Stewardship) การจัดลำดับความสำคัญ (prioritization) การสร้างสมรรถนะ (capacity building) การสร้างความรู้ (knowledge generation) การใช้ประโยชน์ความรู้จากงานวิจัย (knowledge management) การระดมทรัพยากร (resource mobilization)")
4
International Health Policy Program -Thailand 4

5
5 Some basic principles Triangle that moves the mountain Knowledge broker as a bridge between three angles Policy Knowledge Civic groups Knowledgebroker

6
International Health Policy Program -Thailand 6 Political development 1932 Political revolution 1997 Political instability with dominant roles of bureaucrats and military Increasing roles of local businessmen and alliances under their patronages Increasing roles of national businessmen and a need for concrete and achievable policy 2001 general election 1988 An opportunity to submit a draft law to the Parliament for consideration by civic groups Increasing number of middle class and civic movements 1982 People’s Constitution Civic group development 1992 Establishment of HSRI 1996 EU supported Health Care Reform Project 2001 Knowledge development Ayutthaya Project : AR on model of primary care HSRI taskforce on UHC

7
International Health Policy Program -Thailand 7 Link between policy research and field model development Policy research Field model development Financing UHC Provider payment methods Case studies of uninsured Health service organization focusing on primary care Provider payment methods HSRI, IHPP HCR Project Ayutthaya Project HCR Project Research agencies Research areas

8
Conceptual framework of presentation

9
International Health Policy Program -Thailand 9 Source: Analysis of Health and Welfare Survey 2004 (NSO 2004). CSMBS, SHI covers the rich, 52% and 49% belong to Q5 Scheme beneficiaries by income quintiles, 2004 UC scheme covers mostly the poor, 50% belong to Q1+Q2

10
Household OOP for health, % income 1992-2008 Source: Analysis from household socio-economic surveys (SES) in various years 1992-2008, NSO
 in various years , NSO")
11
International Health Policy Program -Thailand 11 Incidence of catastrophic health expenditure in Thailand 2000-2006

12
Kakwani indexes of health care finance and share of health care finance in Thailand from 2000 to 2006 Type of health payments Kakwani indexesShare of health care finance (%) * 20002002200420062000200220042006 Out of pocket payments-0.150-0.076 -0.04533.727.926.423.2 Direct tax0.3910.4160.4420.36218.018.820.8 24.5 Indirect tax-0.096-0.069-0.043-0.08333.438.237.135.2 Premium Insurance-0.362-0.391-0.323Na9.69.28.99.2 SHI contribution0.1650.1120.105Na5.35.96.87.9 Premium insurance & SHI contributionNa -0.049na 17.1% Overall Kakwani index-0.00350.03740.06300.0406100.0
 * Out of pocket payments Direct tax Indirect tax Premium Insurance Na SHI contribution Na Premium insurance & SHI contributionNa na 17.1% Overall Kakwani index")
13
International Health Policy Program -Thailand 13 Equity in utilization: Concentration Index OP service by levels: 2001 to 2007 Facility levels200120032004200520062007 Health centers-0.294-0.365 -0.345-0.380-0.267-0.292 District hospitals-0.270-0.320 -0.285-0.300-0.256-0.246 Provincial and regional hospitals-0.037-0.080 -0.119-0.1000.0280.013 Private hospitals0.4310.348 0.3890.3720.5160.528 Overall-0.090-0.139 -0.163-0.177-0.054-0.041 13 Note: CI range from -1 to + 1. Minus 1 (plus 1 ) means in favour of the poor (rich), or the poor (rich) disproportionately use more services than the rich (poor).
 means in favour of the poor (rich), or the poor (rich) disproportionately use more services than the rich (poor)..")
14
International Health Policy Program -Thailand 14 Equity in utilization: Concentration Index IP service by levels: 2001 to 2007 Types of health facilities200120032004200520062007 Community hospitals-0.316-0.293 -0.294-0.266-0.242-0.293 Provincial and regional hospitals -0.069-0.138 -0.114-0.156-0.049-0.114 Private hospitals0.3200.309 0.2540.3660.3980.464 Overall-0.079-0.121-0.127-0.114-0.051-0.080 14

15
Equity in budget subsidies: BIA, (2001-2007)
")
16
Health service delivery: Better coverage of essential vaccines, ARV and condom use Compulsory licensing Include ART in UC package Generic production of triple ART Percentage of female sex worker consistently use condom when having sex with general client in the past 1 month, 1995 – 2007

17
International Health Policy Program -Thailand 17 Increase access to particular services

18
18 More geographical access to open-heart surgery between 2004 – 2007 but don’t know whether they were the rich or the poor

19
Inequity in quality and patterns of health service provision: Percentage of caesarian section to total deliveries by health insurance schemes Source: Electronic claim database of inpatients from National Health Security Office, 2004-2006 (N=13,232,393 hospital admissions)
")
20
Inequity in quality and patterns of health service provision: Propensity of receiving single source antiplatelets clopidogrel, cilostazol: 6 regional hospitals

21
Inefficiency of the Thai health care system: CSBMS expenditure from 1989 to 2008, current year price Note: Expenditure for 2008 is extrapolated from 6 months actual spending Source: Ministry of Finance, Comptroller Generals Department, various years

22
Current situation and challenges of human resources for health in Thailand Thailand Source: World Development Indicator 2002 and World Health Report 2006

23
Inequity in geographical distribution of Health workforce in 2007 Physicians 800-3,305 3,306-6,274 6,245-9,272 9,243-12,300 Pharmacists 4,600-8,432 8,433-12,274 12,275-16,115 16,116-19,956 Nurses 280 - 652 653 - 904 905 - 1,156 1,157 – 1,408 Dentists 5,500-15,143 15,144-25,767 25,768-36,390 36,391-47,011

24
จำนวนปีสุขภาวะที่สูญเสียของประชากรไทยตามกลุ่มของสาเหตุ ระหว่างพ.ศ. 2542 และพ.ศ. 2547 เพศชาย เพศหญิง

25
จำนวนปีสุขภาวะที่สูญเสียจากภาระโรค พ.ศ. 2542 และ 2547 จำแนกตามกลุ่มอายุ เพศชาย เพศหญิง

26
ปัจจัยเสี่ยงและจำนวนปีสุขภาวะที่สูญเสียจากภาระโรคของประชากร ไทย พ.ศ. 2542 และ 2547 ที่มา โครงการศึกษาภาระโรคและปัจจัยเสี่ยงของประเทศไทย พ.ศ. 2547

27
แนวโน้มการสูบบุหรี่และการดื่มสุราของประชากรไทย แหล่งข้อมูล สอส. 2544, 2546, 2549

28
ความชุกของการดื่มสุราในประชากรอายุ 15 ปีขึ้นไป แหล่งข้อมูล สอส. 2544, 2546 และ 2549

29
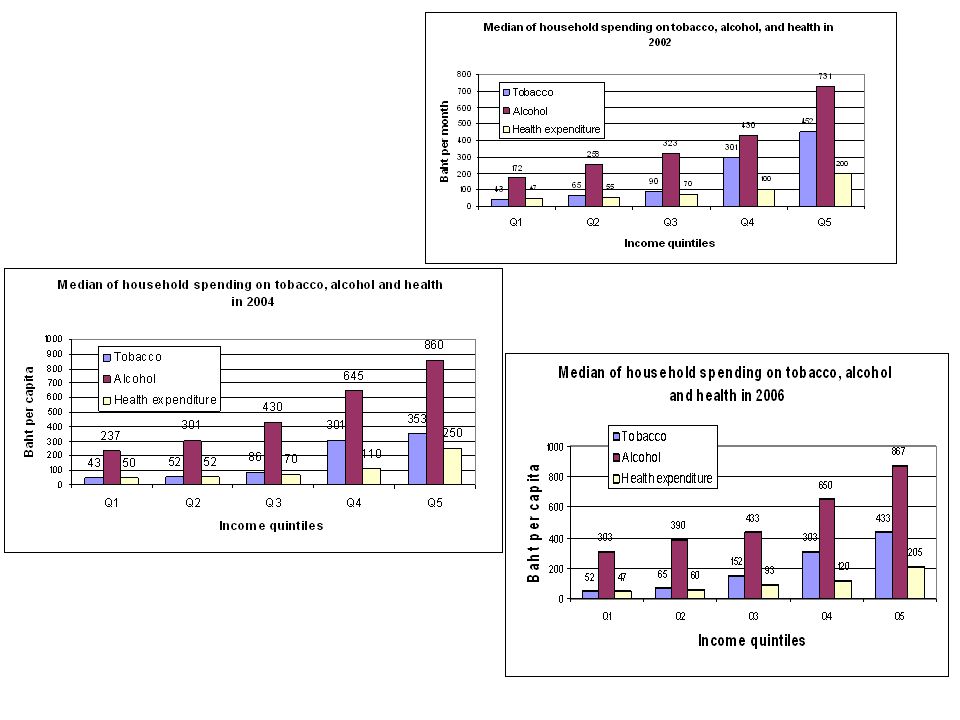
Household consumption: tobacco, alcohol and health Median household expenditure per month Sources: Analyses from 2006 SES

31
Child mortality in Thailand from various sources of surveys Source: Hill et al. Int J Epidemiol 2007 (with updates)
.")
32
RR = 2.8 (95% CI 2.5-3.0) RR = 1.8 (95% CI 1.6-2.0) 55% (39%-68%) reduction Error bars are 95% CIs Source: Vapattanawong P, Hogan MC, Hanvoravongchai P, Gakidou E, Vos T, Lopez AD, Lim SS. Reductions in child mortality levels and inequalities in Thailand: analysis of two censuses. Lancet 2007; 369:850-855 Child mortality by quintile of household economic status from 1990 and 2000 census

33
How equity and efficiency were achieved? 1. Long term financial sustainability 2. Technical efficiency, rational use of services at primary health care Functioning primary health care at district level, wide geographical coverage of services, referral back up to tertiary care where needed, close-to-client services with minimum traveling cost In-feasible for informal sector (equally 25% belong to Q1 and Q2) to adopt contributory scheme 1. Equity in financial contribution Tax financed scheme, adequate financing of primary healthcare 2. Minimum catastrophic health expenditure 3. Minimum level of impoverishment Breadth and depth coverage, comprehensive benefit package, free at point of services 4. Equity in use of services 5. Equity in government subsidies Provider payment method: capitation contract model and global budget + DRG EQUITY GOALS EFFICIENCY GOALS
 to adopt contributory scheme 1. Equity in financial contribution Tax financed scheme, adequate financing of primary healthcare 2. Minimum catastrophic health expenditure 3. Minimum level of impoverishment Breadth and depth coverage, comprehensive benefit package, free at point of services 4. Equity in use of services 5. Equity in government subsidies Provider payment method: capitation contract model and global budget + DRG EQUITY GOALS EFFICIENCY GOALS.")
34
International Health Policy Program -Thailand 34 Key challenges and unfinished agenda – BOD challenges Increased diseases burden from chronic NCD Demographic changes in Thailand Little success in controlling traffic injuries Revitalizing HIV prevention in the light of universal ART – Health systems capacity to cope with Increased workload with very strained health workforces Decentralization context –threats and opportunities, don’t’ move fast Public private dialogues, better trust and collaboration Medical tourism and internal brain drains – Long term financial sustainability Universal access to renal replacement therapy-heavy fiscal pressure, cost ineffective, >4X GNI per QALY, but adopted due to catastrophic and inequity across 3 schemes Second and third lines ARV Medical technology advancement-main drivers in OECD

งานนำเสนอที่คล้ายกัน