ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Interesting case พ.ต. ประสาร เหมือนพงษ์
หน่วยโรคระบบหายใจและกุมารเวชวิกฤต รพ.พระมงกุฎเกล้า

2
Case ผู้ป่วยเด็กหญิงไทย อายุ 7 ปี ภูมิลำเนา จ. สุพรรณบุรี
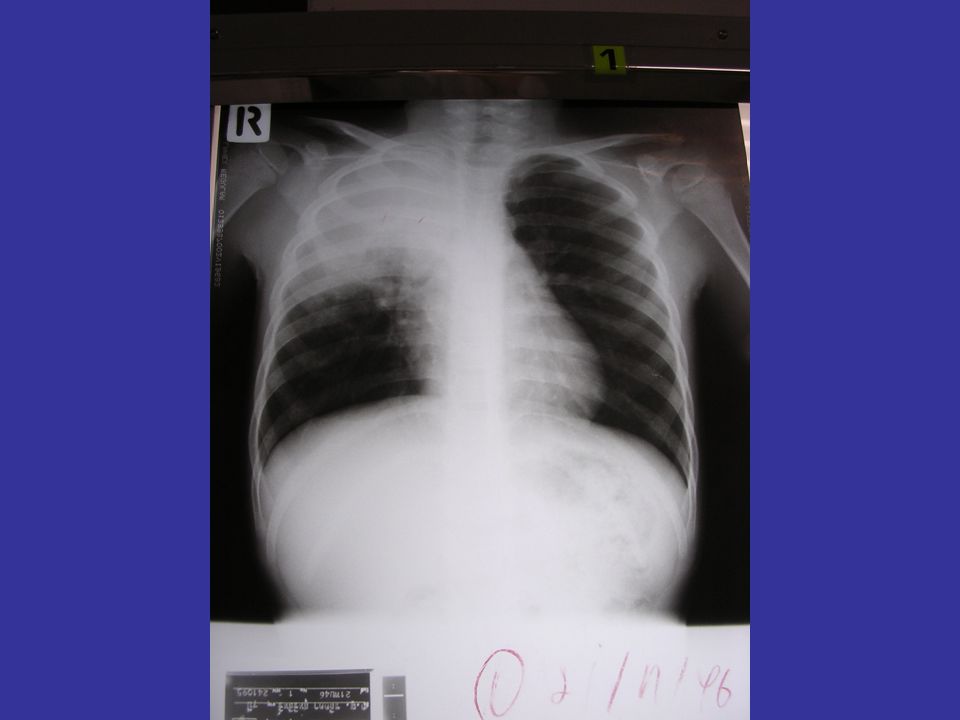
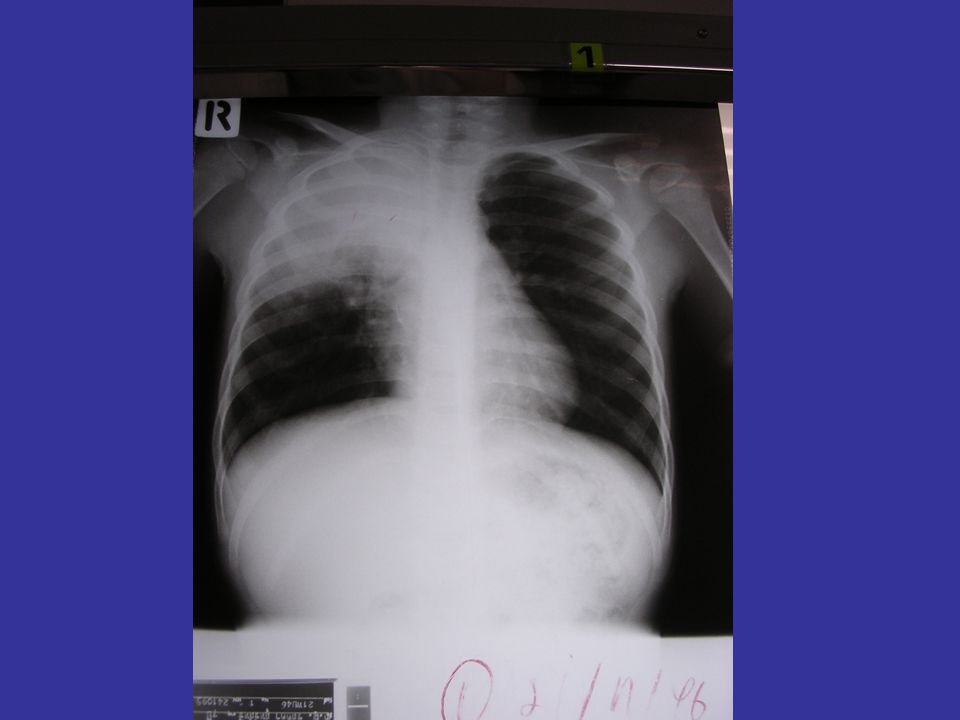
CC : ไอเป็นเลือดสด 1 เดือน ก่อนมารพ. PI : -10 เดือน ก่อนมารพ. มีไข้ต่ำๆ ไอมีเสมหะ ไปรับยาที่อนามัยมากินหลายครั้ง แต่อาการไม่ดีขึ้น - 4 เดือน ก่อนมารพ. มีไข้สูง เหนื่อย ไอมีเสมหะปนเลือดเล็กน้อย จึงไปที่รพ.เจ้าพระยายมราช CXR พบ opacity RUL ,PPD negative , Gastric content for AFB × 3 วันและC/S for TB negative จึงได้ทำการรักษาแบบ pneumonia ได้ให้ Ampicillin + Erythromycin 8 วัน อาการดีขึ้น จึงให้กลับบ้าน

3
- 2 เดือน ก่อน ไป F/U ตามนัดที่ร. พ
- 2 เดือน ก่อน ไป F/U ตามนัดที่ร.พ.เดิม อาการปกติดี แต่ CXR ไม่ดีขึ้น จึง Admit อีกครั้งเพื่อ work up พบว่า PPD = 12×16 mm , gastric content for AFB × 3 วัน negative จึง try treatment ด้วย Anti – TB drug ( IRZE ) แล้วให้กลับบ้าน
 แล้วให้กลับบ้าน.")
4
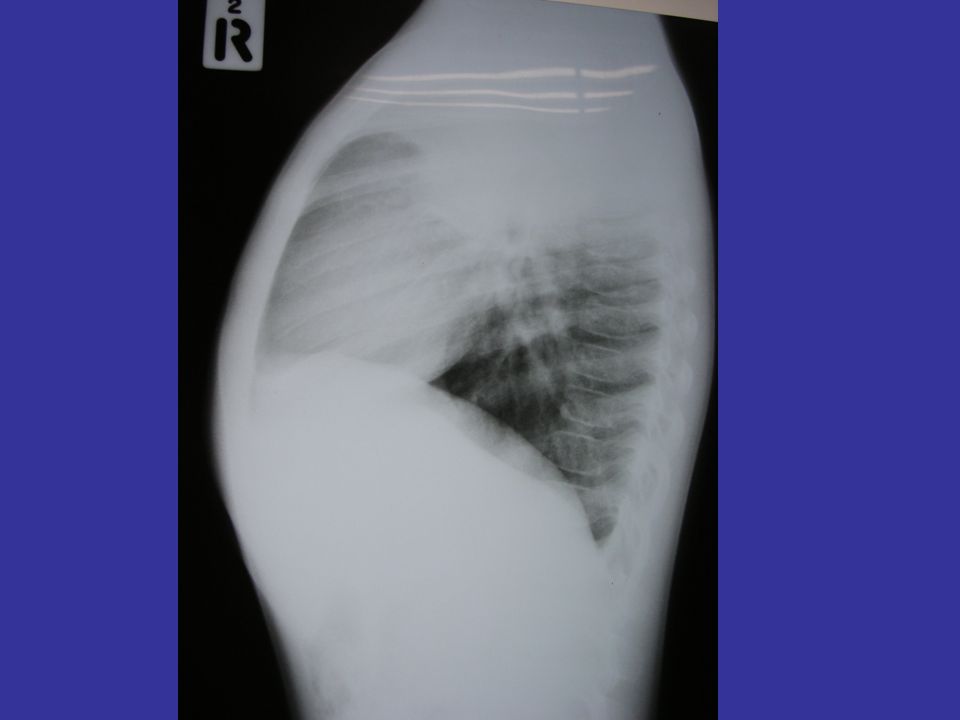
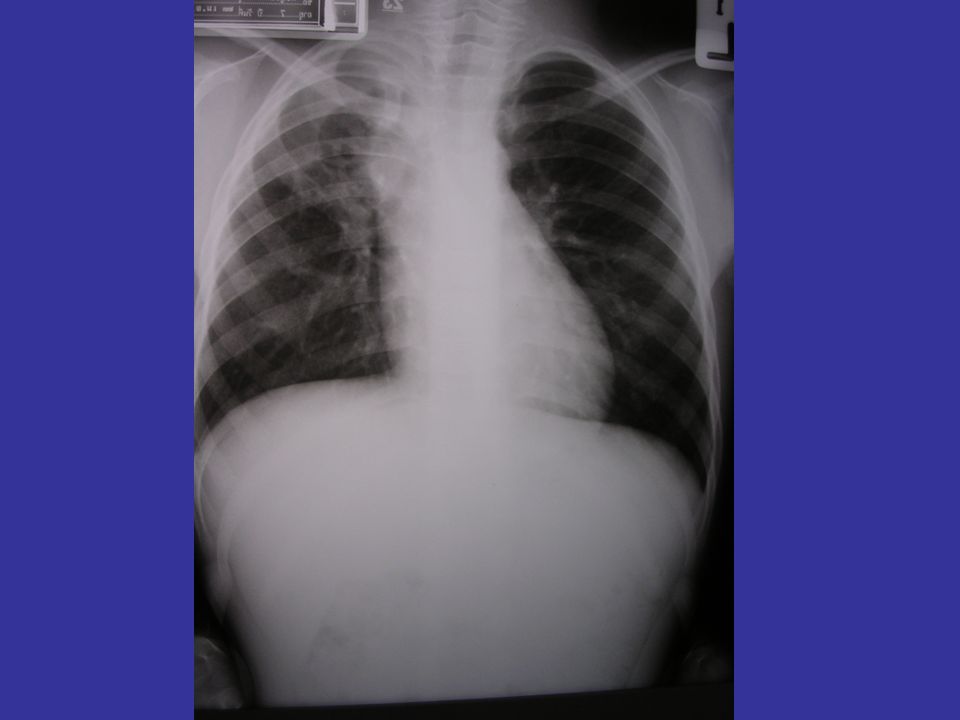
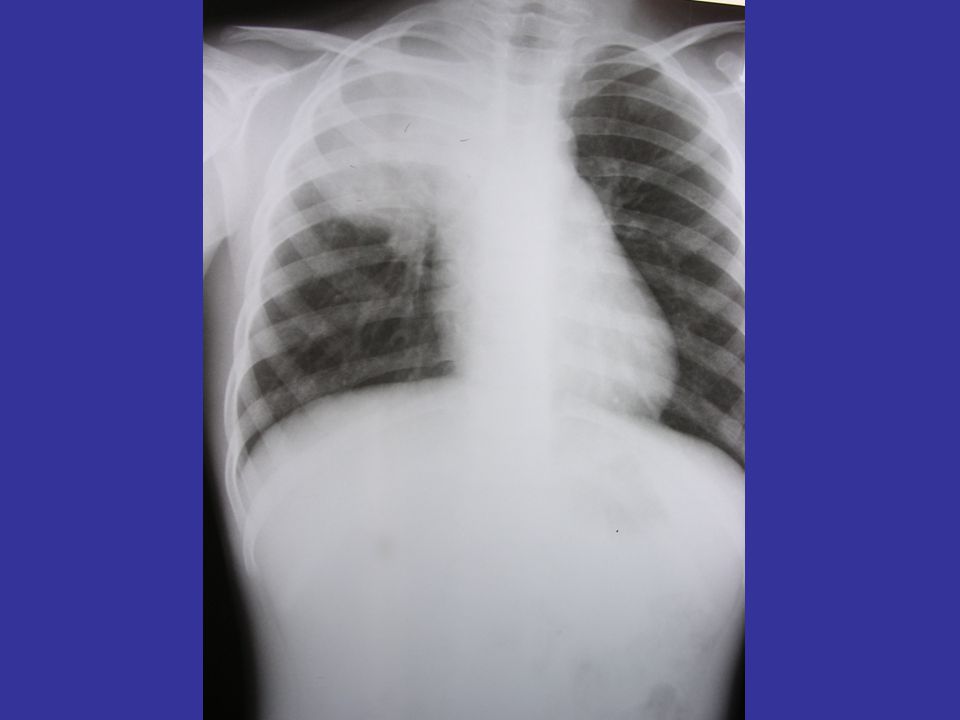
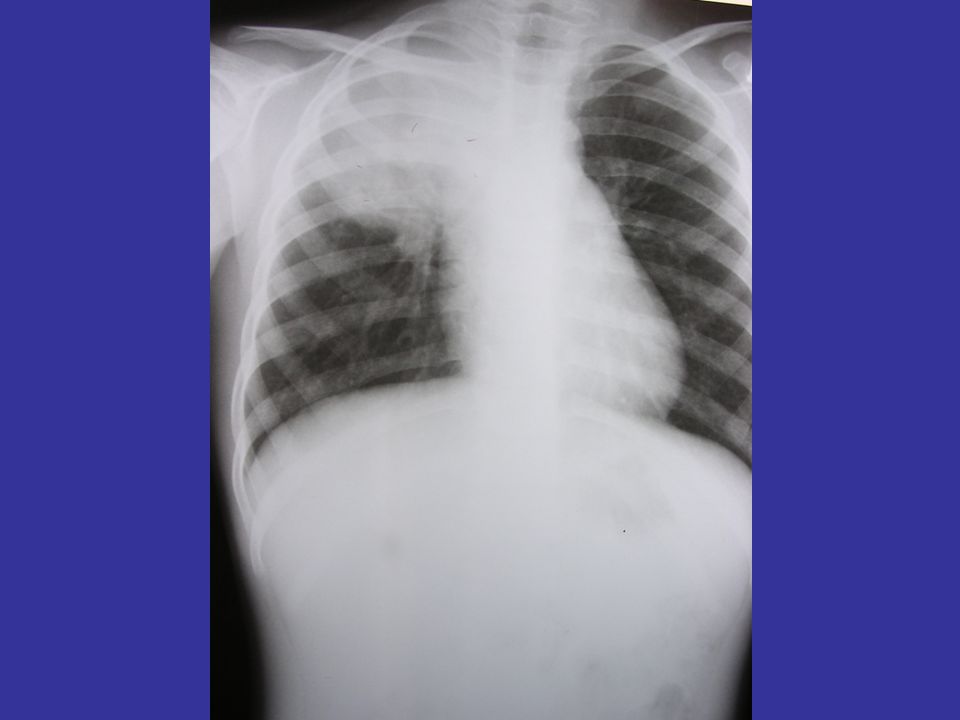
- 2 สัปดาห์ ก่อน ขณะกำลังเล่นกับน้อง ถูกดาบพลาสติกกระแทกที่หลัง แล้วมีอาการไอออกมาเป็นเลือดสด ประมาณครึ่งแก้ว เจ็บหน้าอกขวา เหนื่อย และไอเป็นเลือดสดอีก 2 ครั้ง จึงรีบไปรพ.เจ้าพระยายมราช ได้ Admit ทำ sputum for AFB × 3 วัน neg, CXR พบ haziness RUL คล้ายเดิม ทำ CT chest ผลเป็น thickened wall cystic mass with thick fluid contained at RUL และRefer มารพ.พระมงกุฎเกล้า

5
PH : ปฏิเสธโรคประจำตัว
ปฏิเสธเบื่ออาหาร น้ำหนักลด ปฏิเสธประวัติ contact TB Prenatal Hx : good ANC , no complication Natal : NL, Term , BW = 2,800gm , แข็งแรงดี Nutrition : อาหาร 3 มื้อ ,ไม่ชอบกินผัก G&D : เรียน ประถมศึกษาปีที่ 2 การเรียนปานกลาง Vaccine : BCG , HBV 3 ,OPV 5 ,DPT 5 , MMR2 , JE 3

6
Drug and Allergy : ปฏิเสธการแพ้ยา และแพ้อาหาร
Family Hx บุตรคนที่ 1/2 น้องชาย 1 คน อายุ 5 ปี แข็งแรงดี บิดาอายุ 29 ปี อาชีพ รับจ้าง มารดาอายุ 28 ปี อาชีพ แม่บ้าน บ้านอยู่กลางทุ่งนา สัตว์เลี้ยงเป็นแมว,สุนัข ประมาณ 1 ปี ก่อน ลุง 2 คน มีอาการไอและถ่ายเหลวเรื้อรัง เสียชีวิตในเวลาใกล้เคียงกัน

7
v/s : BT = 37.0 c , PR = 95 mmHg , RR = 20/min , BP = 87/55 mmHg
Physical examination v/s : BT = 37.0 c , PR = 95 mmHg , RR = 20/min , BP = 87/55 mmHg Height = cm ( 3rd percentile ) Weight = 18 Kg ( 10th percentile ) GA : A Thai girl, good consciousness. HEENT : No pale conjunctivae , anicteric sclerae, Pharynx and tonsils are not injected. Lungs : Decreased breath sound at RUL, increased vocal resonance at RUL.
 Weight = 18 Kg ( 10th percentile ) GA : A Thai girl, good consciousness. HEENT : No pale conjunctivae , anicteric sclerae, Pharynx and tonsils are not injected. Lungs : Decreased breath sound at RUL, increased vocal resonance at RUL.")
8
CVS : No active precordium , normal S1 ,S2,
no murmurs. Abdomen : No distension , soft, no guarding , no rigidity. No hepatosplenomegaly. Extremities : No rash , no edema .

9
Lab Investigation CBC: Hct 34.3 % Hb 11.2 g/dl WBC 8,100 cells/mm3
PMN 50 % ,Lym 38 % ,Mono 7 %, EO 4.9 % Platelet 364,000 cells/mm3 ESR = 7 mm/hr

10
Lab Investigation (cont.)
Serum electrolyte Na mmol/L K mmol/L Cl mmol/L CO mmol/L BUN = 2.3 mmol/L , Cr = 41 mmol/L Coagulogram - PT = 11.4 - PTT = 23.6 - INR = 11.4 - TT = 6.5

11
Lab Investigation (cont.)
LFT Alb = 40 , Glob = 34 , SGOT = 24 , SGPT = 11 , TB = 11 , DB = 1 LDH = 199 U/L

14
What is the most likely pathogen?
A) M. tuberculosis B) S. pneumoniae C) Staphylococcus spp. D) Anaerobic bacteria E) Others (not list above)
 M. tuberculosis. B) S. pneumoniae. C) Staphylococcus spp. D) Anaerobic bacteria. E) Others (not list above)")
15
What is your further investigation?
A) lung biopsy B) Bronchoscopy with BAL C) Endotracheal intubation and collect sputum D) MRI chest E) Serology and antigen detection
 lung biopsy. B) Bronchoscopy with BAL. C) Endotracheal intubation and collect sputum. D) MRI chest. E) Serology and antigen detection.")
16
Lab Investigation (cont.)
Melioid titer : negative Anti-HIV (ELISA) : negative
 : negative.")
17
Lab Investigation (cont.)
Bronchoscope with BAL findings: brown color, thick, mud-like fluid at RUL bronchus BAL gram stain : mixed organism AFB : not found Modified AFB : not found AFB culture : no growth Anaerobic culture : no growth Culture for fungus : Aspergillus fumigatus

18
Treatment Itraconazole 10 mg/kg/day Continue anti-TB drugs

23
Diagnosis: Chest CT scan – halo sign

24
Diagnosis: Chest CT scan – air crescent sign

28
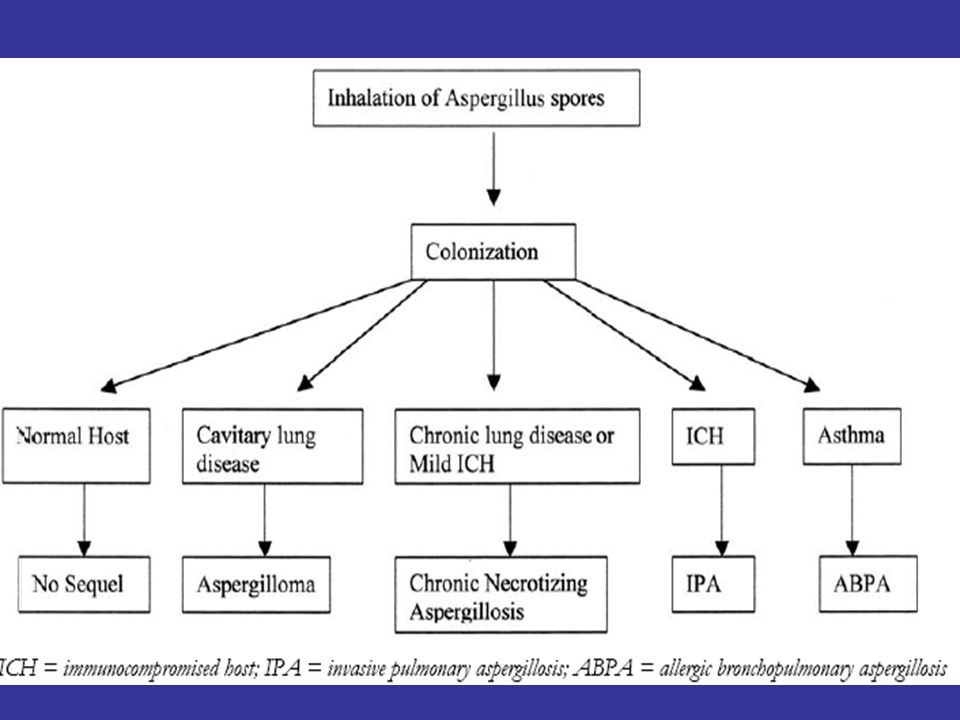
Aspergillosis Clinical manifestration
Allergic bronchopulmonary aspergillosis Allergic sinusitis Aspergillomas and otomycosis Invasive aspergillosis

29
Etiology Aspergillus spp. Aspergillus fumigatus Aspergillus flavus
Aspergillus teres Aspergillus niger

30
Epidemiology Transmitted by inhalation of conidia Host Environment
Impaired phagocytic function Neutropenia Hematologic malignancies Organ transplantation AIDS Environment Constrution area Faultry ventilation

31
Incubation period is unknown
Less likely transmitted by skin contact No person to person spread

33
Mycology Culture of mould from aspirate, BAL or sputum
PCR in BAL, CSF or blood Mycology Mould seen in sinus aspirate Fungal elements seen in sterile body fluids Aspergillus antigen in BAL, CSF or blood Invasive Fungal Infections Cooperative Group

34
Host factors Host factor >3 weeks corticosteroids Neutropenia
>4 days unexplained fever despite broad spectrum antibiotics <36°C or >38°C and: prior mycosis AIDS immunosuppressives >10 days neutropenia Graft versus host disease Invasive Fungal Infections Cooperative Group

35
Pulmonary Mycoses Opportunistic Fungi Endemic Mycoses Aspergillosis
Cryptococcosis Candidiasis Mucormycosis Sporotrichosis Histoplasmosis Coccidiomycosis Endemic Mycoses Histoplasmosis Blastomycosis Cryptococcosis Coccidioidomycosis Paracoccidiodomycosis Penicilliosis Sporotrichosis

36
Diagnostic tests Dichotomously branched and septate hyphae identified by KOH or Gomori methenamine-silver nitrate stain Definitive diagnosis is BAL or tissue biopsy culture Rapid antigen test and PCR also help CT are more specific than CXR

37
Histopathological evidence of IA

38
HRCT Scans Halo sign Air crescent sign
Kuhlman 1987 Chest 92: 95-99; Caillot 2001 J Clin Oncol 19: 253-9

39
Treatment Amphotericin B in high dose ( 1-1.5MKD) for 4-12wks
Itraconazole 5-10 MKD Caspofungin can be used in children

40
Comparative spectrum of activity
Fungus AMB FCZ ITZ CZ PCZ RCZ CF MF AF Candida albicans Candida tropicalis Candida parapsilosis Candida krusei Candida glabrata Cryptococcus neoformans Histoplasma capsulatum Blastomyces dermatitidis Coccidiodes immitis Paracoccidiodes brasiliensis Pneumocystis carinii Aspergillus fumigatus Mucor spp Rhizopus spp Fusarium spp

41
Candins Potent broad spectrum activity Fungicidal
Novel mechanism of activity Low potential for developing resistance Well tolerated in humans

42
Caspofungin Member of a new class of antifungals, the echinocandins
Inhibitors of glucan synthesis in the fungal cell wall Cell wall target absent from mammalian cells Spectrum of activity includes Aspergillus and Candida spp. Unique mechanism of action results in a lack of cross-resistance with azoles and polyenes

43
Caspofungin spectrum of activity
Spectrum of activity includes Candida albicans, non-albicans Candida spp., and Aspergillus spp. Caspofungin is fungicidal for Candida spp. Caspofungin demonstrates clear activity against Aspergillus spp. In vitro, no cross-resistance to Candida spp. with intrinsic or acquired resistance to fluconazole, amphotericin B, or flucytosine No activity against Cryptococcus neoformans Activity against other fungi less well defined

งานนำเสนอที่คล้ายกัน













>")








