ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
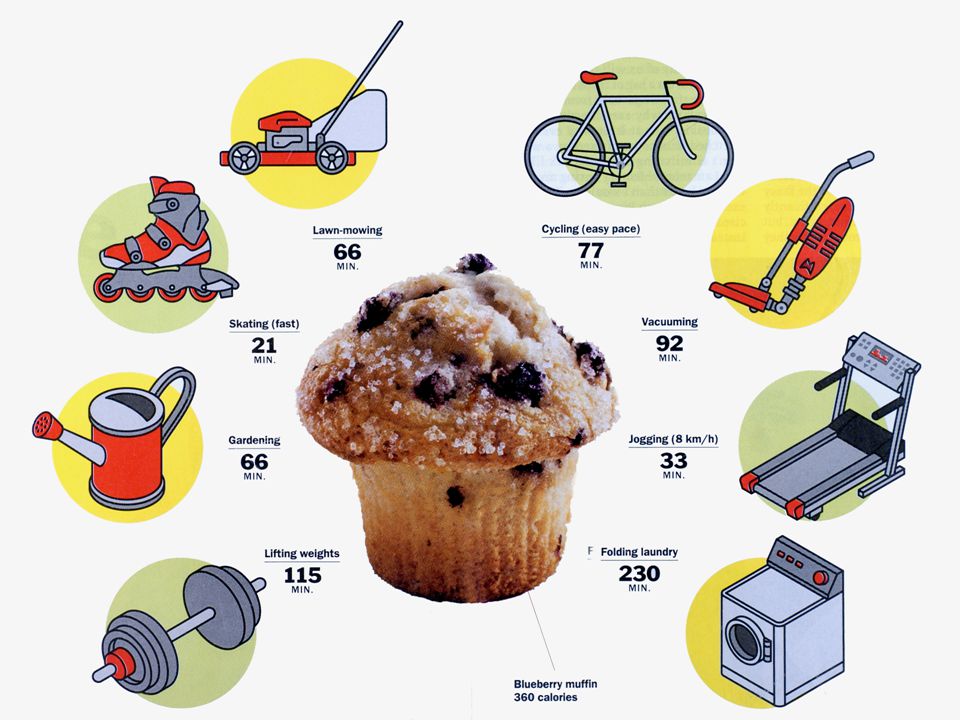
เพราะกินดี จึงอยู่ดี รศ. นพ. ประเสริฐ อัสสันตชัย
รศ. นพ. ประเสริฐ อัสสันตชัย ภาควิชาเวชศาสตร์ป้องกันและสังคม คณะแพทยศาสตร์ศิริราชพยาบาล

4
กินไม่ดี ในผู้สูงอายุ
ภาวะขาดสารอาหาร (under-nutrition) ภาวะสารอาหารเกิน (over-nutrition)
 ภาวะสารอาหารเกิน (over-nutrition)")
5
ภาวะขาดสารอาหารในผู้สูงอายุ
Under-nutrition

6
Why under-nutrition is so important among older patients ?_common
Protein calorie malnutrition Developed country: community 15%, hospital 23-62%, nursing home 85% Thailand : community ชาย (%) หญิง (%) กลุ่มอายุ 60 – 69 ปี 13 – 27 5 – 24 กลุ่มอายุ 70 – 79 ปี 16 – 39 11 – 39 กลุ่มอายุ > 80 ปี 20 – 39 18 – 54 ประเสริฐ อัสสันตชัย การอบรมด้านผู้สูงอายุและความชรา พ.ศ กรุงเทพฯ : โรงพิมพ์แห่งจุฬาลงกรณ์มหาวิทยาลัย 2544 : 58-83
 หญิง (%) กลุ่มอายุ 60 – 69 ปี 13 – – 24. กลุ่มอายุ 70 – 79 ปี 16 – – 39. กลุ่มอายุ > 80 ปี 20 – – 54. ประเสริฐ อัสสันตชัย การอบรมด้านผู้สูงอายุและความชรา พ.ศ กรุงเทพฯ : โรงพิมพ์แห่งจุฬาลงกรณ์มหาวิทยาลัย 2544 :")
7
Why under-nutrition is so important among older patients ?_common
Vitamin deficiency_surveyed in 2,336 cases from 4 parts of Thailand Betacarotene deficiency 83 % Vitamin E deficiency % (vs. 2.5%) Folate deficiency % (vs. 3.3%) Vitamin B1 deficiency 30.1 % (vs. 3-15%) Vitamin C deficiency 9.9 % (vs. 25%) Vitamin A deficiency 6.1 % (vs. 0.3%) Vitamin B12 deficiency 0.6 % (vs. 20%) Assantachai P, et al. Pub Health Nutr 2007; 10 :
 Folate deficiency 38.8 % (vs. 3.3%) Vitamin B1 deficiency 30.1 % (vs. 3-15%) Vitamin C deficiency 9.9 % (vs. 25%) Vitamin A deficiency 6.1 % (vs. 0.3%) Vitamin B12 deficiency 0.6 % (vs. 20%) Assantachai P, et al. Pub Health Nutr 2007; 10 :")
8
- low lean body mass (OR 0.96, 95%CI:0.92-0.98)
Why under-nutrition is so important among older patients ?_underlying causes - Fall - low lean body mass (OR 0.96, 95%CI: ) - low serum albumin (OR 0.96, 95%CI: ) Assantachai P, et al. J Med Assoc Thai 2003; 86: - Osteoporosis - community : low fat mass (OR 0.91, 95%CI: in women) (OR 0.94, 95%CI: in men) Assantachai P, et al. Osteoporos Int 2006; 17 : - nursing home : low lean body mass (regression coefficient 0.003, p 0.03) Assantachai P, et al. Osteoporos Int 2006; 17 :
 - low serum albumin (OR 0.96, 95%CI: ) Assantachai P, et al. J Med Assoc Thai 2003; 86: Osteoporosis. - community : low fat mass (OR 0.91, 95%CI: in women) (OR 0.94, 95%CI: in men) Assantachai P, et al. Osteoporos Int 2006; 17 : nursing home : low lean body mass (regression coefficient 0.003, p 0.03) Assantachai P, et al. Osteoporos Int 2006; 17 :")
9
- Survey in 66 elderly clubs : low BMI OR 1.52, 95%CI:1.09-2.13
Why under-nutrition is so important among older patients ?_underlying causes - Hospitalization - Survey in 66 elderly clubs : low BMI OR 1.52, 95%CI: Assantachai P, et al. J Med Assoc Thai 2005 ; 88 : - Quality of life - Survey in 66 elderly clubs : lack of regular milk intake OR 1.40, 95%CI: Assantachai P, et al. J Med Assoc Thai 2003 ; 86 :

10
Summary of screening issues for under-nutrition
Physical Mental Social Dietary recall Chronic alcoholism Poverty Drug-induced anorexia Mental health assessment Low education, nutritional awareness Oral health Depression screening Live alone Chronic disease esp. chronic diarrhea Dementia screening Poor social input Serial body weight Poor ADL: cooking, shopping

11
How to recognize under-nutrition in older patients ? __clinical setting
MEALS ON WHEELS M: medications E: emotional (depression) A: alcoholism, anorexia, abuse of the elders L: late-life paranoia S: swallowing problems (dysphagia) O: oral problems N: no money (poverty) W: wandering and other dementia-related problems H: hyperthyroidism, pheochromocytoma E: enteric problems (malabsorption) E: eating problems L: low salt, low cholesterol diet S: shopping and meal preparation problems 3 common causes: malignancy, depression, GI problems
 A: alcoholism, anorexia, abuse of the elders. L: late-life paranoia. S: swallowing problems (dysphagia) O: oral problems. N: no money (poverty) W: wandering and other dementia-related problems. H: hyperthyroidism, pheochromocytoma. E: enteric problems (malabsorption) E: eating problems. L: low salt, low cholesterol diet. S: shopping and meal preparation problems. 3 common causes: malignancy, depression, GI problems.")
12
Alternative anthropometric measurement for older Thai people
Demispan measurement cut-off point of Mindex for Thai woman 55.95 kg./m. cut-off point of Demiquet for Thai man 75.6 kg./m.2 Assantachai P, et al. Asia Pacific J Clin Nutr 2006; 15:

13
Over-nutrition

16
Prevalence of chronic diseases among Thai elderly Health System Research Institute 1998
age group 60-69 70-79 80-89 > 90 Knee arthralgia 22.9 26.1 20.8 Low back pain 16.5 17.9 17.7 10.4 Hypertension 14.9 15.0 14.6 6.2 Vision problem 10.2 14.4 16.7 Diabetes mellitus 10.0 7.0 3.1 2.1 Ischemic heart dis. 2.0 4.7 4.2 Stroke 1.7 2.2 3.8 Dementia 1.6 2.4 3.5

17
Chronic diseases influenced long term disability
Chronic diseases influenced long term disability Health System Research Institute 1998 Odds ratio AR* Pop.AR** Accident -- 421 217.2 Stroke 16.89 788 190.7 Eye disease 1.93 152 182.9 Knee pain 1.81 76 179.9 Hypertension 1.50 112 166.0 * AR: attributable risk , ** Pop.AR : population attributable risk

18
Mortality rate of diseases among the Thai Elderly (per 105) Health Policy and Planning Institute 2000 60-74 yr. > 75 yr. rate YLL* Circulatory dis. 574 452567 1936 376946 Cancer 564 461888 897 89321 Diabetes mellitus 213 178984 348 56542 COPD 209 159142 920 162844 GI diseases 114 94674 301 57937 YLL : year of life lost – number of years lost due to premature death

19
Barthel Activity of daily living 2.63 2.27
Conditions related to hypertension in the Thai elderly Health System Research Institute 1999 Hypertension(%) Normal (%) p value Dementia 4.1 2.8 < 0.05 Long term disability 24.9 16.2 < 0.001 Barthel Activity of daily living 2.63 2.27
 Normal. (%) p value. Dementia < Long term disability < Barthel Activity of daily living")
21
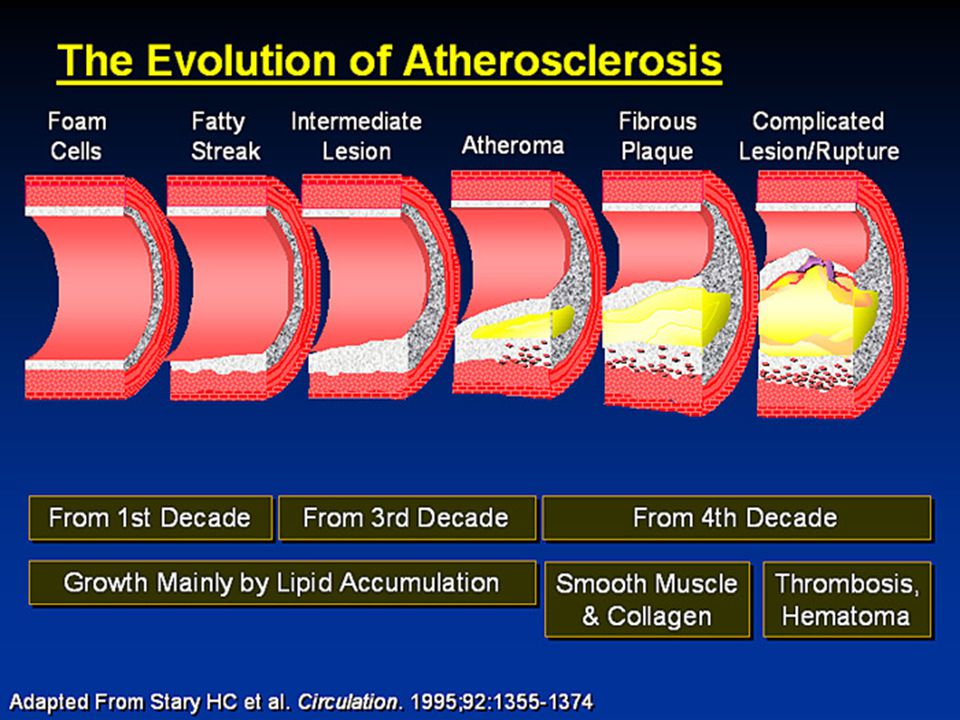
Atherosclerosis risks
Smoking Hypertension : BP>140/90 Dyslipidemia: HDL < 40 Family history of premature coronary heart disease: men < 55, women<65 Age : men > 45, women > 55

22
Atherosclerosis outcomes
Coronary heart disease : angina pectoris, unstable angina, myocardial infarction, congestive heart failure, arrhythmia Cerebrovascular disorders: cerebral infarction, intracerebral hemorrhage Peripheral vascular disease Abdominal aortic aneurysm Retinopathy

23
Distribution of systolic pressure with age
Framingham , Health Survey for England 1994

24
Hypertension in the Elderly
What should be concerned before diagnosis ? Why do they need treatment ? When is the best time of intervention ? What is precaution before starting treatment ? How many forms of management ? What is the most appropriate drug of choice ? How far should blood pressure be lowered? Is it the same between the young old elderly and the very old elderly ?

25
What should be concerned before diagnosis of hypertension in the elderly ?
Variability: white-coat (labile) hypertension Pseudohypertension: Osler manoeuvre ISH :exclude aortic insufficiency, severe anemia, hyperthyroidism, arteriovenous fistula, fever. Secondary hypertension: renal artery stenosis Associated disease : DM, dyslipidemia Personal factors : salt intake, obesity, exercise, smoking, drinking
 hypertension. Pseudohypertension: Osler manoeuvre. ISH :exclude aortic insufficiency, severe anemia, hyperthyroidism, arteriovenous fistula, fever. Secondary hypertension: renal artery stenosis. Associated disease : DM, dyslipidemia. Personal factors : salt intake, obesity, exercise, smoking, drinking.")
26
958 cases followed up 42 months:
White-coat vs. Sustained Hypertension in the Elderly Kario K, et al. J Am Coll Cardiol 2001;38: 958 cases followed up 42 months: 147 (normal), 236 (white-coat), 575 (HT) Stroke occurrence: Normal: 3 (2.0%) White-coat : 5 (2.1%) HT : 54 (9.4%) Incidence of stroke : in white-coat hypertension = in normotensives = ¼ risk in sustained hypertension.
, 236 (white-coat), 575 (HT) Stroke occurrence: Normal: 3 (2.0%) White-coat : 5 (2.1%) HT : 54 (9.4%) Incidence of stroke : in white-coat hypertension = in normotensives = ¼ risk in sustained hypertension.")
27
Isolated Systolic Hypertension-Why?

28
Secondary hypertension in the elderly
Early diagnosis of HT before 30 yrs.old without family history Recent worsening of blood pressure + premature target organ damage Resistant to treatment Recent poor control without obvious reason ARF after ACEI or ARB

29
Hypertension in the Elderly
What should be concerned before diagnosis ? Why do they need treatment ? When is the best time of intervention ? What is precaution before starting treatment ? How many forms of management ? What is the most appropriate drug of choice ? How far should blood pressure be lowered? Is it the same between the young old elderly and the very old elderly ?

30
Mulrow et al. Hypertension in the elderly. JAMA 1994, p.1932-8.
Why do they need treatment?__ 3 stages of clinical trials of hypertension in the elderly Mulrow et al. Hypertension in the elderly. JAMA 1994, p 5-yr NNT Aust EWPHE 16 14 37 52 STOP SHEP MRCOA-beta Summary

31
Second stage of antihypertensive trial in the elderly
การศึกษาโดยใช้ยาในกลุ่ม calcium channel blocker ในช่วงปี ค.ศ ได้แก่ การศึกษา STONE (ใช้ยา nifedipine), SYST-CHINA (ใช้ยา nitrendipine), HOT (ใช้ยา felodipine ) และ PREVENT (ใช้ยา amlodipine) พบว่าสามารถลดอุบัติการณ์ของโรคระบบหัวใจและหลอดเลือดได้ถึงร้อยละ
, SYST-CHINA (ใช้ยา nitrendipine), HOT (ใช้ยา felodipine ) และ PREVENT (ใช้ยา amlodipine) พบว่าสามารถลดอุบัติการณ์ของโรคระบบหัวใจและหลอดเลือดได้ถึงร้อยละ")
32
Third stage of antihypertensive trial in the elderly
การศึกษาโดยใช้ยาในกลุ่ม angiotensin converting enzyme inhibitor และกลุ่มangiotensin receptor blocker (ARB) ในช่วงปี ค.ศ.2000 ถึงปัจจุบัน การศึกษา HOPE ที่ใช้ยา ramipril พบว่าสามารถลดอัตราตายจากโรคระบบหัวใจและหลอดเลือดได้อย่างมีนัยสำคัญ (relative risk 0.74) การศึกษา PROGRESS ที่ใช้ยา perindopril ร่วมกับ indapamide ในผู้ป่วยที่มีประวัติโรคหลอดเลือดสมอง พบว่าลดความเสี่ยงต่อการเกิดโรคหลอดเลือดสมองซ้ำได้อย่างมีนัยสำคัญ การศึกษา SCOPE ใช้ยา candesartan ซึ่งไม่ลดอุบัติการณ์ของโรคหลักในระบบหัวใจและหลอดเลือด แต่ลดอุบัติการณ์ของ non-fatal stroke ได้อย่างมีนัยสำคัญราวร้อยละ 28
 ในช่วงปี ค.ศ.2000 ถึงปัจจุบัน. การศึกษา HOPE ที่ใช้ยา ramipril พบว่าสามารถลดอัตราตายจากโรคระบบหัวใจและหลอดเลือดได้อย่างมีนัยสำคัญ (relative risk 0.74) การศึกษา PROGRESS ที่ใช้ยา perindopril ร่วมกับ indapamide ในผู้ป่วยที่มีประวัติโรคหลอดเลือดสมอง พบว่าลดความเสี่ยงต่อการเกิดโรคหลอดเลือดสมองซ้ำได้อย่างมีนัยสำคัญ. การศึกษา SCOPE ใช้ยา candesartan ซึ่งไม่ลดอุบัติการณ์ของโรคหลักในระบบหัวใจและหลอดเลือด แต่ลดอุบัติการณ์ของ non-fatal stroke ได้อย่างมีนัยสำคัญราวร้อยละ 28.")
33
Hypertension in the Elderly
What should be concerned before diagnosis ? Why do they need treatment ? When is the best time of intervention ? What is precaution before starting treatment ? How many forms of management ? What is the most appropriate drug of choice ? How far should blood pressure be lowered? Is it the same between the young old elderly and the very old elderly ?

34
Hypertension in the Elderly
salt intake In general: every Na 100 mmol SP 4-5 mmHg DP 2 mmHg In elderly: every Na 100 mmol SP 10 mmHg In elderly with 95 percentile of BP : every Na 100 mmol SP 15 mmHg Law MR, et al. Br Med J 1991; 312:

35
Hypertension in the Elderly
Obesity Among the Thai elderly: Hypertensive cases BMI, subcutaneous fat, percent body fat ประเสริฐ อัสสันตชัย โครงการศึกษาวิจัยครบวงจรเรื่องผู้สูงอายุไทย ม.มหิดล 2542. INTERSALT study BW 10 kg. SP 3 mmHg Dyer et al. J Hum Hypertension 1989; 3: 299.

36
Hypertension in the Elderly
Exercise Regular exercise decrease blood pressure in general : 3 / 3 mmHg in mild hypertensives : 6 / 7 mmHg in overt hypertensives : 10 / 8 mmHg Fagard RH J Hypertension 1993; 11(Suppl.5) : S47-52.
 : S")
37
Hypertension in the Elderly
Alcoholic drinking linear relationship of blood pressure and alcohol 1 unit of alcohol per day SP 1 mmHg Klatsky AL, et al. N Eng J Med 1977; 296: 1194. In UK study - men with 35 unit/wk. more hypertensive than men with 1-10 unit/wk. - the effect more pronounced among the ones aged than those aged Rimm EB, et al. Lancet 1991; 338: 464.

38
How far should blood pressure be lowered
How far should blood pressure be lowered? Is it the same between the young old elderly and the very old elderly ? Rationale A 5-year retrospective study in Finland in 561 older people aged > 85 yrs,mortality was greatest among lowest BP, and lowest among SP > 160, DP > 90 mmHg. Mattila et al. Br Med J 1988; 296:887-9. A study in California, a paradoxical increase in survival was found in men aged > 75 yrs with increasing DP. Langer et al. Br Med J 1989; 298:

39
80 years old milestone !! Antihypertensive treatment in < 80 years old : stroke 25 – 40% cardiac events 13 – 27% all cardiovascular events 17 – 40% Antihypertensive treatment in > 80 years old ??

40
The Hypertension in the Very Elderly Trial (HYVET). Bulpitt CJ et al
The Hypertension in the Very Elderly Trial (HYVET) Bulpitt CJ et al. J Hypertension 2003;21: submitted for entry = 1372 excluded 89 cases: SBP< 160, DBP<90 & >109 antihypertensives treatment age<80 mental test score < 7 creatinine > 150 μmol/l 1283 cases assigned to groups
 Bulpitt CJ et al. J Hypertension 2003;21: submitted for entry = excluded 89 cases: SBP< 160, DBP<90 & >109. antihypertensives treatment. age<80. mental test score < 7. creatinine > 150 μmol/l cases assigned to groups.")
41
The Hypertension in the Very Elderly Trial (HYVET)
No treatment n = 426 Diuretic n = 426 ACE inhibitor n = 431 pilot trail : March 1994 – June 1998 died n = 30 lost n = 9 complete 386 died n = 27 lost n = 7 complete = 397 died n = 22 lost n = 8 complete = 394

42
HYVET-Pilot study_CONCLUSION
Treatment of 1000 patients for 1 year may reduce stroke events by 19 (9 non-fatal), but may be associated with 20 extra non-stroke deaths. Each stroke saved by antiHT treatment, there was one non-stroke death.
, but may be associated with 20 extra non-stroke deaths. Each stroke saved by antiHT treatment, there was one non-stroke death.")
43
HYVET_main clinical trial
International trial 3,845 cases aged > 80 with SP mmHg. Indapamide SR or placebo Add-on : ACEI (perindopril mg/d.) Target BP 150 / 80 mmHg. Results: all stroke (RR 0.59, p 0.009), relative risk reduction - 41% all death from any cause (RR 0.76, p 0.007), relative risk reduction – 24%
 Target BP 150 / 80 mmHg. Results: all stroke (RR 0.59, p 0.009), relative risk reduction - 41% all death from any cause (RR 0.76, p 0.007), relative risk reduction – 24%")
44
Quality of life in Syst-Eur Trial. Fletcher AE, et al
Quality of life in Syst-Eur Trial Fletcher AE, et al. J Hypertension 2002; 20: Isolated systolic hypertension in older people 4695 cases aged > 60 yrs, SP & DP >95 mmHg. Double-blind RCT, nitrendipine+enalapril+HCTZ Target sitting SP<150 (at least 20 mmHg reduction from baseline) followed for 2 yrs. Result: 42% ↓strokes (p<.003), 26%↓cardiac events (p<.03) Quality of life:Sickness Impact Profile(SIP), Brief Assessment Index (BAI) Conclusion: active treatment was associated with some small adverse impacts on quality of life.
 followed for 2 yrs. Result: 42% ↓strokes (p<.003), 26%↓cardiac events (p<.03) Quality of life:Sickness Impact Profile(SIP), Brief Assessment Index (BAI) Conclusion: active treatment was associated with some small adverse impacts on quality of life.")
45
การศึกษาที่ติดตามผู้ที่มีอายุ 80 ปีขึ้นไปที่เป็นโรคความดันเลือดสูงและได้รับยาลดความดันเลือดเป็นเวลา 5 ปี พบว่าในบรรดาผู้ที่มีระดับความดันเลือดอยู่ในเกณฑ์ที่ควบคุมได้ ผู้ที่มีระดับความดันเลือดต่ำกว่าจะมีอัตราการรอดชีวิตที่ 5 ปี (5-year survival rate) น้อยกว่า ผู้ที่มีระดับความดันเลือดสูงกว่า Oates DJ, et al. Blood pressure and survival in the oldest old. J Am Geriatr Soc 2007 ; 55 : 383-8

46
จากการศึกษา SHEP พบว่าในกลุ่มผู้ที่มีระดับความดันเลือดปกติหลังได้รับการรักษา ถ้า DP ลดลงไปอีก 5 มม.ปรอทจากค่าเฉลี่ย 77 มม.ปรอท จะมีความเสี่ยงต่อการเกิดโรคในระบบหัวใจและหลอดเลือดเพิ่มขึ้นถึงร้อยละ ปรากฏการณ์นี้เรียกว่า J – curve ซึ่งพบใน DP มากกว่าจาก SP Somes GW, et al. The role of diastolic blood pressure when treating isolated systolic hypertension. Arch Intern Med 1999 ; 159 : Cruickshank JM, et al. Benefits and potential harm of lowering high blood pressure. Lancet 1987; 1 :

47
ไขมันในช่องท้องมากเกิน
Apple shape/ visceral fat Pear shape/ Subcutaneous fat Obesity Urbanization - Westernized diet - Physical inactivity IDF Criteria 2005 Metabolic Syndrome Waist circumference - Male >90 cm - Female >80 cm กลุ่มโรค อ้วนลงพุง Plus 2 of the followings - Triglyceride >150 mg/dl - HDL-C: Male <40 mg/dl Female <50 mg/dl - BP >130/85 mmHg/on Rx - FBS >100 mg/dl Intra-Abdominal Adiposity ไขมันในช่องท้องมากเกิน

48
Diabetes mellitus Adverse outcomes
Macrocirculation: heart disease, stroke Microcirculation : renal disease, retinopathy Delayed wound healing Infection : TB, fungus

49
Endocrine Changes in Aging
Physiologic changes Clinical correlation impaired glucose tolerance ↑ DM ↑ BS 5.3 mg%/10yrs after 30 years old ↑ serum insulin metabolic syndrome

50
Changes in blood glucose levels with age
Postprandial Fasting Elahi D, et al. Eur J Clin Nutr 2000; 54: S112-S120.

51
Natural History of Type 2 Diabetes
Glucose Post-prandial glucose 100 200 150 300 250 350 mg/dL Fasting glucose Relative to normal 250 Insulin resistance 200 (%) 150 100 At risk for diabetes 50 Beta-cell dysfunction Insulin level -10 -5 5 10 15 20 25 30 Years R.M. Bergenstal, International Diabetes Center
 At risk for. diabetes. 50. Beta-cell dysfunction. Insulin level Years. R.M. Bergenstal, International Diabetes Center.")
52
Diabetes mellitus Symptoms of DM + random blood glucose > 200 mg/dl. (8 hours) Fasting plasma glucose > 126 mg/dl Two-hour plasma glucose > 200 mg/dl NB: repeat testing on a different day

53
Diabetes mellitus Ideal goals for glycemic control normal goal action
Preprandial < <80, >140 glucose HbA1c(%) < 6 < 7 > 8
 < 6 < 7 > 8.")
54
Target of dyslipidemia treatment
Cholesterol = triglyceride/5 + HDL + LDL Goal : risk LDL 0-1 risk < 160 2+ risks < 130 CHD, DM < 100

55
Dietary therapy: special considerations for older people with diabetes
financial difficulty shopping difficulty due to mobility problems poor food preparation skills esp. widowed men ingrained dietary habits difficulty following dietary instruction because of impaired cognitive function ↓ taste ↑ frequency of constipation

56
You are what you eat !!

งานนำเสนอที่คล้ายกัน








>")



 98.08% 100.02% จังหวัด.>")








