ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Acute Pain (Postoperative) Management
การระงับปวดหลังผ่าตัด Acute Pain (Postoperative) Management ศ. สมบูรณ์ เทียนทอง ภาควิชาวิสัญญีวิทยา คณะแพทยศาสตร์ มหาวิทยาลัยขอนแก่น June 2008
 Management. ศ. สมบูรณ์ เทียนทอง. ภาควิชาวิสัญญีวิทยา. คณะแพทยศาสตร์ มหาวิทยาลัยขอนแก่น. June")
2
หัวข้อบรรยาย ความสำคัญของการระงับปวด การประเมินและบันทึกความปวด
IM PRN : ทำอย่างไรให้ได้ดีกว่าเดิม เทคนิคการระงับปวดในปัจจุบัน New Concepts in PO pain management การติดตามผลการรักษา (APS)
")
3
ถ้าไม่ต้องรับรู้อาการปวดเลยจะดีหรือไม่ ?

4
Definition “Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage “ (IASP, 1979 ) ความปวด “ คือประสบการณ์ทางความรู้สึกและอารมณ์ที่ไม่สบาย ซึ่งเกิดขึ้นร่วมกับการที่เนื้อเยื่อถูกทำลาย หรือถูกบรรยายประหนึ่งว่ามีศักยะในการทำลายเนื้อเยื่อนั้น”
 ความปวด. คือประสบการณ์ทางความรู้สึกและอารมณ์ที่ไม่สบาย ซึ่งเกิดขึ้นร่วมกับการที่เนื้อเยื่อถูกทำลาย หรือถูกบรรยายประหนึ่งว่ามีศักยะในการทำลายเนื้อเยื่อนั้น")
5
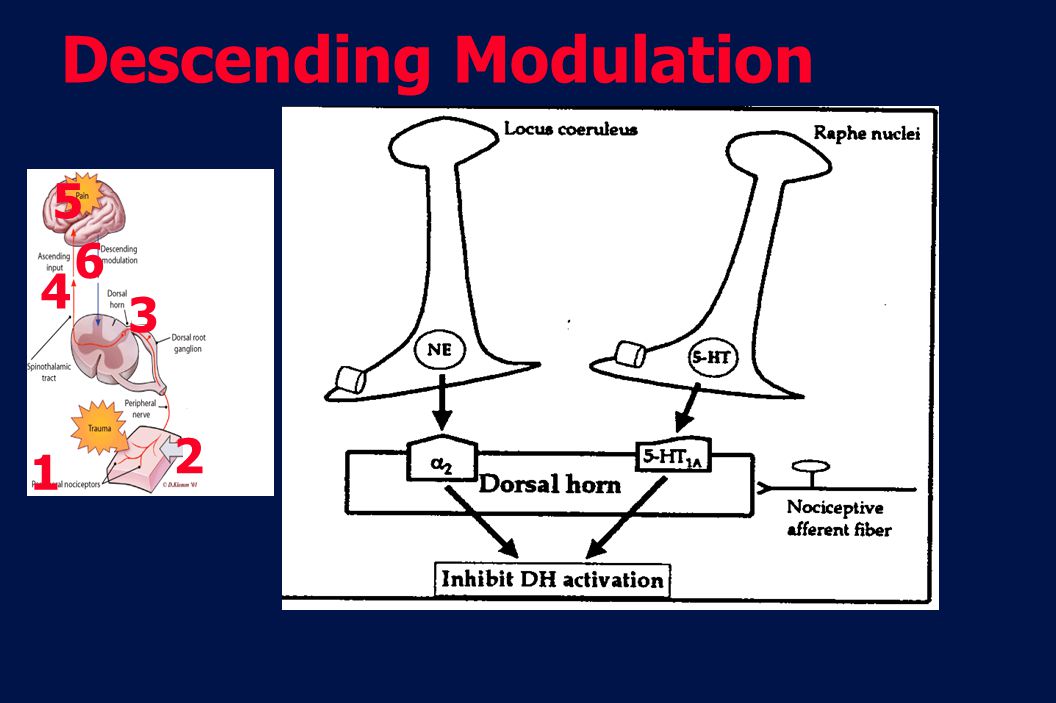
Postoperative Pain (Pain Transmission)
Descending modulation Dorsal Horn Sensitizing soup Ascending input Dorsal root ganglion Inflammatory mediators - Prostaglandin, Substance-P, H+, Histamine, etc., Spinothalamic tract Peripheral nerve Trauma This slide illustrates the pathways of pain. Pain is transmitted as a nerve signal. Pain response is a complex process that involves both the peripheral nervous system (PNS) and central nervous system (CNS).1 The transduction of noxious stimuli typically begins with peripheral nociceptors. Signals from these nociceptors travel to the dorsal horn of the spinal cord and then along the spinothalamic tract to the thalamus and cortex of the brain1 COX-2 contributes to increased pain sensitivity peripherally at the nociceptors as well as centrally at the dorsal horn2 References: 1. Gottschalk A, Smith DS. New concepts in acute pain therapy: preemptive analgesia. Am Fam Physician. 2001;63: Samad TA, Moore KA, Saperstein A, et al. Interleukin-1β-mediated induction of COX-2 in the CNS contributes to inflammatory pain hypersensitivity. Nature. 2001;410: Peripheral nociceptors Adapted from Gottschalk A et al. Am Fam Physician. 2001;63:1981, and Kehlet H et al. Anesth Analg. 1993;77:1049.
 and central nervous system (CNS).1. The transduction of noxious stimuli typically begins with peripheral nociceptors. Signals from these nociceptors travel to the dorsal horn of the spinal cord and then along the spinothalamic tract to the thalamus and cortex of the brain1. COX-2 contributes to increased pain sensitivity peripherally at the nociceptors as well as centrally at the dorsal horn2. References: 1. Gottschalk A, Smith DS. New concepts in acute pain therapy: preemptive analgesia. Am Fam Physician. 2001;63: Samad TA, Moore KA, Saperstein A, et al. Interleukin-1β-mediated induction of COX-2 in the CNS contributes to inflammatory pain hypersensitivity. Nature. 2001;410: Peripheral. nociceptors. Adapted from Gottschalk A et al. Am Fam Physician. 2001;63:1981, and Kehlet H et al. Anesth Analg. 1993;77:1049.")
6
Gate Control Theory

8
Chronic Pain: Myofascial, neuropathic Pain
Nociceptive Pain Central sensitization: Neurotransmitters 1 2 6 3 4 5 Chronic Pain: Myofascial, neuropathic Pain

9
Brain Ascending Tracts Descending Tracts
Frontal Cortex -Cingulate Gyrus -Insula & Other structures in Limbic system Thalamic Nuclei Hypothalamic Nuclei -Paraventricular Nucleus Amygdala Lucus Ceruleus Rostral Pons Periaquaductal grey

10
Descending Modulation
1 2 6 3 4 5
11
ความปวดอาจมีผลเสียอะไรบ้าง
Anxiety Immobilization Tissue hypersensitive Neuro modulation Regional blood flow PA I N DVT Plt aggregation RS Na retention CAD Stress response HYPOXIA O2 consumption Delayed healing Immune

12
2 Cases นาย......

13
Effective Pain Management: มีข้อดีอะไรบ้าง
Patient comfort and satisfaction1,2,3 Earlier mobilization4 ↑ Pulmonary outcomes5 Hospital stay3,4 Costs4 1. Eisenach JC, et al. Anesthesiology. 1988;68:444–448. 2. Harrison DM, et al. Anesthesiology. 1988;68:454–457. 3. Miaskowski C, et al. Pain. 1999;80:23–29. 4. Finley RJ, et al. Pain. 1984;2:S397. 5. Ballantyne JC, Anesth Analg 1998; 86(3):
:")
14
Pain Continues to be Undertreated
Postoperative pain U.S., 1993 and 20031,2 Any Pain 77% 82% 1993 (n=135) 2003 (n=250) Moderate Pain 49% 47% Severe Pain 23% 21% Slight Pain 19% 13% Extreme Pain 8% 18% A survey of 250 patients published in 2003 showed that pain management generally did not improve over a 10-year period, while the incidence of extreme pain increased.1,2 A 1993 study by Warfield et al showed that the incidence and severity of postoperative pain was high1,2 3 out of 4 patients experienced pain after surgery1,2 80% rated their pain as moderate to extreme1,2 A follow-up study by Apfelbaum et al showed that the incidence of pain after surgery had not improved in the preceding 6 years1 Nearly 80% of all patients reported experiencing pain after surgery1 The vast majority of these patients reported pain that was moderate to extreme1 References: 1. Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97: Warfield CA, Kahn CH. Acute pain management: programs in U.S. hospitals and experiences and attitudes among U.S. adults. Anesthesiology. 1995;83: Undertreated 1Adapted from Apfelbaum JL et al. Anesth Analg. 2003;97: Warfield CA et al. Anesthesiology. 1995;83: Why?
 2003 (n=250) Moderate. Pain. 49% 47% Severe. Pain. 23% 21% Slight. Pain. 19% 13% Extreme. Pain. 8% 18% A survey of 250 patients published in 2003 showed that pain management generally did not improve over a 10-year period, while the incidence of extreme pain increased.1,2. A 1993 study by Warfield et al showed that the incidence and severity of postoperative pain was high1,2. 3 out of 4 patients experienced pain after surgery1,2. 80% rated their pain as moderate to extreme1,2. A follow-up study by Apfelbaum et al showed that the incidence of pain after surgery had not improved in the preceding 6 years1. Nearly 80% of all patients reported experiencing pain after surgery1. The vast majority of these patients reported pain that was moderate to extreme1. References: 1. Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97: Warfield CA, Kahn CH. Acute pain management: programs in U.S. hospitals and experiences and attitudes among U.S. adults. Anesthesiology. 1995;83: Undertreated. 1Adapted from Apfelbaum JL et al. Anesth Analg. 2003;97: Warfield CA et al. Anesthesiology. 1995;83: Why")
15
Barriers to pain relief
นโยบาย (ชาติ) ระบบการบริการ ตัวผู้ป่วย/ญาติ ระบบบริหาร รพ. ทักษะและความรู้เรื่องความปวด เลือกเทคนิคระงับปวดไม่เหมาะสม ปัญหาควบคุมยาเสพติด:ใบ ยส. ความเชื่อที่ผิดๆ กลัวผลแทรกซ้อนของยา/ติดยา ไม่ใช่หน้าที่ แพทย์/พยาบาล ความรู้ Attitude (ไม่ถูก) Rawal N. Anesth Pain Med. 1999;24(1):68–73. Sinatra R. In: Cousins MJ, Bridenbaugh PO. Neural Blockade in Clinical Anesthesia and Management of Pain; 1998:793–835. American Pain Society Quality Improvement Committee. JAMA. 1995;1847–1880.
 ระบบการบริการ. ตัวผู้ป่วย/ญาติ ระบบบริหาร. รพ. ทักษะและความรู้เรื่องความปวด. เลือกเทคนิคระงับปวดไม่เหมาะสม. ปัญหาควบคุมยาเสพติด:ใบ ยส. ความเชื่อที่ผิดๆ. กลัวผลแทรกซ้อนของยา/ติดยา. ไม่ใช่หน้าที่ แพทย์/พยาบาล. ความรู้ Attitude. (ไม่ถูก) Rawal N. Anesth Pain Med. 1999;24(1):68–73. Sinatra R. In: Cousins MJ, Bridenbaugh PO. Neural Blockade in Clinical Anesthesia and Management of Pain; 1998:793–835. American Pain Society Quality Improvement Committee. JAMA. 1995;1847–1880.")
16
การระงับปวดเริ่มต้นด้วย 2A
A1. = Attitude, A2 = Assessment รายงานนักเรียน ปวดเล็กน้อย ปวดพอทน รายละเอียด pain

17
การประเมินความปวดทำได้อย่างไร?
“Self-report” Numeric rating scale (NRS) 0 - 10 2. Verbal rating scale (VRS) no pain, mild, moderate, severe 3.Visual Analogue scale (VAS) x
 Verbal rating scale (VRS) no pain, mild, moderate, severe. 3.Visual Analogue scale (VAS) 0 x 10.")
18
เครื่องมือประเมินความปวด
ไม่ปวด มากที่สุด NRS 1 2 8 3 4 5 6 7 9 10 ไม่ปวด เล็กน้อย ปานกลาง มาก มากที่สุด VRS มากที่สุด ไม่ปวด Face

19
การที่จะประเมินความปวดได้ง่ายและน่าเชื่อถือ
จำเป็นที่จะต้องสอนผู้ป่วยก่อนผ่าตัด 15 สอนขณะให้ IV ศศิวิมล และคณะ วิสัญญีสาร 2548?

20
Pain assessment (Children)
Face scale

21
รวม 10 รักษา>3

22
2001 JCAHO Pain Management Standards
Patients have the right to appropriate assessment and management of pain Pain is considered the 5th vital sign Pain intensity ratings are required to be recorded with BT, PR, BP and RR

23
Pain: The Fifth Vital Sign™1*

24
Pain Control :Techniques
จาก 2 A มาถึง Knowledge เทคนิคการระงับปวดหลังผ่าตัด IV infusion Oral Traditional Methods IV PCA Pain Control :Techniques Others - IA Morphine - PNB, LA Epidural Analg Low – Hi tech เลือกตามความเหมาะสม: อายุ ชนิดการผ่าตัด Spinal Morphine

25
การระงับปวดด้วยวิธี IM ได้ผลอย่างไร Pain Intensity by Techniques
% Dolin. Br J Anaesth 2002 Pain Intensity by Techniques

26
แนวโน้มการใช้ IM ในการระงับปวด
No of Studies (N = 165) Dolin. Br J Anaesth 2002;89:
 Dolin. Br J Anaesth 2002;89:")
27
หลับ/มีอาการแทรกซ้อน
Order แบบ PRN ระดับยาลดต่ำ ผู้ป่วยมีอาการปวด ผู้ป่วยขอยาแก้ปวด พยาบาลรับทราบ พยาบาลดูผู้ป่วย อ่านคำสั่ง/ ตัดสินใจให้ยา เตรียมยา ฉีดยา ยาดูดซึม ยาออกฤทธิ์ ระดับยาสูงเกินไป/ หลับ/มีอาการแทรกซ้อน Response time 27-42 min(1) 1.Chan, Reg Anesth 1995;20: Pain Cycle: 10 Steps of PRN
 1.Chan, Reg Anesth 1995;20: Pain Cycle: 10 Steps of PRN.")
28
พยาบาล ผู้ป่วย PRNvs Around the Clock: Concept ที่ต่างกัน
จุดอ่อน PRN: จุดอ่อน ATC: - ไม่กล้าขอยา Breakthrough pain - Response ช้า

29
ทำไม pare สั้นกว่า valde ในเมื่อ pare valde
BMC Anesthesiology 2003,3

30
IM PRN จะดีกว่าเดิมได้อย่างไร
PACU IM PRN จะดีกว่าเดิมได้อย่างไร Web site APS มีแนวทางระงับปวด - มีการประเมินความปวด - มีการติดตามผลการรักษา - Rescue dose - มีการบันทึกความปวด

31
Srinagarind Med J 2002; 17(1): 2-3.
การฉีดยาระงับปวดเข้ากล้ามมีข้อเสียอะไร? Srinagarind Med J 2002; 17(1): 2-3. Dose/day = ? (น้อย) SE: เกิดแต่ช้า การระงับปวด: เกิดช้าเช่นเดียวกัน
: 2-3. Dose/day = (น้อย) SE: เกิดแต่ช้า. การระงับปวด: เกิดช้าเช่นเดียวกัน.")
33
in Post- op Pain Management
New Concepts in Post- op Pain Management Preemptive analgesia: มีอะไรใหม่? Multimodal Analgesia Pain Management by Type Specific Procedures There are many ways to effectively treat acute and chronic pain. Each of these options offers its own benefits and risks. No single option is right for every patient. NOTE: for more information on treatment options, see: Kehlet H, Dahl JB. The value of “multimodal” or “balanced analgesia” in postoperative pain treatment. Anesth Analg. 1993;77:

34
Concept of Preemptive Analgesia
Definition Drugs Hyperlinks ไป preemptive and multimodal

35
NSAIDs, acetaminophen, nerve blocks
Multimodal Analgesia Improved Efficacy due to synergistic/additive effects Reduced doses of each analgesic May reduce severity of side effects of each drug Morphine NSAIDs, acetaminophen, nerve blocks Potentiation N/V 30% Kehlet H, Dahl JB. Anesth Analg. 1993;77:1048–1056. Jin F, Chung F. J Clin Anesth 2001;13: (Review)
")
36
Pharmacology Route & Technique

37
Sites of Action COX-2 COX-2 Koppert, et al. Pain 2004;108:148-53. 40mg

38
Yaksh, 1999 C-Terminal COX2 PG Microglia Astrocytes Endothelial
DORSAL HORN NEURON COX1 Microglia Astrocytes Endothelial MO + COX-2 > Spinal MO + LA ไม่ทำให้ชา Yaksh, 1999

39
หัวข้อที่จะเล่าให้ฟัง

40
Reuben SS, et al. Anesthesiology 2006; 104: 411-6.

41
เคยผ่าตัด Lower abdomen ปวดมาก จะมาผ่าตัด TAH ไม่อยากทำ Block หลัง
Case ผู้หญิง อายุ 45 ปี เคยผ่าตัด Lower abdomen ปวดมาก จะมาผ่าตัด TAH ไม่อยากทำ Block หลัง Diclofenac 150 mg iv.infusion ก่อนผ่าตัด Bupivacaine wound infiltration Morphine 3 mg iv q 4 h ไม่ปวด PACU 0 คะแนน Parecoxib

42
คำแนะนำสำหรับ Multimodal Analgesia
การผ่าตัดเล็ก: - ฉีดยาชารอบแผลผ่าตัดหรือทำ PNB - ให้ยาระงับปวด NSAIDs รับประทาน/ฉีด - BTP: Paracetamol, Para+codeine, tramadol การผ่าตัดระดับกลาง: - ฉีด ยาชา รอบแผลผ่าตัดหรือทำ PNB - ยาระงับปวด: NSAIDs รับประทาน/ฉีด Spinal/epidural morphine (single dose) Opioids (IV ATC, PCA)
 Opioids (IV ATC, PCA)")
43
คำแนะนำสำหรับ Multimodal Analgesia
การผ่าตัดใหญ่: - ฉีด ยาชา รอบแผลผ่าตัดหรือทำ PNB - ยาระงับปวด: NSAIDs รับประทาน/ฉีด Spinal morphine (single dose) Opioids (PCA, IV infusion, IV ATC) Continuous Epidural (bupivacaine+Opioids:PCEA)
 Opioids (PCA, IV infusion, IV ATC) Continuous Epidural (bupivacaine+Opioids:PCEA)")
44
in Post- op Pain Management
New Concepts in Post- op Pain Management Preemptive analgesia: มีอะไรใหม่? Multimodal Analgesia Pain Management by Type Specific Procedures There are many ways to effectively treat acute and chronic pain. Each of these options offers its own benefits and risks. No single option is right for every patient. NOTE: for more information on treatment options, see: Kehlet H, Dahl JB. The value of “multimodal” or “balanced analgesia” in postoperative pain treatment. Anesth Analg. 1993;77:

45
Ladder of decreasing pain intensity

46
Dahmani, et al. Br J Anaesth 2001; 87:385-9.
หัวข้อที่จะเล่าให้ฟัง Web APS Dahmani, et al. Br J Anaesth 2001; 87:385-9.

47
รายละเอียดในหนังสือที่ได้รับ NSAIDs as multimodal analgesia

48
Europe

49
ผู้ป่วยหญิง: C/S Explore Lap NSAIDs LA

50
หัวข้อบรรยาย ความสำคัญของการระงับปวด การประเมินและบันทึกความปวด
IM PRN : ทำอย่างไรให้ได้ดีกว่าเดิม เทคนิคการระงับปวดในปัจจุบัน New Concepts in PO pain management การติดตามผลการรักษา (APS)
")
51
Pain Relief and Patients’ Satisfaction
Quality of Pain Management? Pain Relief and Patients’ Satisfaction Very satisfied with pain relief mild pain (<4) Dissatisfaction with pain relief Moderate pain(>5) หัวข้อที่จะเล่าให้ฟัง Jensen MP, et al. The meaning of pain relief in a clinical trial. J Pain 2005;6(6):400-6.
 Dissatisfaction with pain relief. Moderate pain(>5) หัวข้อที่จะเล่าให้ฟัง. Jensen MP, et al. The meaning of pain relief in a clinical trial. J Pain 2005;6(6):")
52
Quality of Pain Management? 2. Pain relief vs Time
3. Pain Intensity (at rest) 4. Side effects: คลื่นไส้ อาเจียน วิงเวียน Davies, et al. BMJ 1999;319:
 4. Side effects: คลื่นไส้ อาเจียน. วิงเวียน. Davies, et al. BMJ 1999;319:")
53
Side effects related to Opioids Sedation/Respiratory Depression
-Sedation Score 2, RR> 8/min ลดขนาด bolus dose RR< 8/min ลดขนาด bolus dose, Naloxone(100 mcg) -Sedation Score 3, ไม่ต้องรอดู RR หยุด PCA, Naloxone (100 mcg, repeat PRN 0.01 mg/kg body weight for children) (infusion:200 micrograms/ml solution dose adjusted to clinical response)
 -Sedation Score 3, ไม่ต้องรอดู RR. หยุด PCA, Naloxone (100 mcg, repeat PRN mg/kg body weight for children) (infusion:200 micrograms/ml solution. dose adjusted to clinical response)")
54
Increasing analgesic response
Unconsciousness Apnea Respiratiory depression (LATE) Increased sedation Increased nausea, vomiting Base - line analgesia Opioid doses
 Increased sedation. Increased nausea, vomiting. Base - line analgesia. Opioid doses.")
55
Nausea/Vomiting อาเจียน - Anti-emetics vs Risk factors
- ลดขนาด opioids ถ้า pain score ไม่สูง - เปลี่ยนชนิด opioids - มีสาเหตุอื่นหรือไม่ - Bed rest ปวด ไม่ขอยา

57
Non-pharmacologic Interventions
Physical therapies Cognitive and behavioral therapies Application of heat or cold Distraction (auditory, visual,tactile, rhythmic) Positioning or elevation Relaxation or biofeedback External support or immobilization Guided imagery TENS or cutaneous vibration Patient teaching or preparatory information Massage Hypnosis or meditation Acupuncture or acupressure Yoga
 Positioning or elevation. Relaxation or biofeedback. External support or immobilization. Guided imagery. TENS or cutaneous vibration. Patient teaching or. preparatory information. Massage. Hypnosis or meditation. Acupuncture or acupressure. Yoga.")
58
Why? ทำไมคุณภาพการระงับปวดหลังผ่าตัดจึงไม่ดีขึ้น Pain score Year 1
Severe 10% Why?

59
Why? Pain intensity Pain at rest Khon Kaen N= 274(%) Chiang Mai
Pain intensity in orthopedic patients (post-op day one) Pain intensity Pain at rest Khon Kaen N= 274(%) Chiang Mai N= 234(%) No pain 57 (20.8) - Mild, NRS (1-3) 83 (30.3) 173 (73.9 ) Moderate, NRS (4-6) 108 (39.4) 47 (20.1) Severe, NRS 7-10 26 (9.5) 14 ( 6) Why? ความแตกต่างอยู่ที่การใช้ NSAIDs
 Pain intensity. Pain at rest. Khon Kaen. N= 274(%) Chiang Mai. N= 234(%) No pain. 57 (20.8) - Mild, NRS (1-3) 83 (30.3) 173 (73.9 ) Moderate, NRS (4-6) 108 (39.4) 47 (20.1) Severe, NRS (9.5) 14 ( 6) Why ความแตกต่างอยู่ที่การใช้ NSAIDs.")
60
คำถาม

61
http//: Prof McQuay ได้อนุญาต ให้ใช้ ข้อมูลได้แล้ว

62
->1991

64
Pain, R2R, KM,

งานนำเสนอที่คล้ายกัน













 98.08% 100.02% จังหวัด.>")









