ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
การพัฒนาคุณภาพทางคลินิก นพ.อนุวัฒน์ ศุภชุติกุล
ผู้อำนวยการสถาบันพัฒนาและรับรองคุณภาพโรงพยาบาล Surveillance Workshop_2007

2
Priority Diseases & Quality Dimension
Competency Efficient Responsive Timeliness Appropriate Effective Holistic/Humanized Safety High Risk Preg DHF Ac. Appendicitis Acute MI COPD DM Hypertension

3
All-in-One Disease Mapping
Care Process: Ac. Appendicitis Risk Prevention Monitor CQI Research Entry Initial Assessment Consultation Predictive value of US Investigation Delayed/missed diagnosis Patho. Diag. confirmed Use of clinical sign Diagnosis Planning Observation Undetected change Operation Anesthesia All-in-One Disease Mapping OR Transfer Preop Care Anesthesia Anes complication Operative Procedure Delayed operation “Door to operation” time Postanes Care Postop care & monitoring SSI SSI rate D/C plan Follow up

4
ตามรอยเพื่อการเรียนรู้ มิใช่เพื่อส่งการบ้าน
การเรียนรู้จะเกิดขึ้นได้ต่อเมื่อ มีการเก็บ & วิเคราะห์ข้อมูล มีการตั้งคำถามจากข้อมูลที่ได้ มีการค้นหาความรู้เพิ่มเติม

5
เครื่องชี้วัด การดูแลผู้ป่วยไส้ติ่งอักเสบ
Urinary tract calculi Ovarian cyst Diverticulitis Ileitis 47 48 1/49 2/49 3/49 4/49 5/49 6/49 จำนวนผู้ป่วย % ผลพยาธิวิทยาที่ไม่สนับ สนุนการวินิจฉัยทางคลินิก 12% 2% % % % % % % ระยะเวลาตั้งแต่ admit จนถึงผ่าตัด (ชม:นาที) 5: : : : : : : :47 จำนวนผู้ป่วยที่ผ่าตัดหลัง admit เกิน 6 ชั่วโมง 0% % 0% % % 0% % % อัตราการติดเชื้อแผลผ่าตัด เสนอให้ใช้ US มาช่วยในการ investigation เพิ่มเติม
 5:51 4:30 2:50 6:27 6:18 6:33 4:34 8:47. จำนวนผู้ป่วยที่ผ่าตัดหลัง. admit เกิน 6 ชั่วโมง % 0.7% 0% 0% 0% 0% 0% 14% อัตราการติดเชื้อแผลผ่าตัด. เสนอให้ใช้ US มาช่วยในการ investigation เพิ่มเติม.")
6
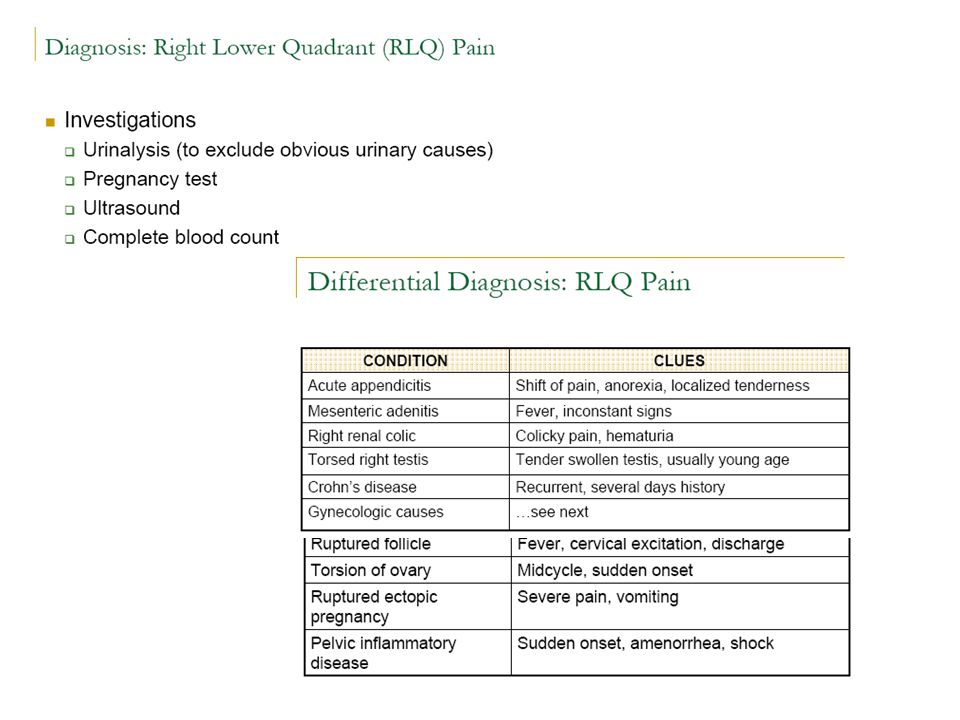
บทเรียน คุณภาพที่ได้จากการวินิจฉัยที่ถูกต้อง อาจจะทำให้เวลาที่ผู้ป่วยควรจะได้รับการผ่าตัดช้าลงไป ขณะเดียวกัน การผ่าตัดในผู้ป่วยที่ยังไม่วินิจฉัยได้แน่นอนหรือผิดพลาดในกลุ่ม high risk ก็จะทำให้อันตายยิ่งสูงมากขึ้น เช่น เกิด septic shock ใน UTI จาก ureteric stone การตรวจวินิจฉัยปกติ เช่น UA, KUB เป็น invetigation ที่ทำได้ง่าย แต่มีประโยชน์ในการวินิจฉัยโรคทาง urinary tract caluculi หรือ infection ได้ ระบบที่จะช่วยในการดูแลรักษาให้ได้ผลดี ได้แก่ การเฝ้าระวังอาการ การตรวจ US ในเวลาที่เหมาะสม

7
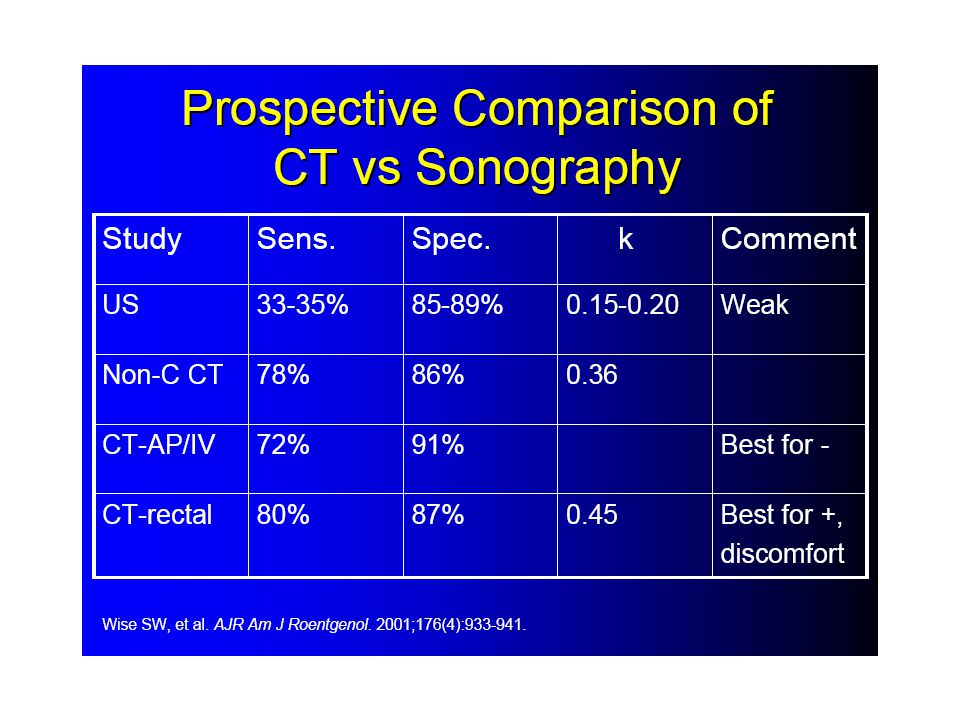
Predictive Value ของการตรวจ US ในผู้ป่วยไส้ติ่งอักเสบ
จากการตามรอยผลลัพธ์ของ รพ. Sensitivity = 17/32 = 53% Specificity = 3/3 = 100%

9
Diagnosis of Acute Appendicitis
Mesenteric Adenitis Acute appendicitis is one of the most common surgical emergencies Incidence: 60-80/100,000 yrs Male=Female Mortality 1%(unperforated) ~5%(perforated) Mainly clinical diagnosis: Some CT/US used in unequivocal cases. Mimicker of Appendicitis May be proceeded by “flu like illness” Children > Adults Diffuse abdominal pain > RIF pain High temp >38.5oC (appendicitis = <38.5oC) But can be indistinguishable from appendicitis. Diagnosis is often made on Laproscopy / Laparotomy
 ~5%(perforated) Mainly clinical diagnosis: Some CT/US used in unequivocal cases. Mimicker of Appendicitis. May be proceeded by flu like illness Children > Adults. Diffuse abdominal pain > RIF pain. High temp >38.5oC (appendicitis = <38.5oC) But can be indistinguishable from appendicitis. Diagnosis is often made on Laproscopy / Laparotomy.")
10
Can US visualise the diseased appendix?
Study: Yonsei University College of medicine, Korea. Using: Meta Analysis of 22 articles between (2643 patients)
")
13
Use of a modified Alvorado score in the diagnosis of acute appendicitis.
Saidi HS, Chavda SK. Department of Human Anatomy, College of Health Sciences, University of Nairobi, P.O Box 30197, Nairobi, Kenya. BACKGROUND: The negative appendicectomy rates have remained high. The integration of clinical scores into the diagnostic process in acute appendicitis has had the purposes of improving decision making and reducing the negative rates in this common condition. The performance of these score systems have however, not been uniform. OBJECTIVE: To assess the usefulness of a modified Alvorado score (1986) to predict groups of patients with suspected appendicitis for definite surgery, observation or discharge from hospital. DESIGN: Prospective study. SETTING: Kenyatta National Hospital (KNH), a central referral and teaching hospital in Nairobi, Kenya. PATIENTS: One hundred and eighty nine patients with suspected acute appendicitis were studied over a period of twelve months. METHODS: Five symptoms and four signs were assigned numerical values and the patients scored out of a total of 10 points. A score of >7 predicted mandatory operation, 5-6 observation and score 1-4 predicted those not considered for surgery. The decision to operate was the prerogative of the surgeon or surgical resident based on overall clinical suspicion and not the diagnostic score. RESULTS: The proportion of patients with scores >7 was 40.7%. The mean score was The mean ages and the gender ratios were similar across score groups. The negative appendicectomy rate was 17.6% for group 1-4, 16.5% for 5-6 and 19.7% for >7. These were similar to the overall negative rate of 18% based on clinical suspicion. The overall sensitivity and sensitivity for the scoring system was 80.3% and 16.8% respectively. CONCLUSION: High scores were found to perform poorly in predicting diagnosis of acute appendicitis preoperatively and in the reduction of negative appendicectomies. The integration of a scoring system does not offer advantage over degree of clinical suspicion. PMID: [PubMed - indexed for MEDLINE]
 to predict groups of patients with suspected appendicitis for definite surgery, observation or discharge from hospital. DESIGN: Prospective study. SETTING: Kenyatta National Hospital (KNH), a central referral and teaching hospital in Nairobi, Kenya. PATIENTS: One hundred and eighty nine patients with suspected acute appendicitis were studied over a period of twelve months. METHODS: Five symptoms and four signs were assigned numerical values and the patients scored out of a total of 10 points. A score of >7 predicted mandatory operation, 5-6 observation and score 1-4 predicted those not considered for surgery. The decision to operate was the prerogative of the surgeon or surgical resident based on overall clinical suspicion and not the diagnostic score. RESULTS: The proportion of patients with scores >7 was 40.7%. The mean score was The mean ages and the gender ratios were similar across score groups. The negative appendicectomy rate was 17.6% for group 1-4, 16.5% for 5-6 and 19.7% for >7. These were similar to the overall negative rate of 18% based on clinical suspicion. The overall sensitivity and sensitivity for the scoring system was 80.3% and 16.8% respectively. CONCLUSION: High scores were found to perform poorly in predicting diagnosis of acute appendicitis preoperatively and in the reduction of negative appendicectomies. The integration of a scoring system does not offer advantage over degree of clinical suspicion. PMID: [PubMed - indexed for MEDLINE]")
15
การพัฒนาคุณภาพที่ได้ผล ยึดเป้าหมาย หลากหลายวิธีพร้อมกัน ไม่ติดรูปแบบ
ใช้เป็นกรอบเพื่อตามรอยกระบวนการพัฒนาคุณภาพ KPI Monitoring ติดตามเครื่องชี้วัดสำคัญ จุดประกายสร้างสรรค์ มาช่วยกันดูหลายๆ มุม Creativity & Innovation Multidisciplinary Team เป้าหมาย การดูแลผู้ป่วย ศึกษาจากผู้เยี่ยมยุทธ์ รุมดูแลแบบองค์รวม Benchmarking Holistic Care How can we get more benefits from these improvement concept and tools? การพัฒนาคุณภาพที่จะให้ประโยชน์สูงสุด ควรนำเครื่องมือและแนวคิดการพัฒนาคุณภาพหลายๆ วิธีมาใช้พร้อมๆ กัน ซึ่งจะก่อให้เกิดความสมดุล เช่น สมดุลระหว่างการใช้ข้อมูลวิชาการ (เน้นทางด้านเทคนิค) กับการดูแลแบบองค์รวม (เน้นด้านจิตวิญญาณ) สมดุลระหว่างการทบทวนจุดอ่อนของตนเอง (จากอุบัติการณ์ บันทึก ข้างเตียง) กับการเรียนรู้สิ่งดีๆ ของคนอื่น (benchmarking) การตามรอยกระบวนการพัฒนาคุณภาพ นอกจากจะช่วยสรุปบทเรียนของความสำเร็จแล้ว ยังช่วยให้เห็นว่ายังมีเครื่องมือและแนวคิดใดอีกบ้างที่สามารถนำมาใช้ประโยชน์เพิ่มขึ้น เจาะจุดอ่อนจากข้างเตียง/บันทึก สวมความรู้วิชาการ Bedside/Medical Record Review Evidence-based Practice ใช้อุบัติการณ์มาวิเคราะห์ Root cause Analysis from Incidence Surveillance Workshop_2007
 กับการดูแลแบบองค์รวม (เน้นด้านจิตวิญญาณ) สมดุลระหว่างการทบทวนจุดอ่อนของตนเอง (จากอุบัติการณ์ บันทึก ข้างเตียง) กับการเรียนรู้สิ่งดีๆ ของคนอื่น (benchmarking) การตามรอยกระบวนการพัฒนาคุณภาพ นอกจากจะช่วยสรุปบทเรียนของความสำเร็จแล้ว ยังช่วยให้เห็นว่ายังมีเครื่องมือและแนวคิดใดอีกบ้างที่สามารถนำมาใช้ประโยชน์เพิ่มขึ้น. เจาะจุดอ่อนจากข้างเตียง/บันทึก. สวมความรู้วิชาการ. Bedside/Medical Record Review. Evidence-based Practice. ใช้อุบัติการณ์มาวิเคราะห์ Root cause Analysis from Incidence. Surveillance Workshop_2007.")
16
ใช้ตัวตามรอยทางคลินิก (Clinical Tracer)
เพื่อเรียนรู้และพัฒนาทุกองค์ประกอบในระบบงาน Quality Process บริบท ประเด็นสำคัญ 1. ตามรอยกระบวนการพัฒนา Content วัตถุประสงค์ 2. ตามรอยกระบวนการดูแลผู้ป่วย Integration 3. ตามรอยระบบอื่นๆ ที่เกี่ยวข้อง Result สิ่งดีๆ ที่มีอยู่ โอกาสพัฒนา ตัวชี้วัด ติดตามผลลัพธ์ ตัวตามรอยทางคลินิก (Clinical Tracer) เป็นการประมวลเครื่องมือและแนวคิดการพัฒนาคุณภาพที่มีอยู่แล้ว มาใช้พร้อมๆ กันสำหรับผู้ป่วยกลุ่มเดียวกัน ทำให้สามารถต่อยอดจากการทบทวนผู้ป่วยเป็นรายๆ สู่การพัฒนาที่เป็นระบบและครอบคลุมในทุกองค์ประกอบ การตามรอยทางคลินิก ทำให้สามารถประเมินการนำมาตรฐานมาสู่การปฏิบัติที่เป็นรูปธรรมได้ชัดเจนยิ่งขึ้น การพัฒนาคุณภาพ การดูแลผู้ป่วย กรอบที่จะช่วยให้เกิดการคิดอย่างเชื่อมโยงและเป็นระบบ Surveillance Workshop_2007
 เป็นการประมวลเครื่องมือและแนวคิดการพัฒนาคุณภาพที่มีอยู่แล้ว มาใช้พร้อมๆ กันสำหรับผู้ป่วยกลุ่มเดียวกัน. ทำให้สามารถต่อยอดจากการทบทวนผู้ป่วยเป็นรายๆ สู่การพัฒนาที่เป็นระบบและครอบคลุมในทุกองค์ประกอบ. การตามรอยทางคลินิก ทำให้สามารถประเมินการนำมาตรฐานมาสู่การปฏิบัติที่เป็นรูปธรรมได้ชัดเจนยิ่งขึ้น. การพัฒนาคุณภาพ. การดูแลผู้ป่วย. กรอบที่จะช่วยให้เกิดการคิดอย่างเชื่อมโยงและเป็นระบบ. Surveillance Workshop_2007.")
17
Implementation (Delivery of Care)
Care Process: Ac. Appendicitis Care Process: A Simple Starting Model Entry Entry Initial Assessment Consultation Assessment Investigation Diagnosis Planning Planning Observation Operation Medicine Operation/Anes Nutrition Rehabilitation Education Anesthesia Implementation (Delivery of Care) OR Transfer Preop Care Anesthesia Evaluation Operative Procedure Postanes Care D/C & Follow UP Postop care & monitoring D/C plan Follow up
 OR. Transfer. Preop Care. Anesthesia. Evaluation. Operative Procedure. Postanes Care. D/C & Follow UP. Postop care & monitoring. D/C plan. Follow up.")
18
Implementation (Delivery of Care)
Care Process: Assessment Entry Initial Assessment Assessment Consultation Investigation Planning Diagnosis Implementation (Delivery of Care) Evaluation D/C & Follow UP
 Evaluation. D/C & Follow UP.")
19
Implementation (Delivery of Care)
Care Process: Planning Entry Uncertain need Care need at hospital Care need at home Assessment Further Investigation Planning Planning Observation Care Plan Discharge Plan Medicine Surgery/Anes Nutrition Rehabilitation Education Psychosocial Monitoring Etc. Self care Care giver Environment Rehabilitation Behavior modification Etc. Implementation (Delivery of Care) Evaluation D/C & Follow UP
 Evaluation. D/C & Follow UP.")
20
Implementation (Delivery of Care)
Care Process: Implementation (Delivery of Care) Entry Assessment Planning Safety precaution Medicine Operation/Anes Nutrition Rehabilitation Education Emergency response Implementation (Delivery of Care) Psychosocial care Care as planned Evaluation Communication Coordination Consultation D/C & Follow UP
 Entry. Assessment. Planning. Safety precaution. Medicine. Operation/Anes. Nutrition. Rehabilitation. Education. Emergency response. Implementation. (Delivery of Care) Psychosocial care. Care as planned. Evaluation. Communication. Coordination. Consultation. D/C & Follow UP.")
21
Implementation (Delivery of Care)
Care Process: Evaluation Entry Assessment Planning Implementation (Delivery of Care) Safety precaution Evaluate Safety / M&M Emergency response Evaluate Responsiveness Psychosocial care Evaluate Psychosocial care Evaluation Care as planned Evaluate Goal Achievement Communication Coordination Consultation Evaluate Team Effectiveness D/C & Follow UP
 Safety precaution. Evaluate Safety / M&M. Emergency response. Evaluate Responsiveness. Psychosocial care. Evaluate Psychosocial care. Evaluation. Care as planned. Evaluate Goal Achievement. Communication. Coordination. Consultation. Evaluate Team Effectiveness. D/C & Follow UP.")
22
All-in-One Disease Mapping
Care Process: Ac. Appendicitis Risk Prevention Monitor CQI Research Entry Initial Assessment Consultation Predictive value of US Investigation Delayed/missed diagnosis Patho. Diag. confirmed Use of clinical sign Diagnosis Planning Observation Undetected change Operation Anesthesia All-in-One Disease Mapping OR Transfer Preop Care Anesthesia Anes complication Operative Procedure Delayed operation “Door to operation” time Postanes Care Postop care & monitoring SSI SSI rate D/C plan Follow up

23
ลำดับชั้นของเอกสาร: ทำให้น้อยที่สุด
All-in-One Disease Mapping Risk Prevention Guide Clinical Tracer Forms CPGs CareMaps CQIs Indicators

24
กิจกรรมกลุ่ม “ภาพเดียว เข้าใจทุกเรื่อง” (All-in-One Disease Mapping)
เขียน Patient Care Process ตามแนวทางในตัวอย่าง ให้ครอบคลุมกระบวนการของทุกสาขาวิชาชีพที่เกี่ยวข้อง (20 นาที) ระบุความเสี่ยงทางคลินิกที่สำคัญในแต่ละขั้นตอน (10 นาที) ระบุมาตรการป้องกันความเสี่ยงดังกล่าวโดยสังเขป (15 นาที) อาจจะแบ่งงานกันทำ และเขียนแยกในกระดาษแผ่นเล็กๆ ระบุตัวชี้วัดที่สมควร monitor ในขั้นตอนต่างๆ และผลลัพธ์ของการดูแล ระบุกิจกรรมพัฒนาคุณภาพที่ทีมงานได้เคยทำมาแล้ว ว่าเกี่ยวข้องกับขั้นตอนใดในการดูแลผู้ป่วย ระบุการใช้ข้อมูลวิชาการ / guideline หรือการสร้างผลงานวิจัย พิจารณาว่าจะทำให้สมาชิกของทีมงานทุกคนเข้าใจประเด็นคุณภาพที่สำคัญในขั้นตอนต่างๆ ของการดูแลผู้ป่วย และร่วมกันสร้างคุณภาพการดูแลผู้ป่วยได้อย่างไร
 ระบุความเสี่ยงทางคลินิกที่สำคัญในแต่ละขั้นตอน (10 นาที) ระบุมาตรการป้องกันความเสี่ยงดังกล่าวโดยสังเขป (15 นาที) อาจจะแบ่งงานกันทำ และเขียนแยกในกระดาษแผ่นเล็กๆ. ระบุตัวชี้วัดที่สมควร monitor ในขั้นตอนต่างๆ และผลลัพธ์ของการดูแล. ระบุกิจกรรมพัฒนาคุณภาพที่ทีมงานได้เคยทำมาแล้ว ว่าเกี่ยวข้องกับขั้นตอนใดในการดูแลผู้ป่วย. ระบุการใช้ข้อมูลวิชาการ / guideline หรือการสร้างผลงานวิจัย. พิจารณาว่าจะทำให้สมาชิกของทีมงานทุกคนเข้าใจประเด็นคุณภาพที่สำคัญในขั้นตอนต่างๆ ของการดูแลผู้ป่วย และร่วมกันสร้างคุณภาพการดูแลผู้ป่วยได้อย่างไร.")
งานนำเสนอที่คล้ายกัน









>")



>")





