ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Recommendations for Infection Control for the Practice of Anesthesiology
Developed by the ASA Committee on Occupational Health Task Force on Infection Control (Third Edition) Good morning, I’m Dr.จิตสุภา ปริชาตปรีชา I’m here with. Dr.ประไพรัตน์ เหมราช And my adviser is อาจารย์ขัตติยา มโนมยางกูร Today, we would like to present a topic review about infectious control in operating room. Reference form ASA committee on Occupational Health Task Force R2 Chitsupha Parichatpricha R2 Prapairat Hemmaraj Aj Kattiya Manomayangkul
 Good morning, I’m Dr.จิตสุภา ปริชาตปรีชา. I’m here with. Dr.ประไพรัตน์ เหมราช. And my adviser is อาจารย์ขัตติยา มโนมยางกูร. Today, we would like to present a topic review about infectious control in operating room. Reference form ASA committee on Occupational Health Task Force. R2 Chitsupha Parichatpricha. R2 Prapairat Hemmaraj. Aj Kattiya Manomayangkul.")
2
Prevention of Healthcare-Associated Infection in Patients
Prevention of Occupational Transmission of Infection to Anesthesiologists We divide to two topics. First, prevention of Healthcare-Associated Infection in Patients. Second, prevention of Occupational Transmission of Infection to Anesthesiologists.

3
Prevention of Healthcare-Associated Infection in Patients
A. Hand Hygiene B. Preventing Contamination of Medications C. Prevention of Surgical Site Infection The things that we should to do in this section are hand hygiene, preventing Contamination of Medications and Surgical Site Infection.

4
Prevention of Healthcare-Associated Infection in Patients
D. Prevention of Intravascular Catheter-Related Infection E. Prevention of Infection Associated with Neuraxial Procedures And the prevention of Intravascular Catheter-Related Infection, neuraxial procedures.

5
PREVENTION OF HEALTHCARE-ASSOCIATED INFECTION IN PATIENTS

6
A. Hand Hygiene In this picture, Indications for hand hygiene:
Number1 and 4-Before and after direct contact with patients. 2-Before clean or aseptic procedure example before donning sterile gloves. 3-After contact with body fluids, non-intact skin, mucous membranes or wound dressings. 5-After contact with high-touch environmental surfaces surroundings patient. And other indications are after removal gloves, before eating and after using the restroom.

7
Hand washing This is step for hand washing.
First, we rub palm to palm, ……….and dry your hand. Don’t forget to wash – between your finger , under your nails and the tops of your hands.

8
You will see the picture that the red and orange areas are most frequently missed during hand washing.

9
This’s hand hygiene algorithm
This’s hand hygiene algorithm. If your hand or gloves contaminated, is there adequate time to perform hand hygiene and reglove? If no, we should remove gloves and use gel hand.

10
What germs are on your hands?
So handwashing is the single most important thing you can do to stop the spread of infection.

11
Next slide, we can use alcohol, 2-4% chlorhexidine and iodine compound for hand-hygiene antiseptic agents. Especially, alcohol and iodine , they’re excellent for disinfection.

12
This study is talk about “Hand hygiene behaviors and taxonomize failures in anesthesia providers.
In department of Anesthesiology, Medical Center, Virginia.

13
Methods: Following 5 observers pose as nursing staff in an academic center observed the Hand-hygeine of anesthesia providers 4-week period throughout the perioperative period The methods is Following 5 observers pose as nursing staff in an academic center, observed the HH of anesthesia providers over 4-week throughout the perioperative period. HH opportunities and HH failures were recorded and categorized. Conclusion revealed in this study that the HH and aseptic practices of anesthesia providers, were very poor.

14
B. Preventing Contamination of Medications and Fluids
Safe Injection Practices Aseptic technique Category IA Aseptic technique is a procedure used by medical staff to prevent the spread of infection. The goal is to reach asepsis. In this topic, we use aseptic technique to avoid contamination of sterile injection equipment Category IA: Strongly recommended and strongly supported by well-designed and experimental studies.

15
2. Syringes, needles and cannulae Category IA
-Needles, cannulae and syringes are sterile, single-use items do not reuse for another patient. -And do not administer medications from a syringe to multiple patients, though the needle or cannula on the syringe is changed. -Such as a Dormicum syringe that we use in our operating room. It should not to do like this.

16
3. Single-dose vials (SDVs) Category IA
-Single-dose vials – If possible we should to use a single-dose vials for parenteral medications than a multidose vials. -And do not administer medications from ampules to multiple patients or leftover contents for later use. - If MDVs must be used both the needle or cannula and syringe must be sterile. - Discard if sterility is questionable. 4. Multi-dose vials (MDVs) Category IA
 Category IA.")
17
5. Fluid infusion and administration sets (i. e
5. Fluid infusion and administration sets (i.e. intravenous bags, tubing, and connectors) Category IB - Fluid infusion and administration sets for example intravenous bags, tubing, and connectors - We should use for 1 patient only and do not use for multiple patients. Category IB: Strongly recommended and supported by some experimental.
 Category IB - Fluid infusion and administration sets for example intravenous bags, tubing, and connectors. - We should use for 1 patient only and do not use for multiple patients. Category IB: Strongly recommended and supported by some experimental.")
18
Medication and Fluid Use in the Immediate Patient Treatment
- All medications and fluids are single-patient-use only. - Use appropriate aseptic technique and hand hygiene including use an alcohol swab to cleanse the vial's rubber septum before entering. - Cleanse the neck of glass ampules with an alcohol swab and let dry before opening.

19
- Syringes should be capped when not in use.
- Discard all used or opened medication/fluid containers (e.g., cap off, bag entered). - Opened single-dose ampules must be immediately discarded and not be stored for any time period. - Discard used needles in a sharps container. - Store unused syringes, needles and related items in a clean areas.
. - Opened single-dose ampules must be immediately discarded and not be stored for any time period. - Discard used needles in a sharps container. - Store unused syringes, needles and related items in a clean areas.")
20
This study is talk about “Reduction in Intraoperative Bacterial Contamination of Peripheral Intravenous Tubing Through the Use of a Novel Device” It was studied in department of Anesthesiology, Dartmouth-Hitchcock Medical Center, Lebanon

21
Method: The study was divided 2 group, control and device group from enrolled one hundred fourteen operative cases. Two sites on the anesthesia machine were selected, decontaminated and cultured via aseptic technique These sites and the peripheral intravenous stopcock were cultured again after completion of the surgery. Conclusions: Improved hand hygiene compliance by using a novel device can reduces the risk of intraoperative bacterial transmission.

22
The Sprixx GJ device (Harbor Medical Inc., Santa Barbara, CA)
This is a novel hand sanitation device. Alcohol-based cleanser deployed by squeezing device Device worn by provider The Sprixx GJ device (Harbor Medical Inc., Santa Barbara, CA)
")
23
C. Prevention of Surgical Site Infections
Glucose control Hair removal Nicotine use Preoperative Considerations Hair removal - Do not remove hair preoperatively unless the hair around the incision site. If necessary, remove immediately before the operation, preferably with electric clippers. Glucose control - Consider control serum blood glucose levels in all diabetic patients and avoid perioperative hyperglycemia. Especially, more than 200 mg/dL has been associated with increased SSI risk. Nicotine use - tobacco cessation for at least 30 days before elective operation. Smoking is a risk factor. Transfusion – is not associated with SSI. Antiseptic shower - Require patients to shower with an antiseptic agent on the night prior to surgery with povidone-iodine or chlorhexidine gluconate. Antimicrobial prophylaxis - Administer agent only when indicated and prior to incision. In order to, bactericidal concentration of the drug is present in the serum and tissues at the time of incision and maintain therapeutic levels throughout the operation. Transfusion Antiseptic shower Antimicrobial prophylaxis

24
C. Prevention of Surgical Site Infections
Operating Room Ventilation Cleaning Normothermia Intraoperative Considerations Operating Room Ventilation - Maintain positive-pressure ventilation in the operating room and adjacent areas. Keep OR doors closed except as needed. Cleaning - Use disinfectant to clean affected areas before the next operation. Asepsis and surgical technique - is the foundation of prevention. Normothermia – If core temperature less than 36 C has been associated with an increased risk by causing vasoconstriction, decreased oxygen delivery to the wound space and impaired phagocytic leukocyte function. Surgical attire - Wear a surgical mask, a cap or hood that fully covers hair on the head throughout the operation. Surgical attire Asepsis and surgical technique

25
C. Prevention of Surgical Site Infections
Postoperative Considerations Postoperative Incision Care - Wash hands before and after dressing changes and any contact with the surgical site. Postoperative Incision Care

26
D. Prevention of Intravascular Catheter-Related Infections
General Considerations 1. Hand hygiene 2. Aseptic technique 3. Catheter site care 4. Dressing regimens 5. Replacement of administration sets Intravascular catheters are an essential part of patient care for anesthesiologists. Although these catheters provide necessary vascular access, we put patients at risk for local and systemic infectious complications. The recommendations are based on guidelines published by the Centers for Disease Control (CDC). It compose of general considerations such as hand hygiene, aseptic technique, catheter site care, dressing regimens and replacement of administration sets.
. It compose of general considerations such as hand hygiene, aseptic technique, catheter site care, dressing regimens and replacement of administration sets.")
27
- Sterile gloves should be worn for insertion of arterial and central catheters. Maximal sterile barrier precautions during insertion of arterial and central venous catheters (CVC) reduces the incidence of catheter-related bloodstream infections (CRBSI) - Catheter site care - Disinfect clean skin with an appropriate antiseptic before catheter insertion, preferably with a 2% chlorhexidine-based preparation

28
- Dressing regimens - Cover catheter site with sterile gauze or sterile transparent, semipermeable dressing and do not routinely apply topical antimicrobial ointment to the insertion site (except with dialysis catheters). - Replacement of administration sets –No more frequently than 72-hour intervals unless catheter-related infection is suspected. Should use of 70% alcohol or an iodofor before accessing the system reduces microbial contamination of vascular catheter hubs.

30
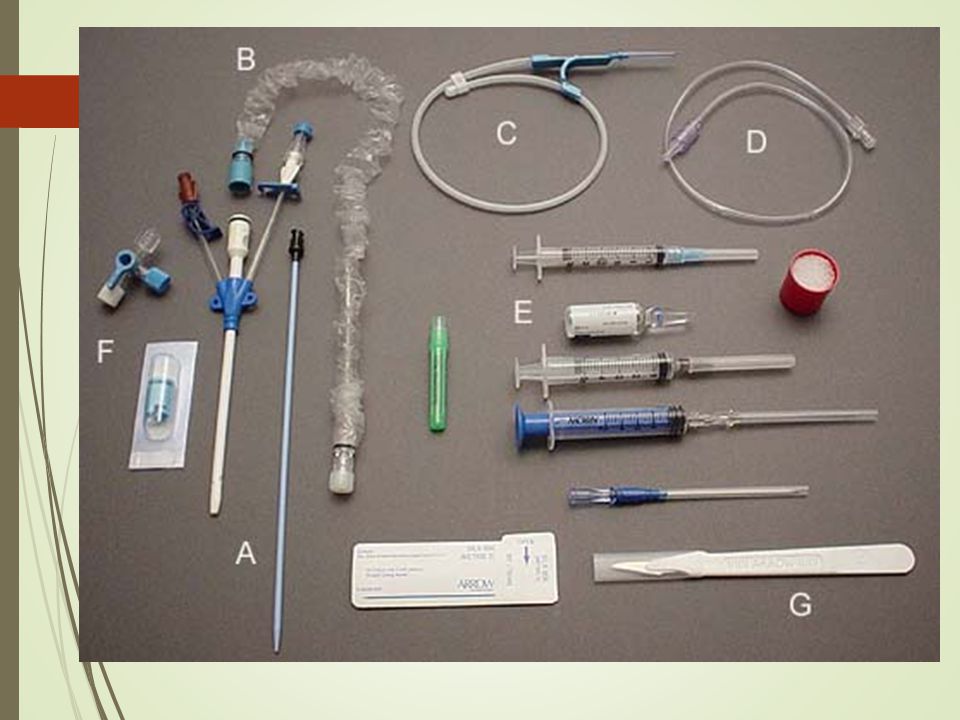
Central Venous Catheters 1. Catheter selection 2. Insertion
iii. Central Venous Catheters 1. Catheter selection 2. Insertion 3. Barrier precautions 4. Catheter replacement 5. Pressure transducers 6. Catheter site dressing Central Venous Catheters compose of - Catheter selection - Use an antimicrobial or antiseptic-impregnated CVC for catheters anticipated to remain in place >5 days in facilities. - Insertion - non-tunneled CVC and internal jugular vein insertion is less common mechanical complications. - Catheter replacement – use a guidewire exchange to replace a malfunctioning, non-tunneled, non-infected CVC or to exchange a catheter. - Pressure transducers - Used continuous flush devices and disposable transducers reduced the risk of infection.

31
E. Prevention of Infection Associated with Neuraxial Procedures
-Although infectious complications of neuraxial anesthesia (predominantly epidural abscess and meningitis) are rare but they’re serious sequelae.
 are rare but they’re serious sequelae.")
32
epidural abscess 1 : 145,000 Meningitis 0.2 -1.3 : 10,000
Post-dural puncture meningitis manifests 6-36 hours after dural puncture symptoms : fever, back pain/tenderness and radicular pain leading to weakness and paralysis The estimated incidence of epidural abscess is 1 in 145,000 (one in one hundred forty-five thousand) - while the incidence of meningitis is 0.2 to 1.3 per 10,000 (zero point two to one point three per ten thousand) - Post-dural puncture meningitis typically manifests between 6 and 36 hours after dural puncture The presenting symptoms are typically fever, back pain/tenderness and radicular pain leading to weakness and paralysis.
 - while the incidence of meningitis is 0.2 to 1.3 per 10,000 (zero point two to one point three per ten thousand) - Post-dural puncture meningitis typically manifests between 6 and 36 hours after dural puncture. The presenting symptoms are typically fever, back pain/tenderness and radicular pain leading to weakness and paralysis.")
33
Summary of Advisory Statements
Summary Advisory Statements of neuraxial procedures These include: - Removal of jewelry - Hand washing- Hand hygiene with alcohol-based hand gel. - Wear cap, mask, sterile gloves - Use of individual packets of antiseptic skin preparation (preferably a chlorhexidine/alcohol solution). -Sterile drape. -Sterile/ occlusive dressing over catheter site. -Consider in-line bacterial filter for extended infusions. -Limit the number of disconnections of the catheter/ infusion system. -Remove catheter as soon as no longer clinically necessary.
. -Sterile drape. -Sterile/ occlusive dressing over catheter site. -Consider in-line bacterial filter for extended infusions. -Limit the number of disconnections of the catheter/ infusion system. -Remove catheter as soon as no longer clinically necessary.")
34
Prevention of Occupational Transmission of Infection to Anesthesiologists
The next part I will talk is about prevention of occupational transmission of infection to anesthesiologists

35
Prevention of Occupational Transmission of Infection to Anesthesiologists
Needlestick/Sharps Safety Transmission-based Precautions Bloodborne Pathogens (hepatitis B virus, hepatitis C virus, human immunodeficiency virus) Tuberculosis (TB) And these are scopes of my topic section. …
 Tuberculosis (TB) And these are scopes of my topic section. …")
36
Needle stick/Sharps Safety
Since we have to work in OR. Everyday we expose with sharp equipment such as needle ,blades, including lots of pathogen. Exposure to many kinds of patients. That means nowsday we take risks of danger from needle stick and infections. So the prevention of infection is very important.

37
Needleless device needleless intravenous access systems
In prevention of accidental needle stick you should use the needleless device or devices with autosafety This is the needleless intravenous access system You should handle device in safety manner needleless intravenous access systems

38
Devices with safety protection features
This is the self – sheathing needles and the scalpels with safety-activated blade covers scalpels with safety-activated blade covers self-sheathing needles

39
Devices with safety protection features
This is the syringe with a retractable needles And the safety intravenous catheters Syringe with a Retractable Needle safety intravenous catheters

40
1-handed technique Avoid recapping but if necessary you should do with one hand technique

41
Sharp disposal container
After using the sharp device you shouldn’t bend or break it , You have to put it in the hard ,not leaked container The container should place near you It should be sealed and replaced before completely filled Puncture-resistant, leak-proof containers located closely ,sealed and replaced before completely filled

42
Mode of transmission Direct contact transmission
Blood , secretion, mucous membrane Indirect contact transmission Enviromental surface, clothing Droplet transmission Coughs, sneezes, talks, sings,intubation,suctioning Airborne transmission Droplet nuclei (<= 5 micron) The prevention of infection bases on mode of transmission There are four classes include Direct contact transmission : This is the transmission of an infectious agent directly from one person to another. This occurs when you touch the blood or secretion of the infected patient Indirect contact transmission : the infectious agent is transmitted via intermediate object such as environmental surface or clothing Droplet transmission: This is a specific type of contact transmission,Droplets are more than five micron in size and formed when a person cough,sneezed,talks,sings ,during intubation and suctioning. Droplet can remain in air with short period ,and 3 feet far away from where they are generated Airborne transmission: This occurs with organism that very small,less than five micron in sizes such asTB ,it can spread and remain in the air longer than the droplets
 The prevention of infection bases on mode of transmission. There are four classes include. Direct contact transmission : This is the transmission of an infectious agent directly from one person to another. This occurs when you touch the blood or secretion of the infected patient. Indirect contact transmission : the infectious agent is transmitted via intermediate object such as environmental surface or clothing. Droplet transmission: This is a specific type of contact transmission,Droplets are more than five micron in size and formed when a person cough,sneezed,talks,sings ,during intubation and suctioning. Droplet can remain in air with short period ,and 3 feet far away from where they are generated. Airborne transmission: This occurs with organism that very small,less than five micron in sizes such asTB ,it can spread and remain in the air longer than the droplets.")
43
Isolation precautions
Standard precautions Transmission-based precautions Isolation precaution can be divided into standard precautions and transmission base precautions Standard precautions are work practice for prevention of infectious transmission in suspected case or in case with no definite diagnosis of infectious disease Transmission base precautions prevent the spread of infectious diseases in patients who have the definite diagnosis and route of transmission Airborne precaution Droplet precaution Contact precaution

44
So the Standard precautions are applied for all patients
These practice reduce the risk of transmission of infectious agents from patient to patient, patient to HCW or HCW to patient It’s a simple and effective way to control infection include Perform Hand washing before and after contact to the patient and after removal of gloves Wear gloves when u will contact with blood, body fluids (except sweat), non-intact skin, and mucous membranes. Use PPE : Wear Gown, face, and eye protection if there is a risk of splash or spray. Use a standard surgical mask when inserting a central line or performing neuraxial anesthesia. Perform Needle and sharp safety Decontaminate of equipment Safe handling of Waste Safe handling of contaminated linen Environmental cleaning
, non-intact skin, and mucous membranes. Use PPE : Wear Gown, face, and eye protection if there is a risk of splash or spray. Use a standard surgical mask when inserting a central line or performing neuraxial anesthesia. Perform Needle and sharp safety. Decontaminate of equipment. Safe handling of Waste. Safe handling of contaminated linen. Environmental cleaning.")
45
Contact precautions Contact precautions are used when the Infectious agents can spread by direct or indirect contact such as VRE,MRSA, ESWL, SARS-CoV viral/bacterial conjunctivitis, Or bacterial that cause impetigo, severe abscess, NF

46
Standard precautions and Private 3 feet between patients
Signage outside room Gown and glove Face and eye protection Remove gloves and gown before exiting room. Avoid self-contamination Perform hand hygiene after removal of PPE. Dedicated patient equipment Clean equipment prior to its use with other patients. Cleaning of room Maintain transport and entire perioperative period. Communicate Contact precautions include Standard precaution and separate the patient but If it is not possible ,the patient can be admited with roommates that have the same infectious agent,and the patient should be placed far away form each other at least3 feet Wear gown and gloves when caring for patients Perform hand hygiene after removing gown and/or gloves. Minimize sharing of equipment. Appropriately clean equipment before use with other patients. Appropriate cleaning of room when vacated. Maintain contact precautions during transport and entire perioperative period. Communicate precaution level to those who will receive patient postoperatively

47
Droplet precautions mumps pertussis diphtheria Rubella=German measles
Droplet precautions are practice for prevention of Infectious disease that spread via droplet such as Influenza, Bird flu SARS-CoV Mumps, Rubella Pertussis Diptheria Rubella=German measles diphtheria

48
HCWs surgical mask, gloves, gown, and eye protection
Single 3 feet. HCWs surgical mask, gloves, gown, and eye protection Patient standard mask Respiratory hygiene/cough etiquette. Communicate precaution level If you have to contact with these patient you should do droplet precaution include Standard precaution and Admit pt in Single room ,or with existing roommate when necessary but separate at least 3 feet between each pt Signage “ Droplet precaution” outside room to indicate level of precautions. HCWs should wear standard surgical mask, gloves, gown, and eye protection Patient should wear standard mask (if tolerated) when transport outside room Respiratory hygiene/cough etiquette. Maintain precautions throughout perioperative period. Communicate precaution level to those who will receive patient postoperatively.
 when transport outside room. Respiratory hygiene/cough etiquette. Maintain precautions throughout perioperative period. Communicate precaution level to those who will receive patient postoperatively.")
49
movie Such a long period of topic, someone are bored, someone fall asleep. I think I should break with this interesting movie. Let’s see. … What s a thrilling movie !! Prapairat Yes this is a movie about infectious agent that could spread by many modes. It spreaded shortly and killed so many people worldwide. The ways to stop it were airborne precaution and contact precaution. Like the SARS which used to be contagious 10 years ago. So infectious control is very improtant.

50
Airborne precaution Measles Chicken pox Well, come back to the topic.
The next is airbourne precaution. It’s used for preventing infectious agents that can spread via air include TB , measles, chicken pox, SARS-CoV Chicken pox

51
Airborne infectious isolation room(AIIR) N95 for HCW
Standard surgical mask for patient Door closed all time Postponed elective procedure Signage and communication Airborne precautions include Standard precaution and…. You have to isolate patient in an airborne isolation room (AIIR). Signage outside room “ Airborne precaution” to indicate level of precautions. Use N95 respirator or greater when in the patient‘s room. Patient should remain in AIIR with door closed at all times, except for medically necessary procedures. Elective procedures should be postponed until patient no longer requires respiratory isolation. Patients should wear a standard surgical mask when transported outside the AIIR. The purpose of the mask is to prevent respiratory droplets from being expelled into the environment where they can become droplet nuclei. Operating rooms (ORs) are designed to be positive pressure in relation to the environment. Therefore, it is important to choose the most appropriate OR to minimize the risk of contamination. Options include the OR that is most remote from others, one with an antechamber, or one in which a portable negative pressure isolation chamber can be installed at the door. The surgical procedure should be scheduled at a time when it will minimize exposure of other patients and medical staff to the airborne infectious disease. Post-anesthesia recovery must take place with the same level of respiratory precautions. Communicate precaution level to receiving personnel. Room should remain vacant after the patient leaves until adequate time has elapsed to result in a 99.9% air turnover (duration dependent on number of air exchanges per hour in room).2 หารูปห้อง airborn isolation room
. Signage outside room Airborne precaution to indicate level of precautions. Use N95 respirator or greater when in the patient‘s room. Patient should remain in AIIR with door closed at all times, except for medically necessary procedures. Elective procedures should be postponed until patient no longer requires respiratory isolation. Patients should wear a standard surgical mask when transported outside the AIIR. The purpose of the mask is to prevent respiratory droplets from being expelled into the environment where they can become droplet nuclei. Operating rooms (ORs) are designed to be positive pressure in relation to the environment. Therefore, it is important to choose the most appropriate OR to minimize the risk of contamination. Options include the OR that is most remote from others, one with an antechamber, or one in which a portable negative pressure isolation chamber can be installed at the door. The surgical procedure should be scheduled at a time when it will minimize exposure of other patients and medical staff to the airborne infectious disease. Post-anesthesia recovery must take place with the same level of respiratory precautions. Communicate precaution level to receiving personnel. Room should remain vacant after the patient leaves until adequate time has elapsed to result in a 99.9% air turnover (duration dependent on number of air exchanges per hour in room).2. หารูปห้อง airborn isolation room.")
52
Airborne infection isolation room (AIIR)
Negative pressure Door close all-time 6-12 air exchanges per hour (ACH). Air exhausted directly to the outside or recirculated through a HEPA filter. AIIR is the Room that has negative pressure in relation to adjoining spaces. Door must be kept shut to maintain negative pressure. 6-12 air exchanges per hour (ACH). 6 ACH for existing structures, 12 ACH for new construction. Air exhausted directly to the outside (away from trafficked areas) or recirculated through a HEPA filter.
. Air exhausted directly to the outside or recirculated through a HEPA filter. AIIR is the Room that has negative pressure in relation to adjoining spaces. Door must be kept shut to maintain negative pressure air exchanges per hour (ACH). 6 ACH for existing structures, 12 ACH for new construction. Air exhausted directly to the outside (away from trafficked areas) or recirculated through a HEPA filter.")
53
Isotation Room AIIR ห้องแยกเดี่ยวควบคุมความดัน
ห้องมีความดันเป็นลบ แบบ Airborne Infectious Isolation Room (AIIR) เป็นห้อง ที่สร้างเพื่อ ควบคุม ไม่ให้เชื้อโรคในอากาศแพร่กระจายออกไปสู่สิ่งแวดล้อมในโรงพยาบาล หรือ สถานที่เสี่ยงภัยต่อการติดเชื้อในอากาศ เป็น ผลิตภัณฑ์ที่ได้มาตรฐานสากล สามารถนำเตียงผู้ป่วย และ อุปกรณ์ต่างๆ ที่ในการรักษาแบบวิกฤต ที่จำเป็นเข้าอยู่ไปในห้องแยกเดี่ยว โดยผ่านเข้า-ออก ทางประตู หน้าห้อง มีห้องanteroom มีประตูระบบ Airlock พร้อมอุปกรณ์สำหรับทิ้งชุดและวัตถุติดเชื้อ ภายในห้องมีความดันลบ negative air pressure ต่ำกว่าภายนอก -20 Pascal มีอากาศไหลเวียนภายในห้อง 12 เท่าของปริมาตร ห้องต่อชั่วโมง ( 12ACH ) ทิศทางการไหลของอากาศจากประตู Airlockไปสู่ผู้ป่วย (หรือ อากาศสะอาดมากไปสู่อากาศที่ติดเชื้อสกปรก) เพิ่มอุปกรณ์ สัญญาณแสง-เสียงเตือนภัย เมื่อความดันผิดปกติ มีการติดตั้งตัวกรอง HEPA filter (High Efficiency Particulate Air Filter)สำหรับกรอง อากาศที่หมุนเวียนในห้องและฆ่าเชื้อด้วยแสง UV ก่อนที่จะปล่อยอากาศสะอาดสู่ภายนอก ผนัง พลาสติกใส เหนียว ทนป้องกันการฉีกขาด สามารถต่อกับอุปกรณ์เสริม ให้แพทย์สามารถปฏิบัติการกับผู้ป่วยในห้อง ได้จาก ด้านนอกห้อง เช่น ถุงมือ เพิ่มอุปกรณ์ สัญญาณแสง-เสียงเตือนภัย เมื่อความดันผิดปกติ
 เป็นห้อง ที่สร้างเพื่อ ควบคุม ไม่ให้เชื้อโรคในอากาศแพร่กระจายออกไปสู่สิ่งแวดล้อมในโรงพยาบาล หรือ สถานที่เสี่ยงภัยต่อการติดเชื้อในอากาศ เป็น ผลิตภัณฑ์ที่ได้มาตรฐานสากล. สามารถนำเตียงผู้ป่วย และ อุปกรณ์ต่างๆ ที่ในการรักษาแบบวิกฤต ที่จำเป็นเข้าอยู่ไปในห้องแยกเดี่ยว โดยผ่านเข้า-ออก ทางประตู หน้าห้อง มีห้องanteroom มีประตูระบบ Airlock พร้อมอุปกรณ์สำหรับทิ้งชุดและวัตถุติดเชื้อ ภายในห้องมีความดันลบ negative air pressure ต่ำกว่าภายนอก -20 Pascal มีอากาศไหลเวียนภายในห้อง 12 เท่าของปริมาตร ห้องต่อชั่วโมง ( 12ACH ) ทิศทางการไหลของอากาศจากประตู Airlockไปสู่ผู้ป่วย (หรือ อากาศสะอาดมากไปสู่อากาศที่ติดเชื้อสกปรก) เพิ่มอุปกรณ์ สัญญาณแสง-เสียงเตือนภัย เมื่อความดันผิดปกติ มีการติดตั้งตัวกรอง HEPA filter (High Efficiency Particulate Air Filter)สำหรับกรอง อากาศที่หมุนเวียนในห้องและฆ่าเชื้อด้วยแสง UV ก่อนที่จะปล่อยอากาศสะอาดสู่ภายนอก. ผนัง พลาสติกใส เหนียว ทนป้องกันการฉีกขาด สามารถต่อกับอุปกรณ์เสริม ให้แพทย์สามารถปฏิบัติการกับผู้ป่วยในห้อง ได้จาก ด้านนอกห้อง เช่น ถุงมือ. เพิ่มอุปกรณ์ สัญญาณแสง-เสียงเตือนภัย เมื่อความดันผิดปกติ")
54
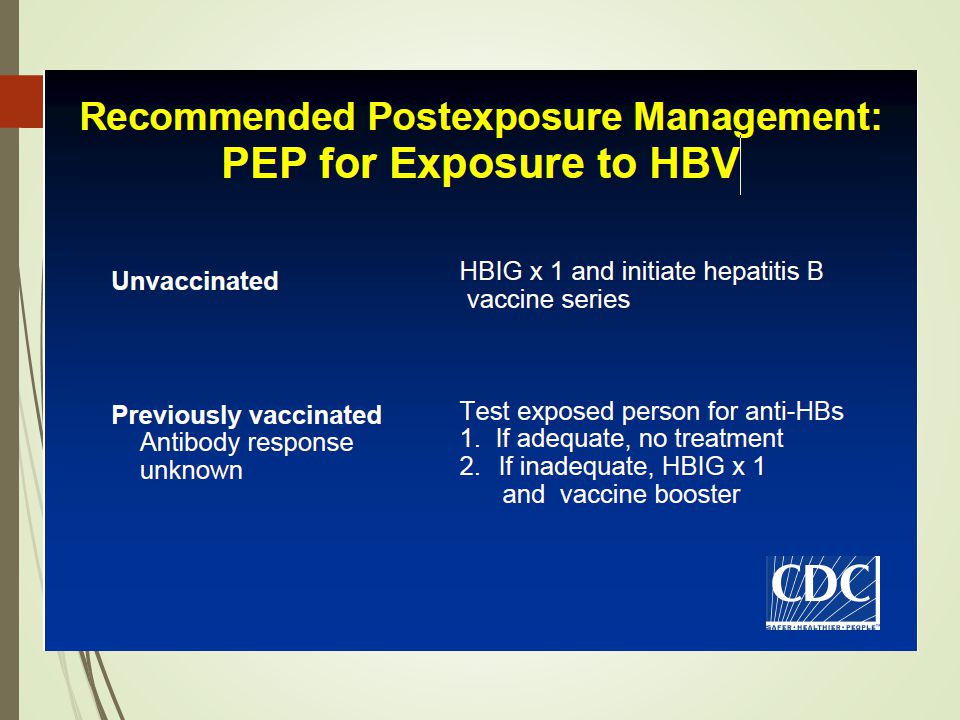
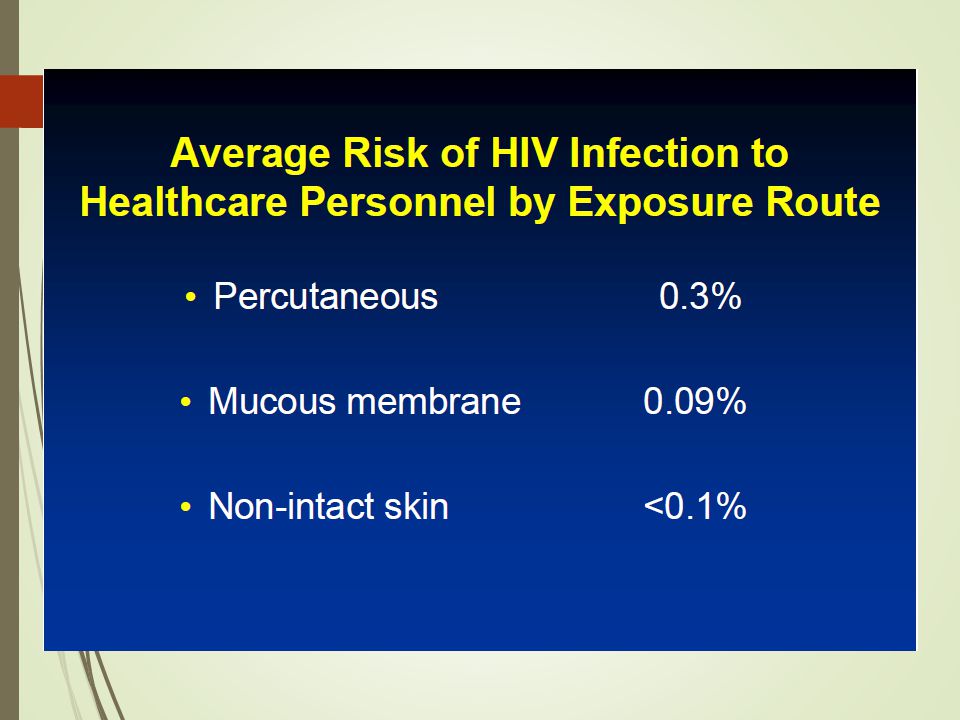
Blood borne Pathogens (HBV, HCV, HIV)
Recommendation All anesthesiologists should be vaccinated and have documented immunity to hepatitis B virus (HBV). Standard precautions Sharps safety Post-exposure prophylaxis guideline Next is about specific pathogen and immunization HIV,HBV and HCV are blood borne pathogens and can cause chronic infection CDC recommend that all anesthesiologists should be vaccinated and have documented immunity to hepatitis B virus (HBV). You should do standard precautions, sharps safety and receive post-exposure prophylaxis after a significant exposure
. Standard precautions. Sharps safety. Post-exposure prophylaxis guideline. Next is about specific pathogen and immunization. HIV,HBV and HCV are blood borne pathogens and can cause chronic infection. CDC recommend that all anesthesiologists should be vaccinated and have documented immunity to hepatitis B virus (HBV). You should do standard precautions, sharps safety and receive post-exposure prophylaxis after a significant exposure.")
57
Tuberculosis Postponed until the patient is no longer infectious.
Elective Surgery for Patients with Active TB Infection Recommendation Postponed until the patient is no longer infectious. We should postpone surgery for the active TB infected patient in case of elective surgery.

58
Tuberculosis Airborne Precautions
Urgent/Emergent Surgery for Patients with Active TB Infection Recommendation Airborne Precautions For urgent and emergent procedures that must be performed on patients with diagnosed or suspected TB, measures must be taken to minimize the exposure of other patients and health care workers (HCWs) who are in the operating room suites. For Transmission-Based Precautions, we use Airborne Precautions.
 who are in the operating room suites. For Transmission-Based Precautions, we use Airborne Precautions.")
59
Tuberculosis N95 (or higher protection factor)
Filters with an efficiency rating of >95% for particle sizes of 0.3 μm on the Anesthesia Breathing Circuit Recover in a respiratory isolation room or in the OR These are measures we use.

60
Tuberculosis TB Screening Programs for HCWs Recommendation
Baseline screening and yearly testing a tuberculin skin test (TST) a QuantiFERON®-TB Gold (QFT-G) blood test. Positive TST-> chest radiography and review of symptoms Exposed to TB screened shortly after the exposure and again in 12 weeks There is recommendation for medical personnel to have TB screening by using tuberculin skin test. If it ‘s positive, there is the role of CXR and reviewing the symptom. Personnel who have been exposed to TB should be screened shortly after the exposure and again in 12 weeks to test for conversion. (baseline screening and yearly testing for exposure to MTB. Baseline screening a tuberculin skin test (TST) or a QuantiFERON®-TB Gold (QFT-G) blood test. Individuals with a positive TST require chest radiography, and a review of symptoms is used for future screening. The QFT-G test exposes whole blood to MTB antigens and measures the interferon-gamma released from the white blood cells. Personnel who have been exposed to TB should be screened shortly after the exposure and again in 12 weeks to test for conversion)
 a QuantiFERON®-TB Gold (QFT-G) blood test. Positive TST-> chest radiography and review of symptoms. Exposed to TB screened shortly after the exposure and again in 12 weeks. There is recommendation for medical personnel to have TB screening by using tuberculin skin test. If it ‘s positive, there is the role of CXR and reviewing the symptom. Personnel who have been exposed to TB should be screened shortly after the exposure and again in 12 weeks to test for conversion. (baseline screening and yearly testing for exposure to MTB. Baseline screening. a tuberculin skin test (TST) or a QuantiFERON®-TB Gold (QFT-G) blood test. Individuals with a positive TST require chest radiography, and a review of symptoms is used for future screening. The QFT-G test exposes whole blood to MTB antigens and measures the interferon-gamma released from the white blood cells. Personnel who have been exposed to TB should be screened shortly after the exposure and again in 12 weeks to test for conversion)")
61
Emerging Infectious Diseases/Pandemic Influenza
Droplet precaution VS airborne precaution VS contact precaution Vaccination against H1N1 and seasonal influenza in all healthcare workers

62
Operating room Set OR for emergency and urgency case
Limiting the personnel involved in the case Choosing an operating suite remote from others Remove all unnecessary equipment Full PPE Recovery of the patient should be in isolation. PPE should be disposed of upon leaving the OR The anesthesia circuit and gas sampling line should be disposed of at the conclusion of the case. All surfaces should be disinfected with an agent approved by the Environmental Protection Agency (EPA).14,17 Patients should be brought to the OR for urgent or emergent cases only. Efforts should be made to limit exposure of personnel and patients. This may include performing the surgery when the fewest people are present, limiting the personnel involved in the case, and choosing an operating suite remote from others. All unnecessary equipment should be removed from the room to avoid possible contamination. Full PPE should be used. Bacterial/viral filters should be used on the anesthesia circuit to prevent exposure of the machine to respiratory pathogens. Recovery of the patient should be in isolation. PPE should be disposed of upon leaving the OR and clean PPE donned for transport. The anesthesia circuit and gas sampling line should be disposed of at the conclusion of the case. All surfaces should be disinfected with an agent approved by the Environmental Protection Agency (EPA).14,17
.14,17. Patients should be brought to the OR for urgent or emergent cases only. Efforts should be made to limit exposure of personnel and patients. This may include performing the surgery when the fewest people are present, limiting the personnel involved in the case, and choosing an operating suite remote from others. All unnecessary equipment should be removed from the room to avoid possible contamination. Full PPE should be used. Bacterial/viral filters should be used on the anesthesia circuit to prevent exposure of the machine to respiratory pathogens. Recovery of the patient should be in isolation. PPE should be disposed of upon leaving the OR and clean PPE donned for transport. The anesthesia circuit and gas sampling line should be disposed of at the conclusion of the case. All surfaces should be disinfected with an agent approved by the Environmental Protection Agency (EPA).14,17.")
63
Respirators for the Care of Patients With Virulent Respiratory Pathogens SARS
หารูป จากoutbreak…. หนังจากหนัง NIOSH-approved N-95 respirator powered air-purifying respirators (PAPRs) PAPRs use HEPA filters (high-efficiency particulate air filters), which are as efficient as P-100 filters and will protect against SARS
 PAPRs use HEPA filters (high-efficiency particulate air filters), which are as efficient as P-100 filters and will protect against SARS.")
64
Most N95 respirators are manufactured for use in construction and other industrial type jobs that expose workers to dust and small particles. These respirators are evaluated for effectiveness by the National Institute for Occupational Safety and Health (NIOSH), which is part of the Centers for Disease Control (CDC). These are labeled "For occupational use.”
, which is part of the Centers for Disease Control (CDC). These are labeled For occupational use. .")
65
Immunization of Health-Care Workers Recommendations of the Advisory Committee on Immunization Practices (ACIP) and the Hospital Infection Control Practices Advisory Committee (HICPAC)
 and the Hospital Infection Control Practices Advisory Committee (HICPAC)")
66
Strongly recommendations for HCW
BCG Hepatitis B Influenza MMR Varicella-zoster

67
Hepatitis B No serologic evidence of immunity or prior vaccination
If you’re no evidence of serologic immunity or prior vaccination. You should got 3 dose series at 0, 1 and 6 month. And follow up anti-HBs serologic at 1-2 month after dose3.

68
Influenza Get 1 dose of influenza vaccine annually
You should got 1 dose vaccine annually.

69
MMR (measles, mumps, rubella)
No serologic evidence of immunity or previous vaccination Get 2 dose of MMR , 4week apart If no evidence of serologic immunity or prior vaccination. You should got 2 dose of MMR and 4 week apart.

70
Varicella-zoster (chicken pox)
No serologic evidence of immunity or previous vaccination Get 2 dosed of varicella vaccine , 4 weeks apart

71
Tetanus, Diphtheria, Pertussis
มักจะได้รับแล้ว

72
Infectious control is in your hands.

งานนำเสนอที่คล้ายกัน
 ในช่วงยุค Internet เพิ่ง เริ่มต้น เป็นบริษัทที่ดำเนินงานทางด้าน.>")






 /ˈfɪlθi/ –extremely dirty. –( สกปรกมาก )>")











