ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
10 กรกฏาคม 2551 CPC

2
History ผู้ป่วยชายไทย คู่ อายุ 26 ปี อาชีพ วิศวกรเครื่องกล
ภูมิลำเนา & ที่อยู่ปัจจุบัน จ.กรุงเทพฯ ประวัติได้จากผู้ป่วย และเวชระเบียน เชื่อถือได้ 7th admission 24/4/51

3
History CC : ไข้ 10 วัน ก่อนมารพ.
PI : Preexisting precursor B cell ALL ขณะนี้ อยู่ใน phase V in remission period แข็งแรงดี ทำกิจวัตรประจำวันได้ปกติ 10 วัน PTA: ไปเที่ยวดำน้ำ จ.ชุมพร ถูกกัด โดยแตนทะเล หลังดำน้ำขึ้นมาบนเรือสังเกตเห็น ผื่นแดงที่แขน และต้นขา 2 ข้างบริเวณนอกร่มผ้า รู้สึกคัน ไม่มีอาการอื่น เพื่อนที่ไปด้วยกัน มีผื่น แบบเดียวกัน

4
History 8 วัน PTA: ผื่นเริ่มกลายเป็นจุดแดงเป็นปื้นๆ ขึ้นทั่ว ตัว เป็นมากที่แขนขา (เพื่อนๆ ผื่นเริ่มหาย) รู้สึกมี ไข้ต่ำๆ ไม่หนาวสั่น เป็นไข้ตลอดเวลา ปวดเมื่อย ตามตัว คลื่นไส้ ไม่อาเจียน ไม่มีไอ ไม่เจ็บคอ ไม่มี น้ำมูก ปัสสาวะไม่แสบขัด ไม่มีถ่ายเหลว ไปตรวจที่ ร.พ.เอกชน นอนร.พ.3 วันได้ยา moxifloxacin IV 2 วันไข้ลง ผื่นยุบหายคัน กลับบ้านได้ยา moxifloxacin กินต่อ
 รู้สึกมี ไข้ต่ำๆ ไม่หนาวสั่น เป็นไข้ตลอดเวลา ปวดเมื่อย ตามตัว คลื่นไส้ ไม่อาเจียน ไม่มีไอ ไม่เจ็บคอ ไม่มี น้ำมูก ปัสสาวะไม่แสบขัด ไม่มีถ่ายเหลว ไปตรวจที่ ร.พ.เอกชน นอนร.พ.3 วันได้ยา moxifloxacin IV 2 วันไข้ลง ผื่นยุบหายคัน กลับบ้านได้ยา moxifloxacin กินต่อ.")
5
History 3 วัน PTA: หลังกลับจาก ร.พ 2 วันมีไข้ขึ้น ปวด เมื่อยตามตัวอยู่ ไปตรวจและนอน ร.พ.เอกชน - CBC: WBC 1,500 ( N 76%,L 15%,M 9%, E0 1%), Hb 13, Hct 39%, MCV 110, Plt 150,000, UA normal, Urine culture: NG, Hemoculture: NG, CXR: normal - ได้ยา ceftazidime+amikacin IV, add Neutromax 300 mcg SC OD นอนโรงพยาบาล 2 วันอาการไม่ดีขึ้น ผู้ป่วยขอมารักษา ร.พ.จุฬาเพราะ มีประวัติรักษาอยู่เดิม ระหว่างไม่สบายครั้งนี้ไม่มี น้ำหนักลด
, Hb 13, Hct 39%, MCV 110, Plt 150,000, UA normal, Urine culture: NG, Hemoculture: NG, CXR: normal. - ได้ยา ceftazidime+amikacin IV, add Neutromax 300 mcg SC OD นอนโรงพยาบาล 2 วันอาการไม่ดีขึ้น ผู้ป่วยขอมารักษา ร.พ.จุฬาเพราะ มีประวัติรักษาอยู่เดิม ระหว่างไม่สบายครั้งนี้ไม่มี น้ำหนักลด.")
6
Past history Precursor B acute lymphoblastic leukemia Dx พ.ค รพ.จุฬาฯ มาด้วยไข้ต่ำๆ อ่อนเพลีย เลือดออกตามไรฟัน ตรวจ รพ.นครธน -> CBC : Hb 7, Hct 20.4%, WBC 45,200 (blast 90%) refer มารพ.จุฬา BMA : lymphoblast 95% (ALL, L2) Flow cytometry: CD19+, CD20+, CD10+, CD34+, HLA-DR+, TdT+ Chromosome study : 46, XY
 refer มารพ.จุฬา. BMA : lymphoblast 95% (ALL, L2) Flow cytometry: CD19+, CD20+, CD10+, CD34+, HLA-DR+, TdT+ Chromosome study : 46, XY.")
7
ALL Treatment Protocol
24 mo PTA 22 mo PTA 20 mo PTA 17 mo PTA 16 mo PTA Phase I Phase II Phase III Phase IV (1) Phase IV (2) Vincristine Doxorubcin L-asp Prednisone 6-MP Cyclophos. Ara-C IT MTX XRT-CNS Doxorubicin Dexa 6-TG Febrile Neutropenia BM Bx : NL Flow : NL Febrile Neutropenia HLA-Match Donor BM Bx : CR Acyclovir, Fluconazole
 Phase IV (2) Vincristine. Doxorubcin. L-asp. Prednisone. 6-MP. Cyclophos. Ara-C. IT MTX. XRT-CNS. Doxorubicin. Dexa. 6-TG. Febrile Neutropenia. BM Bx : NL. Flow : NL. Febrile. Neutropenia. HLA-Match. Donor. BM Bx : CR. Acyclovir, Fluconazole.")
8
Past History 15 mo PTA : ALL protocol Phase V
6–MP (50 mg) 2*1 -> ½ * 1 OD (due to pancytopenia) Metrothexate (2.5 mg) 13*1 -> 6*1 OW Co-trimoxazole 2*1 twice a week Acyclovir (200) 1*3 thrice a week
 2*1 -> ½ * 1 OD (due to pancytopenia) Metrothexate (2.5 mg) 13*1 -> 6*1 OW. Co-trimoxazole 2*1 twice a week. Acyclovir (200) 1*3 thrice a week.")
9
Past History 1 เดือน PTA: มาตรวจตามนัด สบายดี น้ำหนักปกติ (BW 62 Kg) PE: no hepatosplenomegaly - CBC: WBC 3,240 (N 54%, L 25%, Mo 11%), Hb 13.8, Hct 40% MCV 113, RDW 17, Plt 203,000, no blast cell - BM study : complete remission - Flow cytometry: no detectable leukemia cell
, Hb 13.8, Hct 40% MCV 113, RDW 17, Plt 203,000, no blast cell. - BM study : complete remission. - Flow cytometry: no detectable leukemia cell.")
10
Physical examination A young Thai male, febrile, no tachypnea
V/S : BT 39.5°C, RR 18/min BP 110/60 mmHg, PR 96/min Skin : diffuse mild erythematous papules both exposed sites of arms and legs

11
Physical examination HEENT: No pale conjuctivae, no icteric sclerae, no oral candidiasis , mild enlarged non-inflamed tonsils, multiple bilateral posterior cervical, axilla and epitrochlear lymph nodes size cm in size

13
Physical examination Heart : PMI at Lt 5th ICS, MCL, regular, normal S1,S2, no murmur Lungs : clear Abdomen : no distension, active BS, soft, not tender, liver 1 cm below RCM, sharp edge, not tender, firm, span 12 cm, spleen 2 cm below left costal margin, not tender Extremities : no edema, no eschar

14
Investigation CBC: Hb 13.6, Hct 39.7%, MCV 106, RDW 14.6, WBC 3,430 (N 86.3%, L 11.4%, M 1.7%, Eo 0.3%, B 0.3%), Plt 53,000 PT 13.5, INR 1.2, PTT 32.6 BUN/Cr: 4/0.64 LFT: TB/DB 0.5/0.14, AST/ALT 37/69, ALP 85, globulin 2.4, albumin 4.0 UA: WBC 0, RBC 0, Protein: neg, Sugar: neg U/C: NG , H/C: NG x II Anti-HIV: negative

16
Treatment with Ceftazidime 2 g IV q 8 hr were given together with G-CSF 480 mcg SC OD.
Diagnostic tests were performed.

17
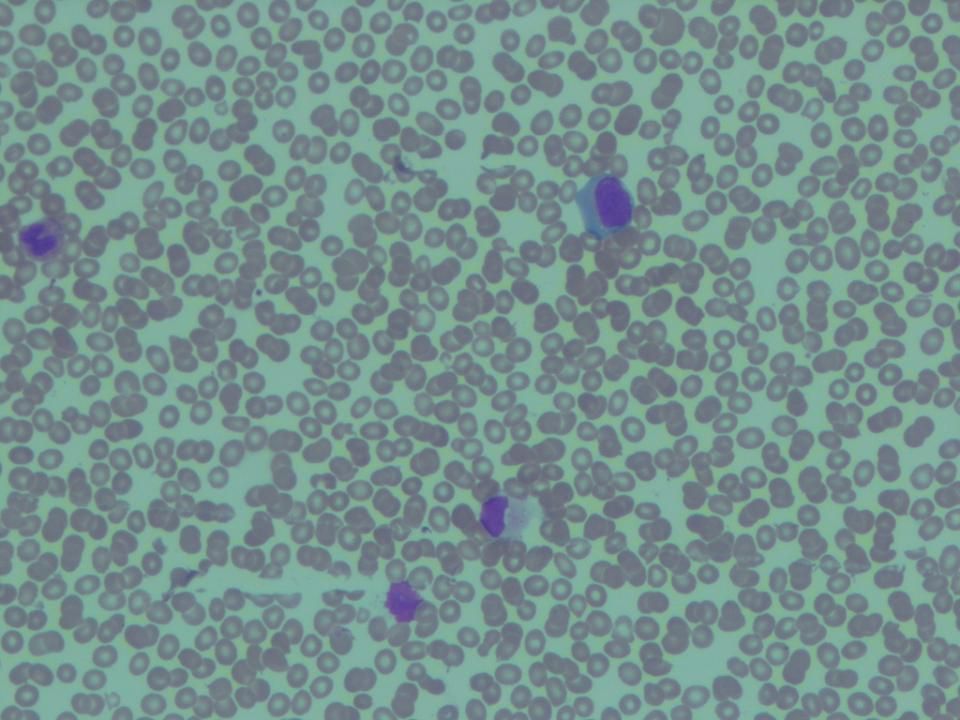
Cardinal Features A young man with protracted course of fever, malaise, erythematous rash, enlarged tonsils, generalized lymphadenopathy and hepatosplenomegaly Leukopenia and thrombocytopenia with atypical lymphocytosis Acute or subacute viral infection Mononucleosis-like syndrome?

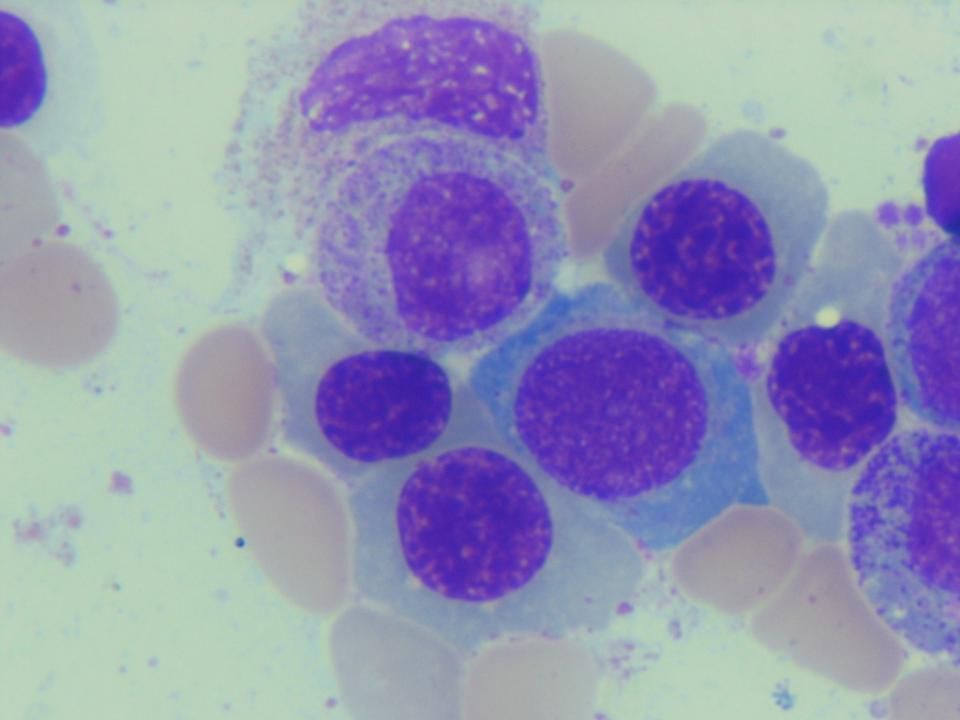
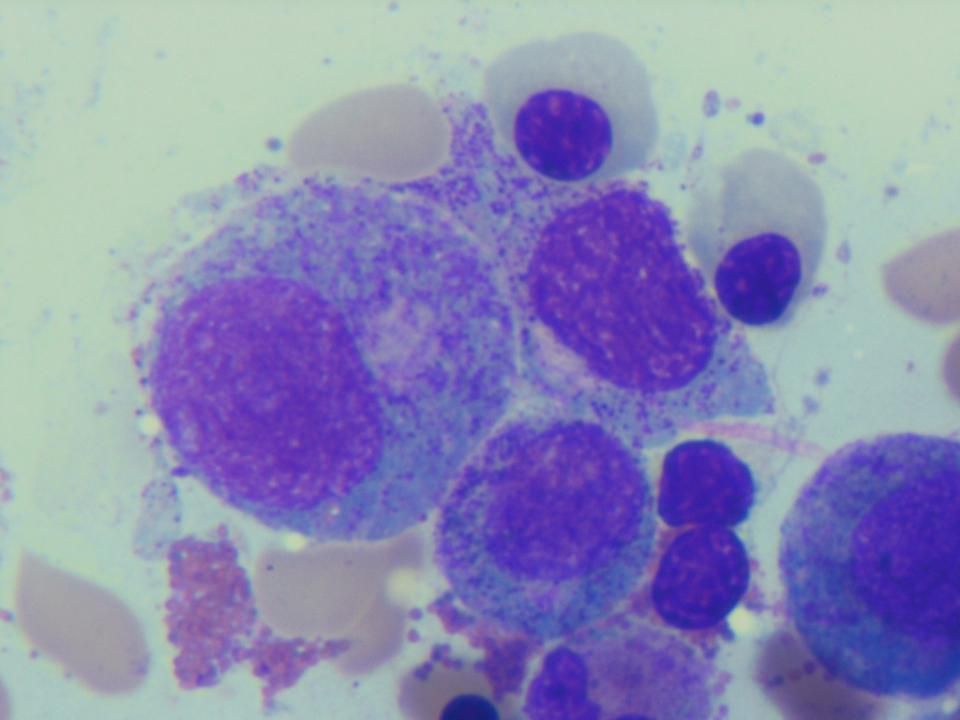
18
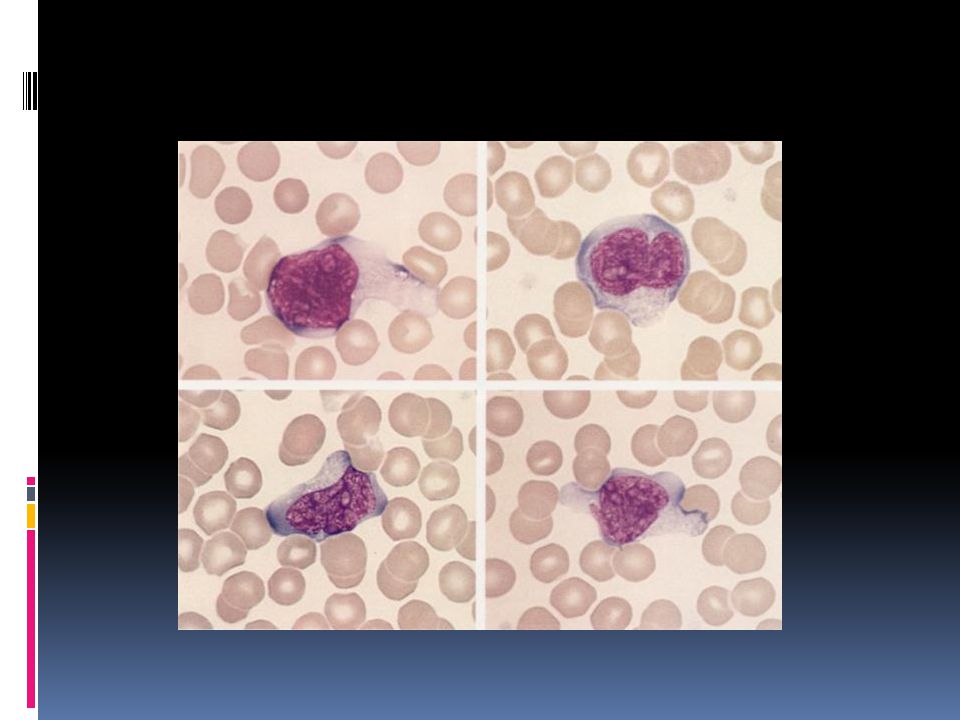
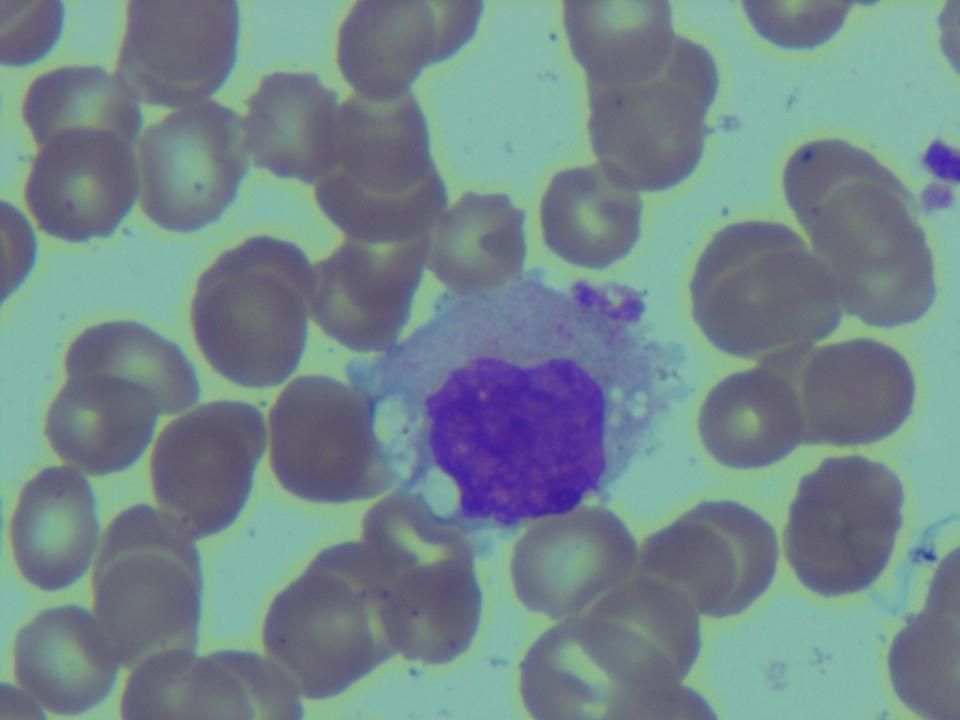
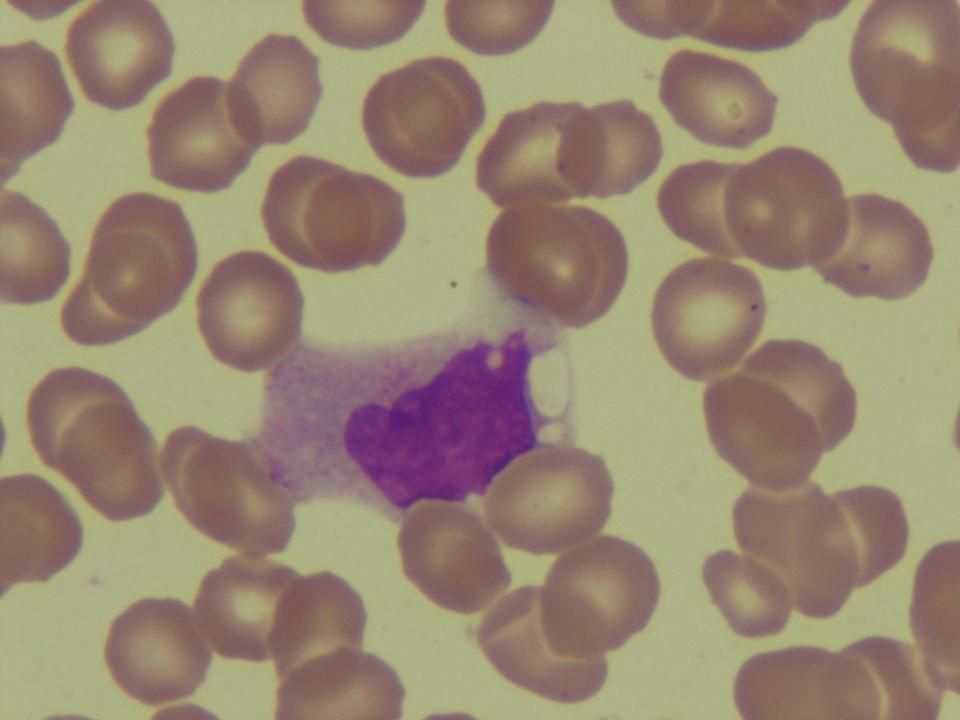
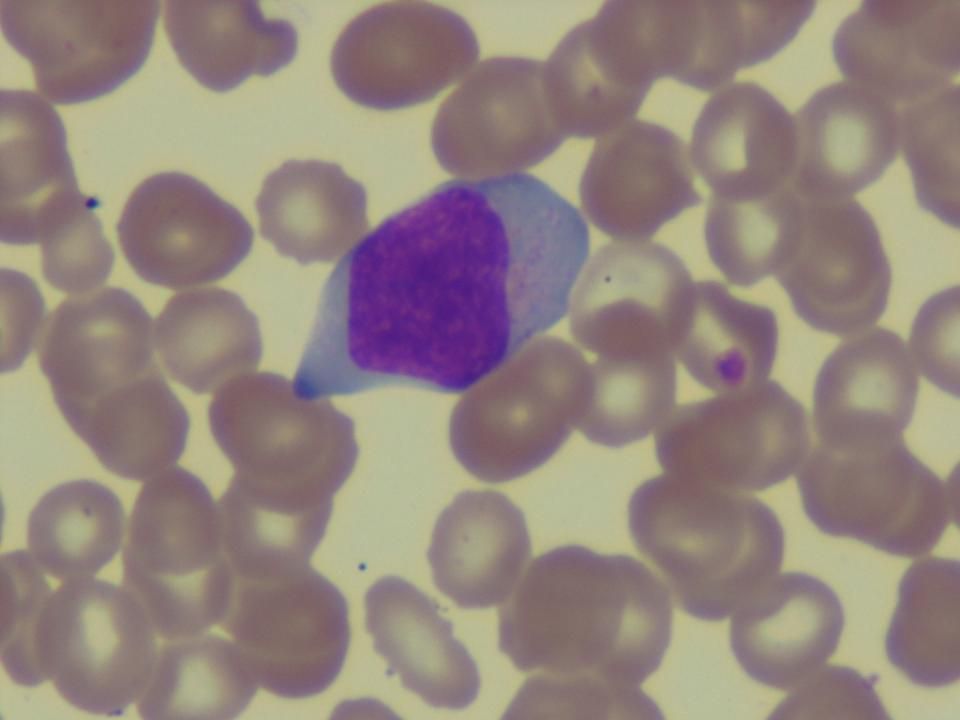
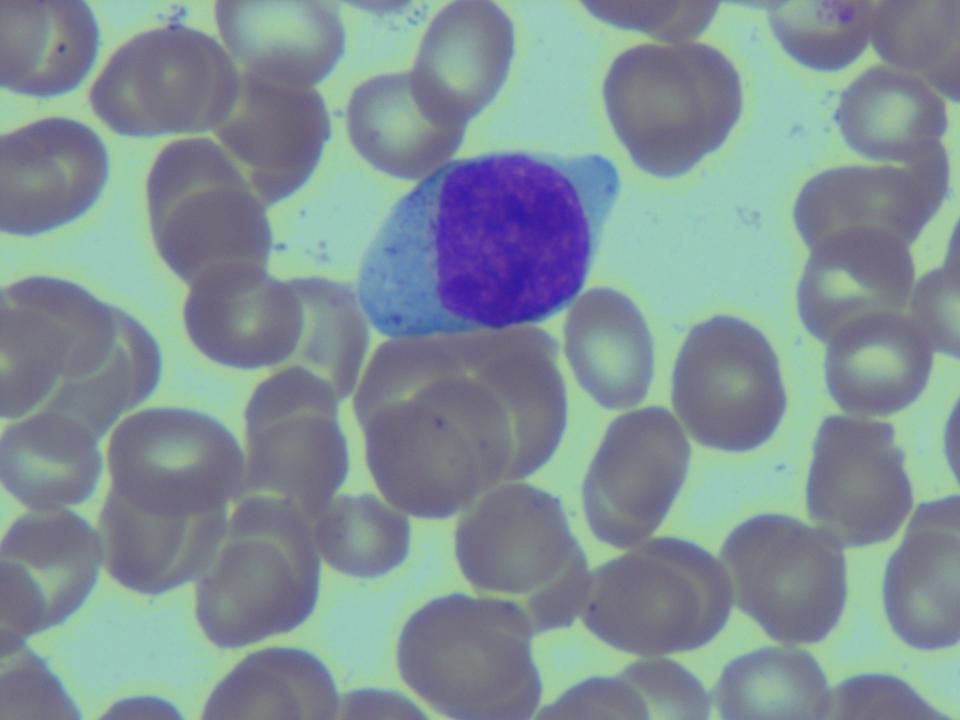
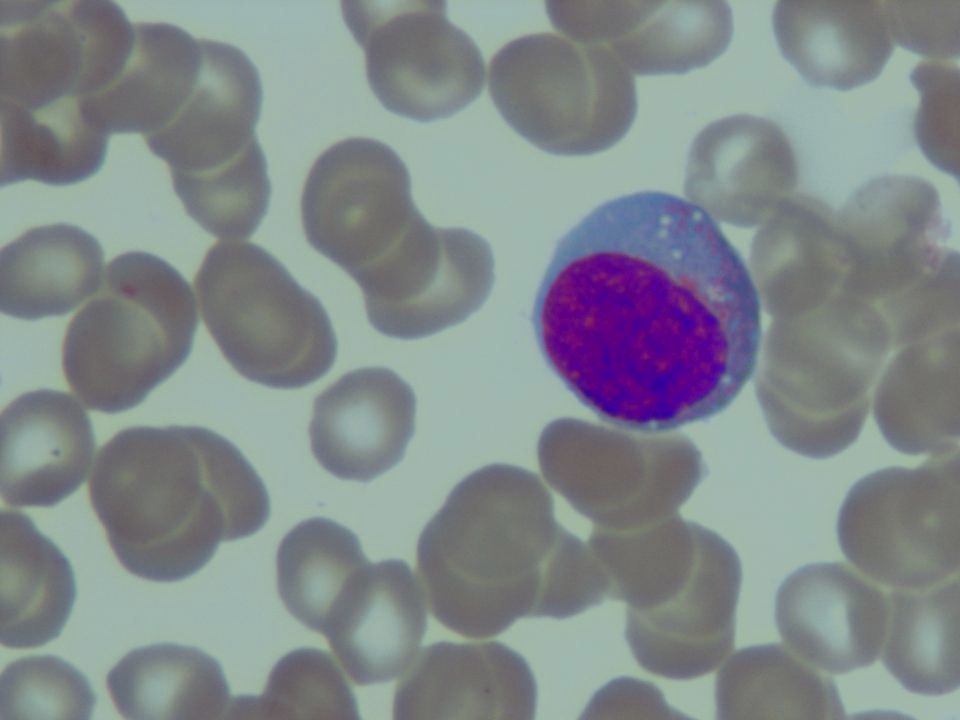
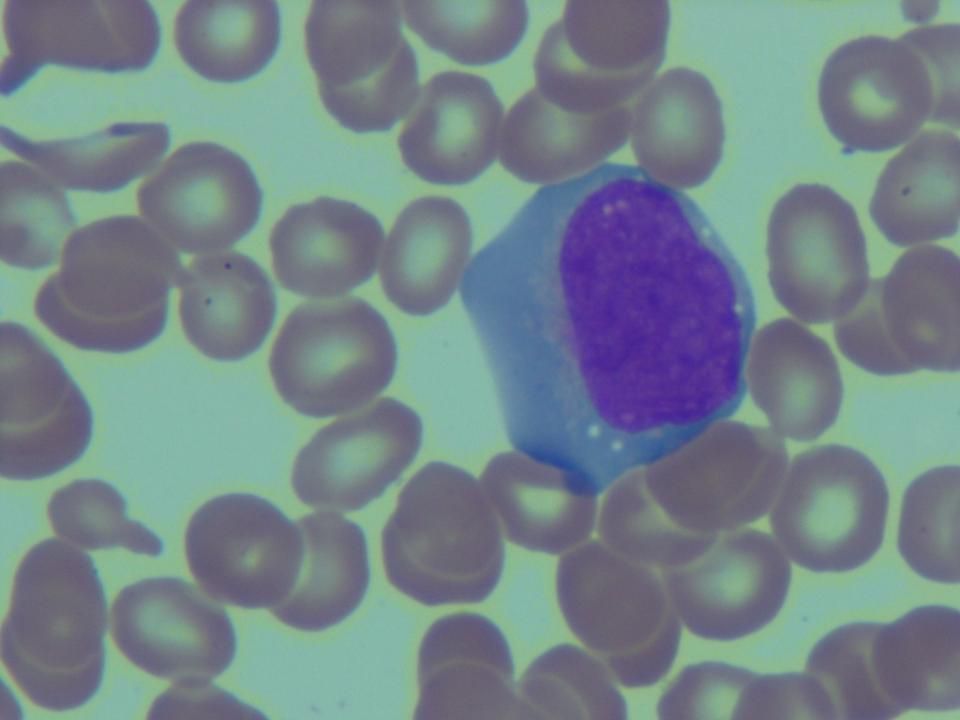
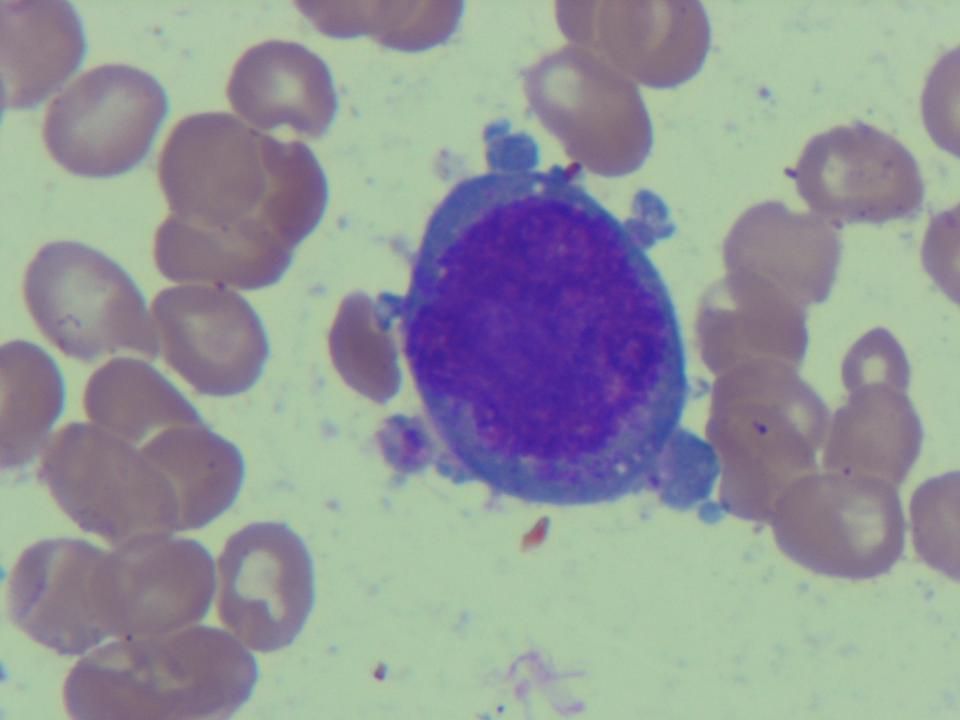
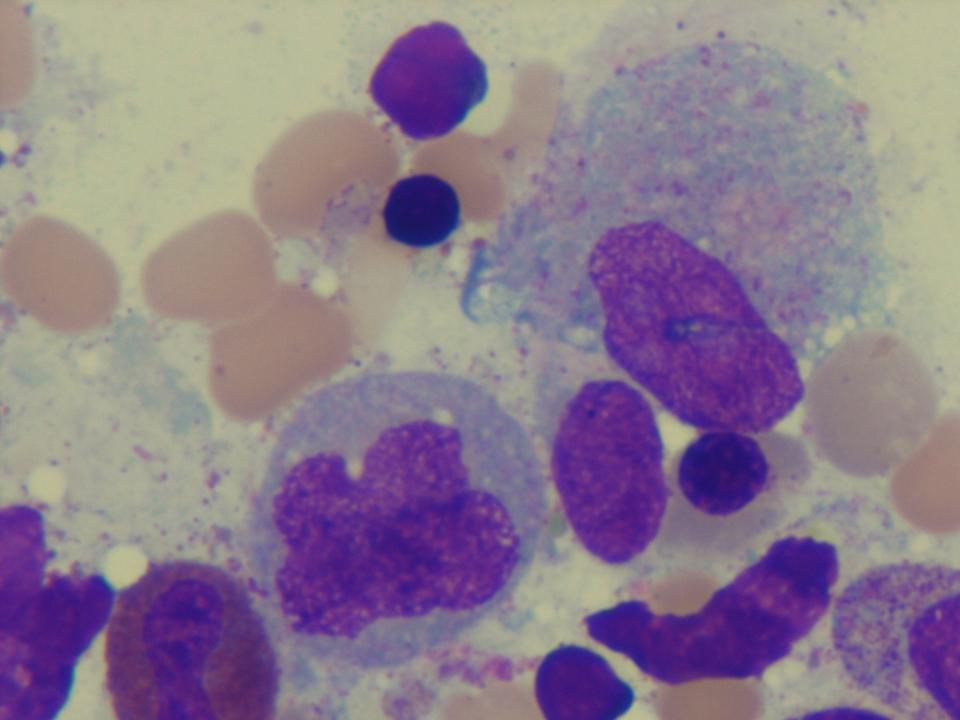
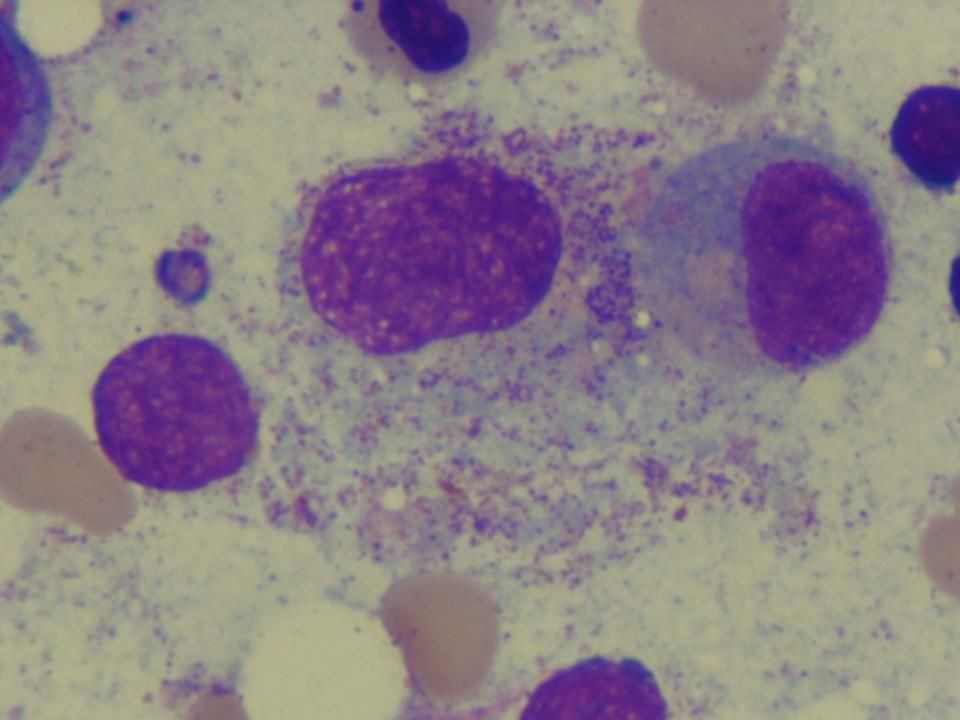
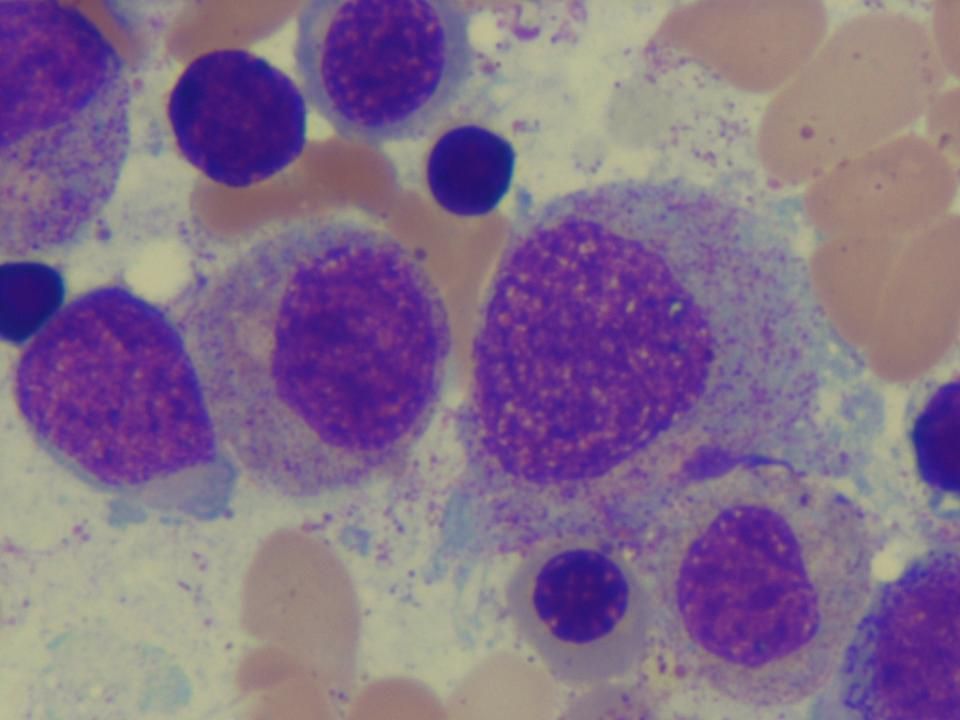
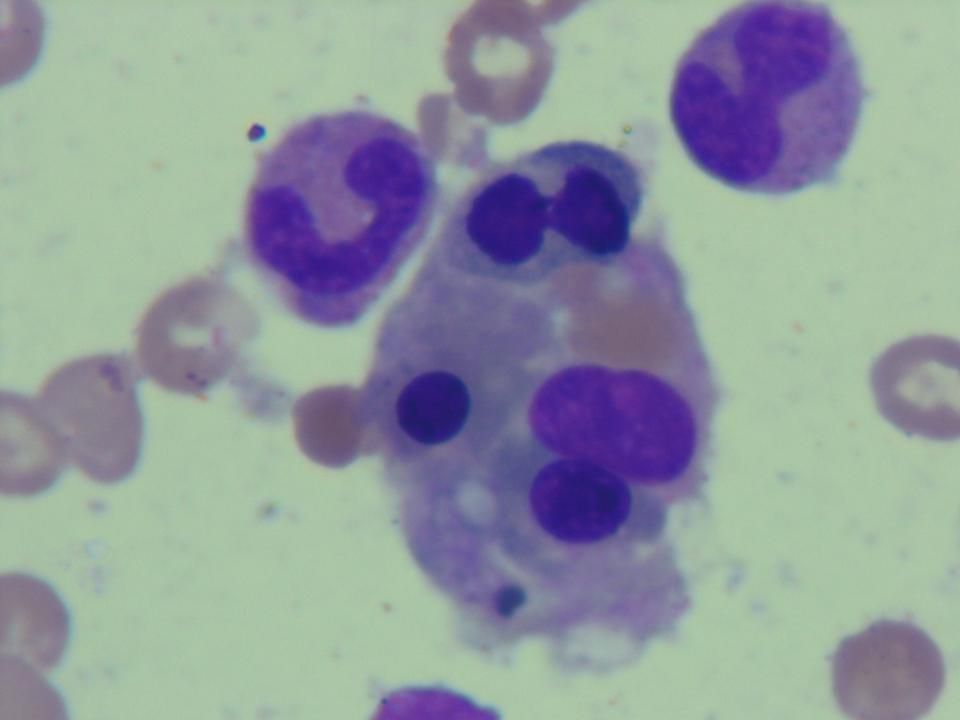
Atypical Lymphocytes First distinguished morphologically from leukemic lymphoblasts by Downey and McKinlay in 1923.

19
Atypical Lymphocytes At least 4 types are easily recognizable
Typical monocytoid atypical lymphocytes: activated CD8+ T cells Plasmacytoid atypical lymphocytes: activated B cells Large granular lymphocytes: cytotoxic T or NK cells Lymphoblastoid atypical lymphocytes: any activated cells about to enter cell division or viral-transformed B or T cells

29
8 days PTA Exposure to แตนทะเล then fever with rash ไข้ลดลง ผื่นยุบ
Fever with chills Admit นครธน Admit นครธน 8 days PTA 3 days PTA 5 days PTA KCMH Hb 13, WBC 1500, N 76%, L 15%, plt 150,000 H/C NG x I, U/C NG WBC 2500 N 73%, L 15% Hb 13.6, WBC 3430, N 86%, L 12%, plt 53,000 Ceftazidime+Amikacin+G-CSF Moxifloxacin 400 mg iv OD Moxifloxacin po

30
Classical Description of Infectious Mononucleosis
From Wintrobe’s Hematology 10th Edition, pp ; reproduced from Carter PL, Penman HG. Infectious Mononucleosis, 1969.

31
Differential Diagnoses of Mononucleosis-like Illnesses
Infection Viruses: EBV, CMV, HHV-6, HSV-1, HIV, Adenovirus, Enteroviruses, Hepatitis A, B, rubella Non-viral infection: Toxoplasma, Group A streptococcus, Bartonella, Turalemia, Brucellosis, Rickettsiosis, Malignant lymphoproliferative disease (CLL, NHL, HL) Connective tissue disease: SLE, Felty’s syndrome, sarcoidosis Drug hypersensitivity: phenytoin, carbamazepine, minocycline, allopurinol,
 Connective tissue disease: SLE, Felty’s syndrome, sarcoidosis. Drug hypersensitivity: phenytoin, carbamazepine, minocycline, allopurinol,")
32
Algorithmic approach to mononucleosis-like illnesses
Hurt C, Tammaro D. Diagnostic evaluation of mononucleosis-like illnesses. Am J Med 2007;120:911-

33
What’s wrong with the pattern recognition approach to complex medical problems?
Requires careful characterization or classical presentation of each symptom in “triads”, “tetrads” or “pentad” of diagnostic criteria Sensitivity and specificity increase with the numbers of typical features Beware mimicry of S&S by other causes or syndromes Modification of S&S by underlying, associated diseases or treatments Give no insight into the pathogenesis of diseases or syndromes

34
Additional Features History of exposure to แตนทะเล (sea wasp?)
History of exposure to moxifloxacin Pre-B ALL in remission on maintenance chemotherapy Sensitive to myelosuppressive effects of ethotrexate and 6-mercaptopurine

35
แตนทะเล = Sea Wasp or Box Jellyfish?
“Box jellyfish are best known for the extremely powerful venom possessed by some of their species. The Chironex fleckeri and the Carukia barnesi (Irukandji) species are the most venomous creatures in the world. Stings from such species are excruciatingly painful, either initially or as an after-effect, and are often fatal.” From Wikipedia accessed at
 species are the most venomous creatures in the world. Stings from such species are excruciatingly painful, either initially or as an after-effect, and are often fatal. From Wikipedia accessed at")
36
แตนทะเล คือ อะไร Sea Wasp?
แตนทะเล เป็นสัตว์ขนาดเล็กล่องลอยอยู่ในน้ำ ส่วนใหญ่มักจะพบในการลงดำน้ำในช่วงเช้ามากกว่าการลงดำในช่วงบ่าย จัดอยู่ในจำพวกแพงตอนขนาดเล็กมักจะอยู่รวมกันเป็นกลุ่มๆ มองดูคล้ายว่าในน้ำมีตะกอน สิ่งที่เราสังเกตได้คือว่าน้ำจะขุ่นกว่าปกติเหมือนมีเศษตะกอนลอยอยู่ในน้ำ ซึ่งเราก็จะแยกไม่ออกว่านั่นคือตะกอนหรือแตนทะเล เราจะรู้ก็ต่อเมื่อโดนมันต่อย อาการเมื่อโดนแตนทะเลต่อยจะรู้สึกเจ็บจี๊ดๆ เหมือนโดนเข็มขนาดเล็กจิ๊ม แต่เจ็บไม่เท่าไรพอทนได้ การรักษา ส่วนใหญ่ไม่แพ้ เมื่อโดนต่อยก็จะรู้สึกเจ็บเฉยๆ แต่สำหรับคนที่แพ้จะมีอาการเป็นจุดแดงและบวมเล็กน้อย แก้ไขด้วยการทานยาแก้แพ้ แต่สำหรับผู้ที่มีอาการแพ้มากจะต้องไปพบแพทย์ฉีดยาสักเข็มก็หาย ที่สำคัญเมื่อโดนแตนต่อยแล้วเกิดตุ่มแดงและคันห้ามเกา ปล่อยไว้อย่างนั้นถึงแม้จะคันก็ทนเอาหน่อย เมื่อทานยาหรือฉีดยาแล้วแผลยุบหายไปก็จะไม่มีแผลเป็น ไม่เสียโฉม

37
ภาพจากเวปไซต์ pantip.com

38
ภาพจากเวปไซต์ pantip.com

39
EBV-associated lymphoproliferative disease and mosquito bite allergy
Hypersensitivity to mosquito bite (HSMB) has been recognized as a spectrum of EBV-associated diseases, especially in the Far East (Japan and Korea) Patients are predisposed to develop hemophagocytic syndrome and clonal EBV- associated lymphoproliferative disease (usually NK or T/NK lymphoma) J Dermatol Sci. 2007;45(3):
 has been recognized as a spectrum of EBV-associated diseases, especially in the Far East (Japan and Korea) Patients are predisposed to develop hemophagocytic syndrome and clonal EBV- associated lymphoproliferative disease (usually NK or T/NK lymphoma) J Dermatol Sci. 2007;45(3):")
40
Pathogenesis of HSMB Poorly understood and studies
Usually increased EBER+ CD16+/CD56+ NK cells in peripheral blood Augmented CD4+ T cells response to EBV J Dermatol Sci. 2007;45(3):
:")
41
Additional Features History of exposure to แตนทะเล (sea wasp?)
History of exposure to moxifloxacin Pre-B ALL in remission on maintenance chemotherapy Sensitive to myelosuppressive effects of ethotrexate and 6-mercaptopurine

42
8 days PTA Exposure to แตนทะเล then fever with rash ไข้ลดลง ผื่นยุบ
Fever with chills Admit นครธน Admit นครธน 8 days PTA 3 days PTA 5 days PTA KCMH Hb 13, WBC 1500, N 76%, L 15%, plt 150,000 H/C NG x I, U/C NG WBC 2500 N 73%, L 15% Hb 13.6, WBC 3430, N 86%, L 12%, plt 53,000 Ceftazidime+Amikacin+G-CSF Moxifloxacin 400 mg iv OD Moxifloxacin po

43
Is there any relationship to moxifloxacin exposure?
No case of mononucleosis-like illness has been reported in patients receiving moxifloxacin in the literature Antibiotics-induced erythematous rashes in infectious mononucleosis are well- known for beta-lactam (especially amoxicilllin) but were also reported in macrolides, doxycycline and quinolones
 but were also reported in macrolides, doxycycline and quinolones.")
44
Picture from Sandoz Atlas of Clinical Haematology 1994.
Morbilliform erythematous eruption in infectious mononucleosis after exposure to amoxicillin. Picture from Sandoz Atlas of Clinical Haematology 1994.

45
Additional Features History of exposure to แตนทะเล (sea wasp?) and moxifloxacin Pre-B ALL in remission on maintenance chemotherapy Is it relapsed? Sensitive to myelosuppressive effects of ethotrexate and 6-mercaptopurine

46
ALL-L2 by FAB classification

47
Immunological classification of ALL

48
Estimated Frequencies of Specific Genotypes in ALL
Figure 2. Estimated Frequencies of Specific Genotypes among Children and Adults with ALL. The data are from studies at St. Jude Children's Research Hospital4,8 and from the Groupe Francais de Cytogenetique Hematologique,5 Chessells et al.,6 and Copelan and McGuire.7 Pui, C.-H. et al. N Engl J Med 1998;339:

49
Poor prognostic factors in ALL
B-lineage ALL Age > 50 years WBC > 30,000/L Pro-B ALL (CD10-) t(9;22)[BCR/ABL] t(4;11)[AF4/MLL] CR > 4 weeks T-lineage ALL WBC > 100,000/L Early-T or mature-T CR > 4 weeks German Multicenter ALL Group 2000
 t(9;22)[BCR/ABL] t(4;11)[AF4/MLL] CR > 4 weeks. T-lineage ALL. WBC > 100,000/L. Early-T or mature-T. CR > 4 weeks. German Multicenter ALL Group")
50
Outcomes of ALL treated by standard protocol
Thomas, X. et al. J Clin Oncol; 22:

51
TREATMENT OF ACUTE LYMPHOBLASTIC LEUKEMIA (ALL)
Induction chemotherapy Combination of VCR, ADR, Pred +/- cyclophosphamide and L-asparaginase in 8-12 weeks Short-course intensive chemotherapy Post-remission therapy Consolidation Intensification Maintenance Stem cell transplant (Auto or Allo SCT) CNS prophylaxis and treatment
 CNS prophylaxis and treatment.")
52
Induction chemotherapy for ALL
Modified from BFM protocol (Hoelzer et.al. Blood 1988)
")
53
Maintenance chemotherapy for ALL

54
Consolidation chemotherapy for ALL

55
Hyper-CVAD for Mature B and T-ALL

56
Results of induction chemotherapy
CR = 75-85%, long-term survival = 30-40%

57
Post-remission therapy
Standard-risk: no bad prognostic factor Standard consolidation chemotherapy, maintenance and CNS prophylaxis Stem cell transplant in second CR High-risk: at lease one poor prognostic factor except Ph chromosome or MRD+ after induction Intensified chemotherapy Stem cell transplant, preferably allogeneic, in first CR Very high-risk: Ph+ ALL Allogeneic stem cell transplant in first CR Search for unrelated donors or cord blood if no siblings Experimental therapy - autologous stem cell transplant with imatinib or antibody-purged grafts

58
Allogeneic SCT for high-risk ALL
Thomas, X. et al. J Clin Oncol; 22:

59
Allogeneic SCT in first CR also improve outcomes of standard risk ALL (MRC UKALL XII/ECOG E2993)
Blood 2008; 111:

60
How possible is relapsed ALL?
1 month prior, he was still in remission with normal bone marrow study including flow cytometry for minimal residual disease CBC now shows relatively preserved marrow function. Peripheral blood smear reveals no blast cells Relapse is, therefore, unlikely at this point but still requires bone marrow study for exclusion

61
Why is he so sensitive to MTX and 6-MP?
His dose of maintenance chemotherapy: 6–MP 25 mg daily and MTX 15 mg weekly ~ 50% reduction.

62
Rocha, J. C. C. et al. Blood 2005;105:4752-4758
Interaction of primary antileukemic agents with products of polymorphic genes Rocha, J. C. C. et al. Blood 2005;105: Copyright ©2005 American Society of Hematology. Copyright restrictions may apply.

63
TMPT Polymorphism and Outcomes of ALL Treatment with Standard Chemotherapy
About 1 in 300 individuals inherit TPMT deficiency as an autosomal recessive trait. Three particular TPMT alleles, designated as TPMT*2, TMPT*3A, and TPMT*3C, have been shown to account for nearly 95% of the observed cases of TPMT deficiency. Patients who carry TPMT polymorphisms are at risk for severe hematologic toxicities when treated with 6-MP because these polymorphisms lead to a decrease in the rate of 6-MP metabolism 6-MP dose intensity is a significant predictor of event-free survival in children with acute lymphatic leukemia (ALL)
")
64
TPMT Polymorphism in Thai Population
Hong-Eng et al. studied in 75 Thai children with acute leukemia. The frequency of TMPT heterozygote was 11%. TPMT*3C was the only allele found in Thailand.1 Subsequent study in general population also confirmed this finding.2 1 Hongeng et al. Med Pediatr Oncol Oct;35(4):410-4 2 Srimartpirom et al.Br J Clin Pharmacol. 2004; 58:66–70.
: Srimartpirom et al.Br J Clin Pharmacol. 2004; 58:66–70.")
65
How about the effects of methotrexate?
Macrocytosis Megaloblastic changes in bone marrow Potentiate bone marrow suppression effects of 6-MP Predispose to EBV-associated lymphoproliferative disease

66
Proposed pathogenesis of MTX-associated LPD

68
My Clinical Diagnosis Precursor B-lymphoblastic leukemia in complete remission TPMT deficiency due to genetic polymorphism TMPT*3C allele Atypical lymphoproliferative disease, probably EBV-associated

69
Further investigation
Bone marrow study: aspirate, biopsy and immunophenotyping Lymphocyte subset study and clonal determination by flow cytometry or TCR and/or Ig rearrangement analysis Abdominal imaging either by CT or ultrasound EBV Anti-VCA IgM, IgG, anti-HHV-6 IgM, IgG EBV-DNA, CMV-DNA, HHV-6 PCR?

70
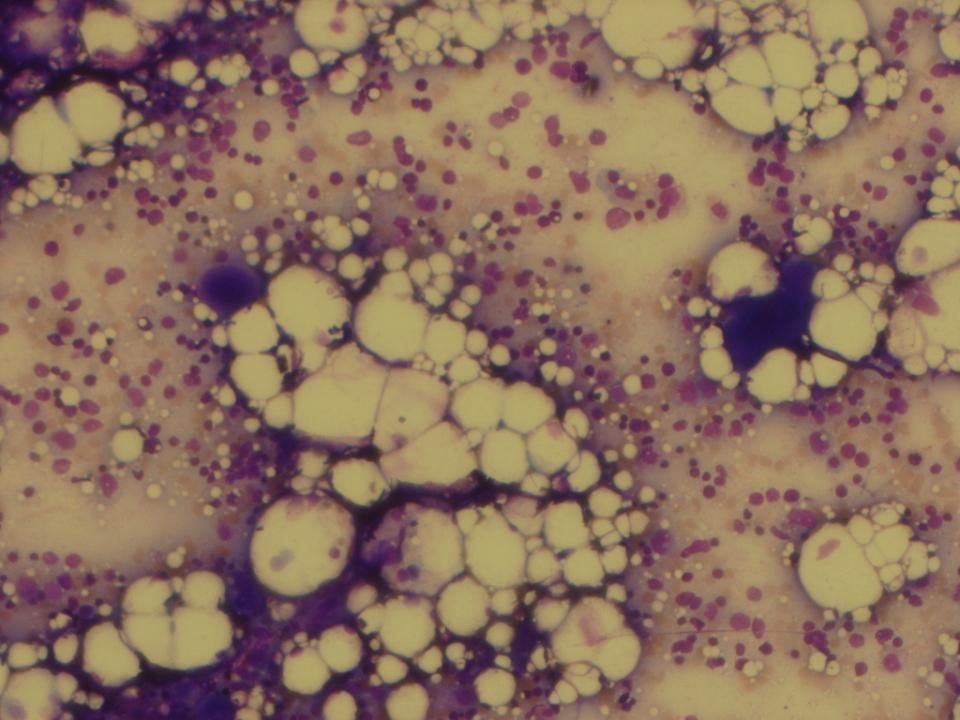
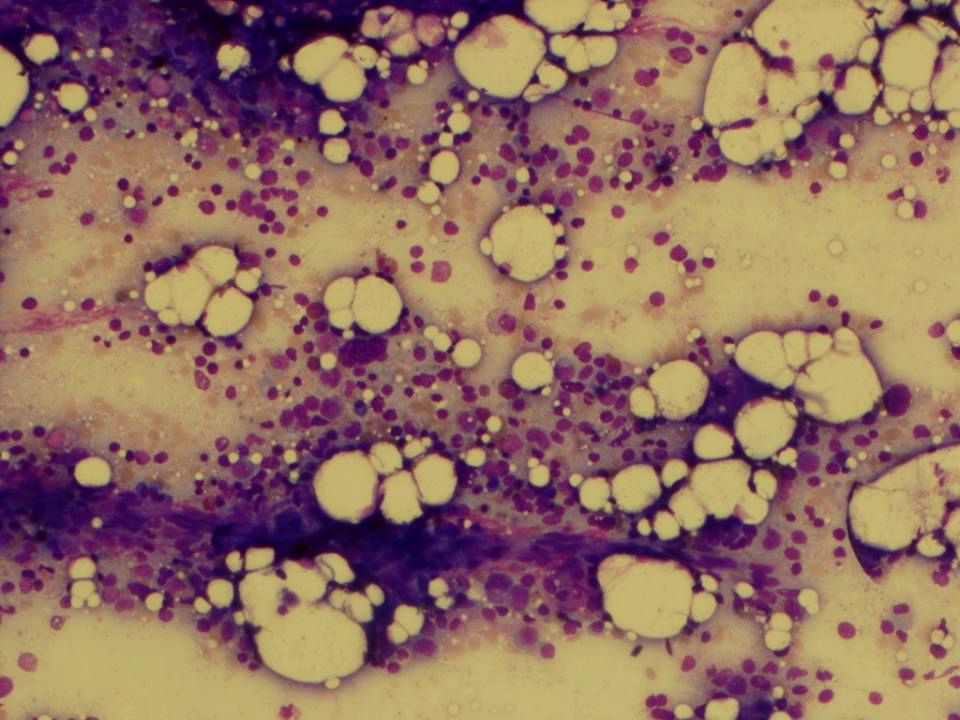
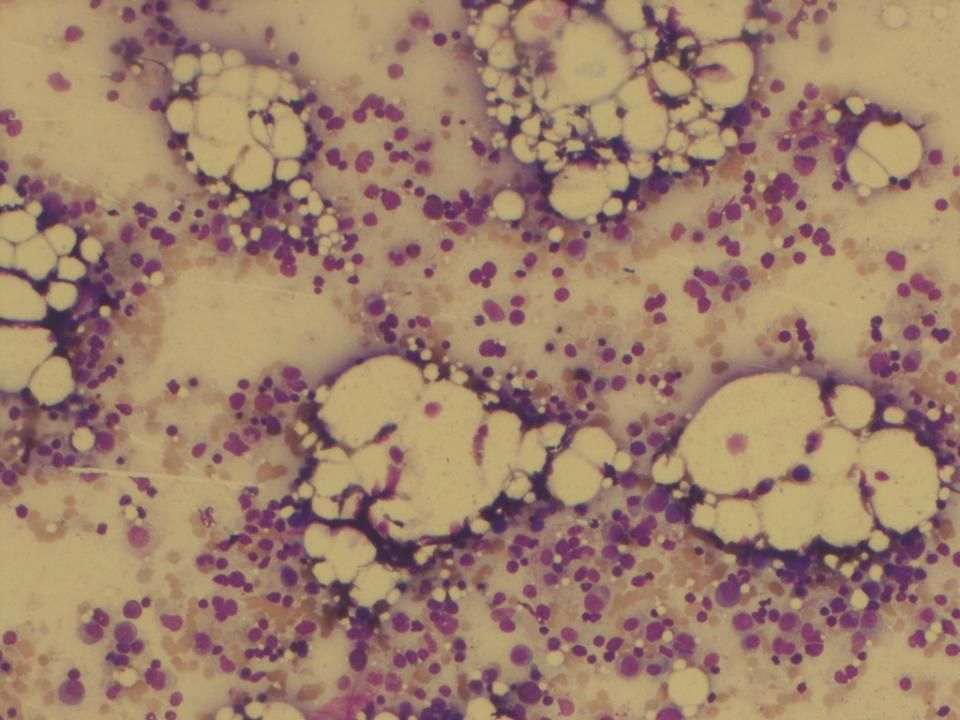
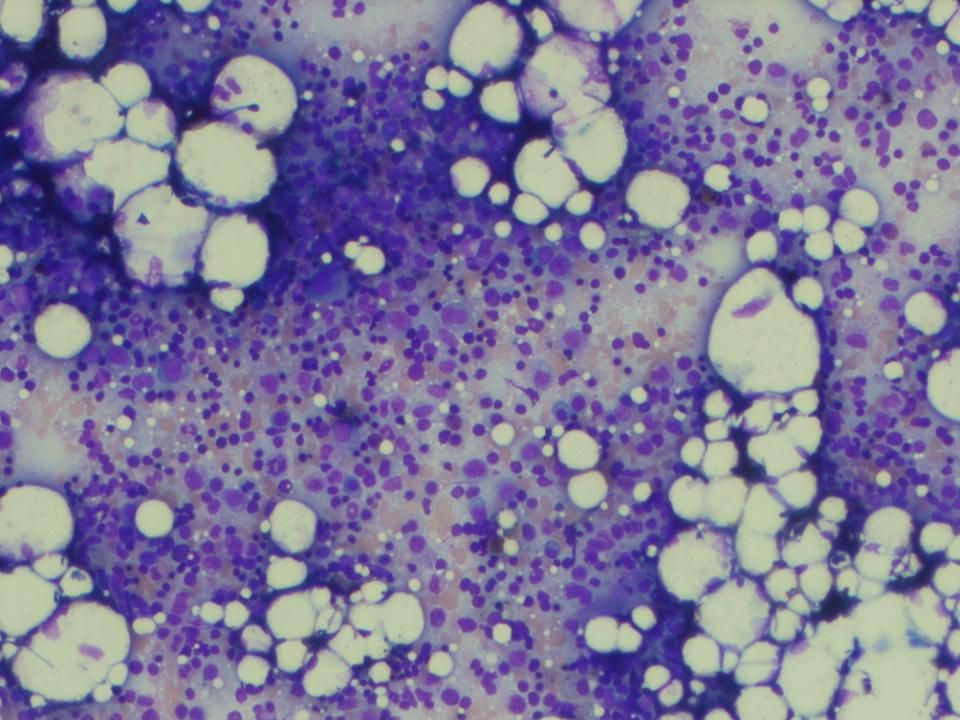
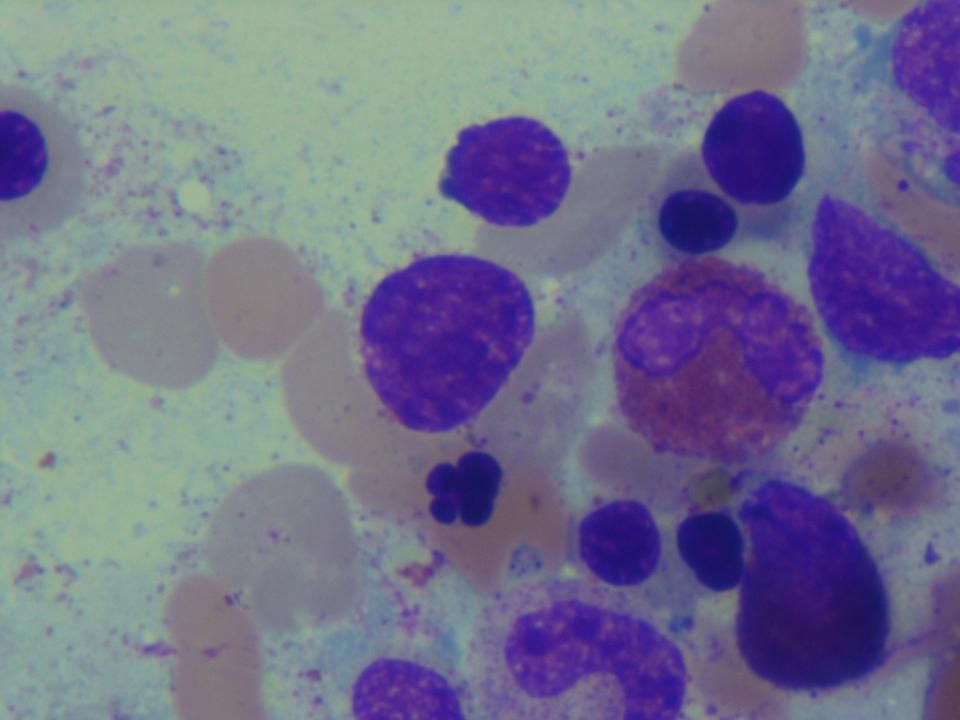
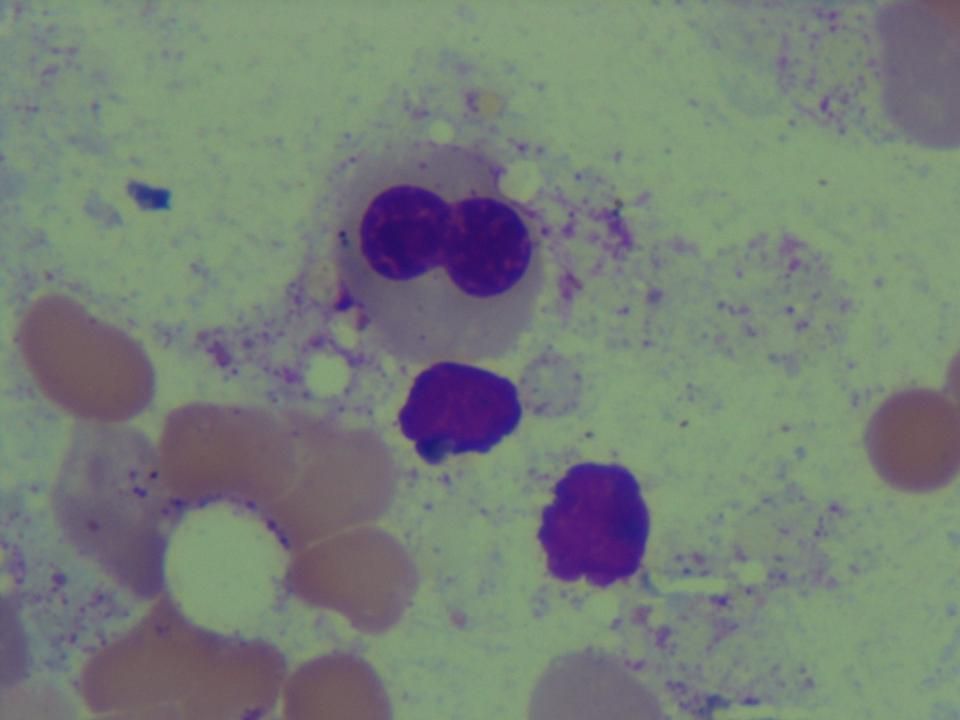
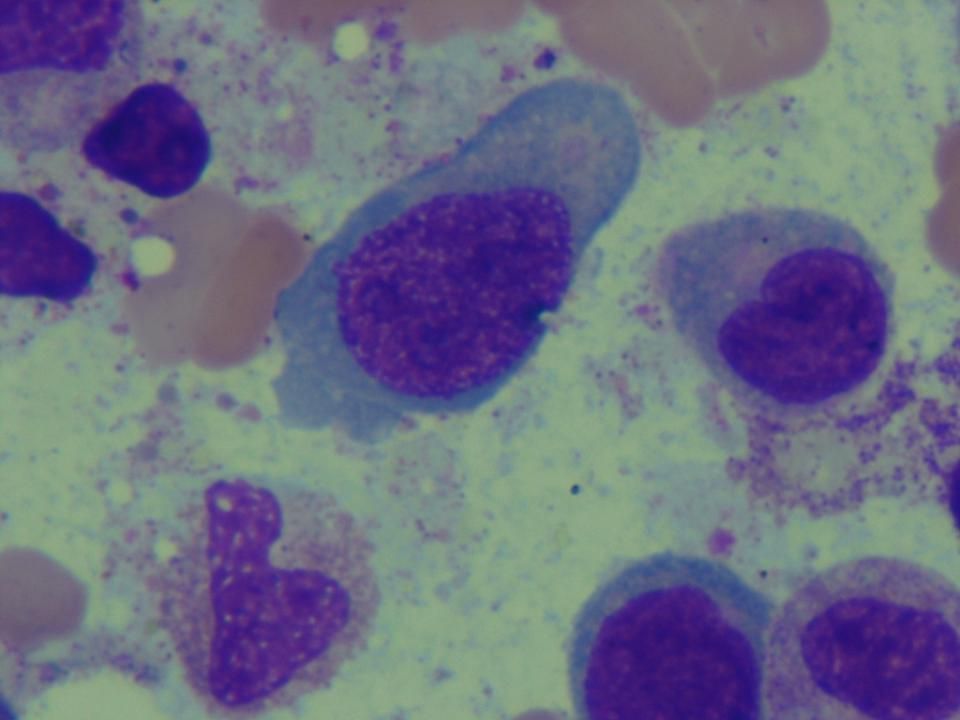
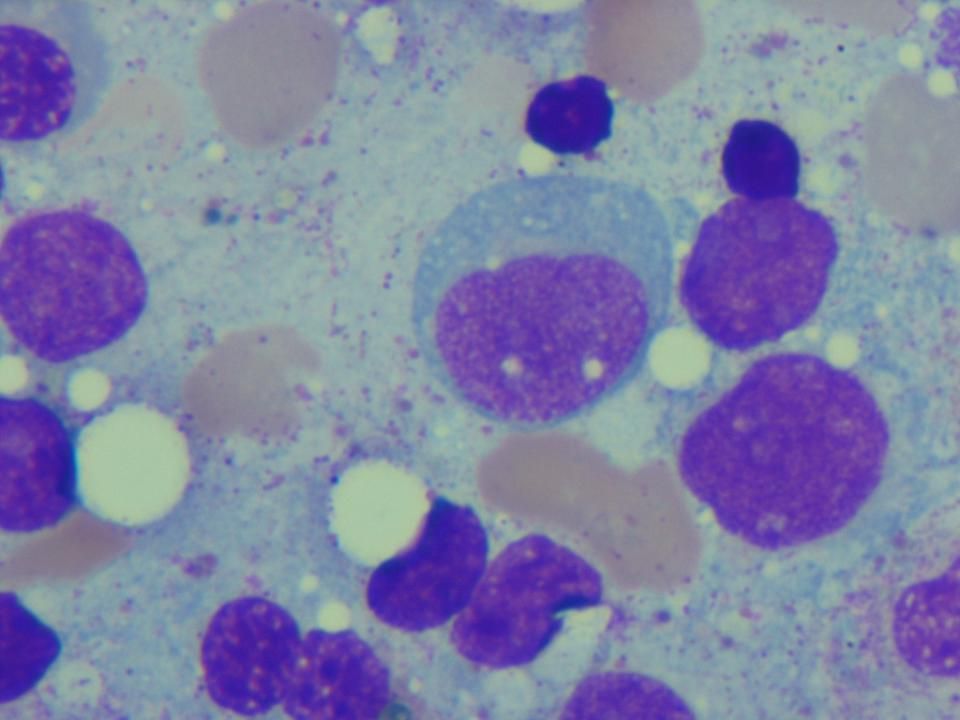
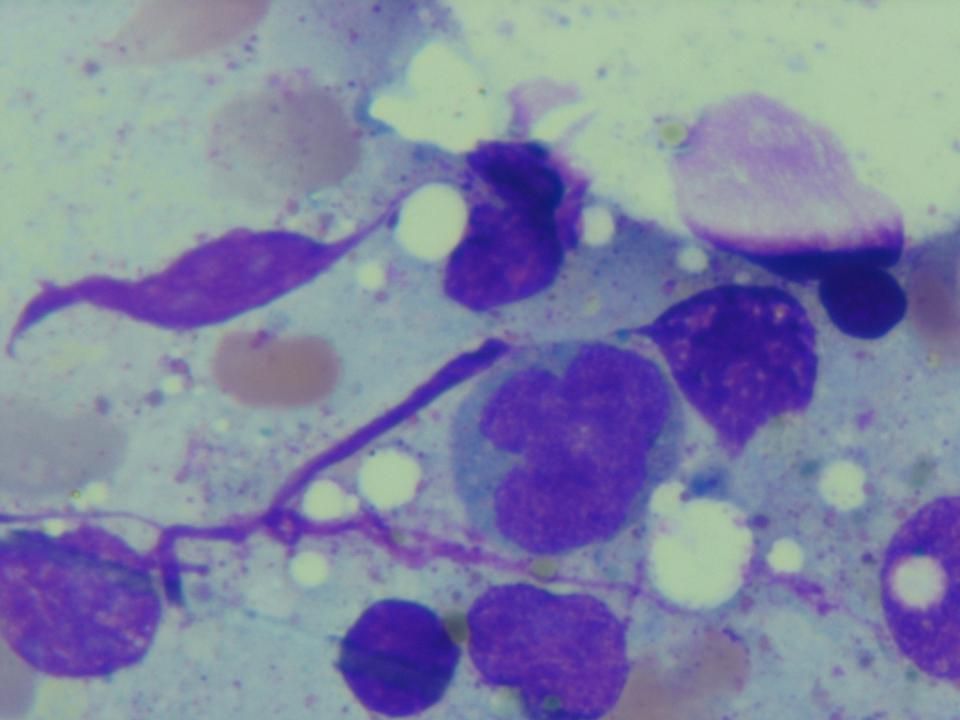
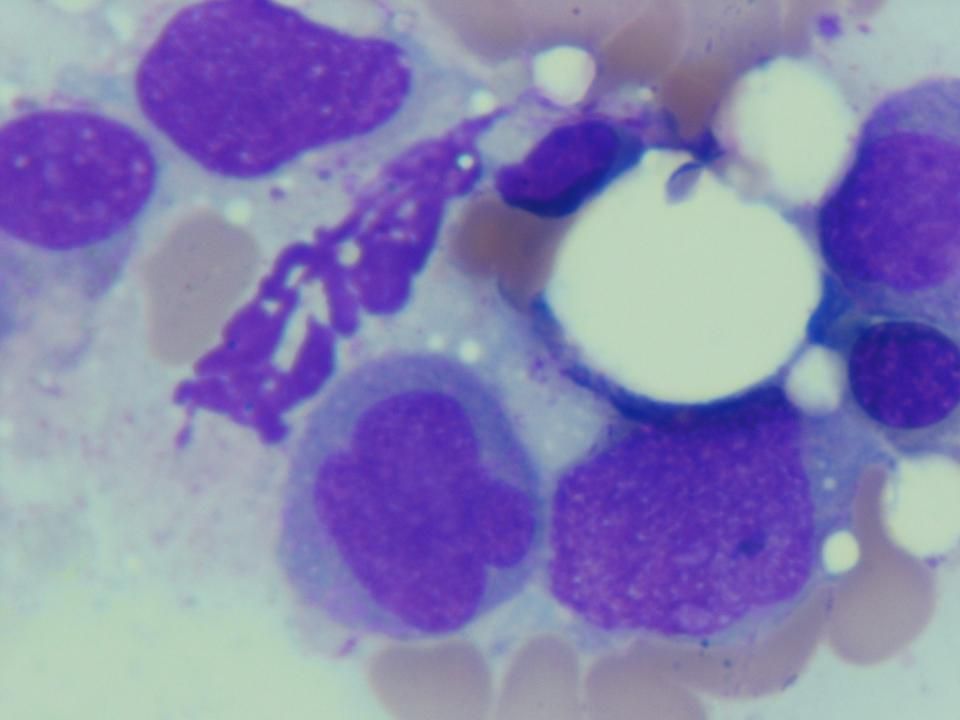
Bone marrow aspirate 25 April 2008

90
Investigation

91
Laboratory investigation
BMA : suboptimal specimen BM Bx : Moderately hypocellular bilineage marrow with markedly decreased mature granucytes : No histologic evidence of leukemia : AFB negative - BM PCR TB : negative

92
Laboratory investigation(1/5/51)
Scrub typhus Ab : negative EBV IgM : positive (15.229, cut off 10) EBV IgG : positive ( , cut off 5) EBV (EBNA) IgG positive ( , cut off 5) EBV viral load :< 100 copies Anti EBV IgM (ELISA test) negative (8.38, cut off 10) Anti EBV IgG (ELISA test) positive (115.65, cut off 5)
 EBV IgG : positive ( , cut off 5) EBV (EBNA) IgG positive ( , cut off 5) EBV viral load :< 100 copies. Anti EBV IgM (ELISA test) negative (8.38, cut off 10) Anti EBV IgG (ELISA test) positive (115.65, cut off 5)")
93
Laboratory investigation (1/5/51)
CMV IgM : positive (1.36, cut off 0.357) CMV IgG : negative CMV viral load : 28,300 Log equivalence : 4.45 Anti-CMV IgM : positive (1.369, cut off 0.357) Anti-CMV IgG : negative (8.58, cut off 40)
 CMV IgG : negative. CMV viral load : 28,300. Log equivalence : Anti-CMV IgM : positive (1.369, cut off 0.357) Anti-CMV IgG : negative (8.58, cut off 40)")
94
Laboratory investigation (15/5/51)
Anti EBV IgM (ELISA) : negative (8.384, cut off 10) Anti EBV IgG (ELISA): positive ( , cut off 5) EBV (EBNA) IgG: positive ( , cut off 5) Anti-CMV IgM : positive (2.04, cut off 0.408) Anti-CMV IgG : positive (77.73, cut off 40)
 : negative (8.384, cut off 10) Anti EBV IgG (ELISA): positive ( , cut off 5) EBV (EBNA) IgG: positive ( , cut off 5) Anti-CMV IgM : positive (2.04, cut off 0.408) Anti-CMV IgG : positive (77.73, cut off 40)")
95
Laboratory investigation
CBC 24/4/51 25/4/51 27/4/51 30/4/51 3/5/51 6/5/51 10/5/51 14/5/51 Hb 13.6 13.2 12.5 12.0 11.9 11.3 Hct 39.7 38.2 38.7 36.2 35.0 33.8 33.3 38.4 WBC 3.430 4,000 4,310 3,150 1,990 6,080 3,610 5,260 N (%) 86.3 79.9 38.3 26.4 27.1 - 24.2 24 L (%) 11.4 15.3 53.6 62.5 57.3 63.5 63 M (%) 1.7 3.5 3.2 7.3 11.1 6.4 E (%) 0.3 0.5 0.2 B (%) 1.3 4.9 3.8 4.0 5 6 Plt 53,000 42,000 23,000 21,000 52,000 49,000 79,000 125,000
 L (%) M (%) E (%) B (%) Plt. 53, , , , , , , ,000.")
96
Laboratory investigation
LFT 24/4/51 30/4/51 2/5/51 6/5/51 14/5/51 30/5/51 TP 6.4 6.7 - Albumin 4.0 3.6 4.3 Globulin 2.4 3.0 3.8 TB 0.50 0.64 0.65 0.48 0.58 DB 0.14 0.23 0.22 0.21 0.16 SGOT 37 273 219 132 34 SGPT 69 370 326 221 70 26 ALP 85 362 384 258 199

งานนำเสนอที่คล้ายกัน






















 98.08% 100.02% จังหวัด.>")


 MICU 68% CCU 32%>")