ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
Systemic therapy for Advanced Hepatoma & Cholagiocarcinoma
นายแพทย์ ชัยยุทธ เจริญธรรม หน่วยมะเร็งวิทยา ภาควิชาอายุรศาสตร์

2
แนวทางการรักษามะเร็งตับ (ระยะโรค, ความแข็งแรงผู้ป่วย, ความแข็งแรงของตับ)
HCC Stage D PST >2, Child–Pugh C Stage 0 PST 0, Child–Pugh A Stage A–C PST 0–2, Child–Pugh A–B Very early stage (0) 1 HCC <2cm Carcinoma in situ Early stage (A) 1 HCC or 3 nodules <3cm, PST 0 Intermediate stage (B) Multinodular, PST 0 Advanced stage (C) Portal invasion, N1, M1, PST 1–2 End stage (D) 1 HCC 3 nodules < 3 cm Portal pressure/ bilirubin Increased Associated diseases Normal No Yes Resection Transplantation Ablation TACE ยา รักษาประคับ ประคอง มีโอกาสหายขาด ระงับหรือบรรเทาโรค Adapted from Llovet JM, et al. J Natl Cancer Inst 2008;100: 2
 1 HCC <2cm Carcinoma in situ. Early stage (A) 1 HCC or 3 nodules <3cm, PST 0. Intermediate stage (B) Multinodular, PST 0. Advanced stage (C) Portal invasion, N1, M1, PST 1–2. End stage (D) 1 HCC. 3 nodules < 3 cm. Portal pressure/ bilirubin. Increased. Associated diseases. Normal. No. Yes. Resection. Transplantation. Ablation. TACE. ยา. รักษาประคับ. ประคอง. มีโอกาสหายขาด. ระงับหรือบรรเทาโรค. Adapted from Llovet JM, et al. J Natl Cancer Inst 2008;100:")
4
โอกาสการมีชีวิตรอดอย่างน้อย 3 เดือน
Patient characteristics Point Ascites Yes 2 No Abdominal pain Weight loss Child-Pugh grade C 5 B A Biochemistry Serum alkaline phosphatase (ALP), int. unit/L >200 3 ≤200 Total bilirubin >50 int. unit/L (2.9 mg/dL) >33 - ≤50 int. unit/l ( mg/dL) 1 ≤33 int unit/L (1.9 mg/dL) Urea >8.9 mmol/L (>25 mg/dL) ≤8.9 mmol/L (≤25 mg/dL) Tumor characteristics Portal vein thrombosis Tumor size Diffuse 4 >5 cm ≤5 cm Lung metastases Serum alpha-fetoprotein (AFP), ng/mL >400 ≤400 โอกาสการมีชีวิตรอดอย่างน้อย 3 เดือน Patients With Advanced HCC Not Amendable to Locoregional Therapy Prognosis Score อัตราการมีชีวิตที่ 3 เดือน, % Good 0-2 >81 3-6 72-80 7-8 66-69 Intermediate 9 63 10-12 51-59 13-14 42-47 15 38 Poor 16 33 17-19 21-29 20-22 10-17 ≥23 <10 Yau et al. Cancer 2008.
, int. unit/L. > ≤200. Total bilirubin. >50 int. unit/L (2.9 mg/dL) >33 - ≤50 int. unit/l ( mg/dL) 1. ≤33 int unit/L (1.9 mg/dL) Urea. >8.9 mmol/L (>25 mg/dL) ≤8.9 mmol/L (≤25 mg/dL) Tumor characteristics. Portal vein thrombosis. Tumor size. Diffuse. 4. >5 cm. ≤5 cm. Lung metastases. Serum alpha-fetoprotein (AFP), ng/mL. >400. ≤400. โอกาสการมีชีวิตรอดอย่างน้อย 3 เดือน. Patients With Advanced HCC. Not Amendable to Locoregional Therapy. Prognosis. Score. อัตราการมีชีวิตที่ 3 เดือน, % Good > Intermediate Poor ≥23. <10. Yau et al. Cancer")
5
อุปสรรคของการรักษามะเร็งตับด้วยยา
HCC tumor biology (พันธ์ดื้อ) disruption in p53 pathway : resistance to apoptosis DNA topoisomerase alpha over-expressed/ up-regulated : resistance to Topoisomerase inhibitors intrinsic drug resistance mediated by an enhanced cellular drug efflux mechanism – MDR1, p-gp, MRP Pharmacokinetic properties of cirrhotic liver (ตับไม่เอื้อ) total liver mass is reduced distortion of the liver architecture leads to significant intra-hepatic shunting and reduced extraction of protein-bound substances. affects the absorption, plasma protein binding, distribution and renal excretion of drugs.
 disruption in p53 pathway : resistance to apoptosis. DNA topoisomerase alpha over-expressed/ up-regulated : resistance to Topoisomerase inhibitors. intrinsic drug resistance mediated by an enhanced cellular drug efflux mechanism – MDR1, p-gp, MRP. Pharmacokinetic properties of cirrhotic liver (ตับไม่เอื้อ) total liver mass is reduced. distortion of the liver architecture leads to significant intra-hepatic shunting and reduced extraction of protein-bound substances. affects the absorption, plasma protein binding, distribution and renal excretion of drugs.")
6
ตัวอย่างของการศึกษาที่ใช้ยาเคมีบำบัด ในการรักษามะเร็งตับ
Chemotherapy Study N อัตราการ ตอบสนอง, % ระยะเวลาที่ รอดชีวิต, เดือน Cisplatin, Doxorubicin Lee et al. 37 18.9 7.3 Cisplatin, Interferon, Doxorubicin, 5-FU (PIAF) Yeo et al. 91 20.9 8.6 Gemcitabine Yang et al 28 17.8 4.6 Capecitabine Patt et al. 11 10.1 Gemcitabine, Oxaliplatin Louafi et al. 34 18 6.3 Capecitabine, Oxaliplatin Boige et al. 50 6 9.3 FOLFOX 4 Quin et al. 184 8.2 6.4 Doxorubicin 187 2.7 P 0.02 4.9 P 0.085
 Yeo et al Gemcitabine. Yang et al Capecitabine. Patt et al Gemcitabine, Oxaliplatin. Louafi et al Capecitabine, Oxaliplatin. Boige et al FOLFOX 4. Quin et al Doxorubicin P P")
7
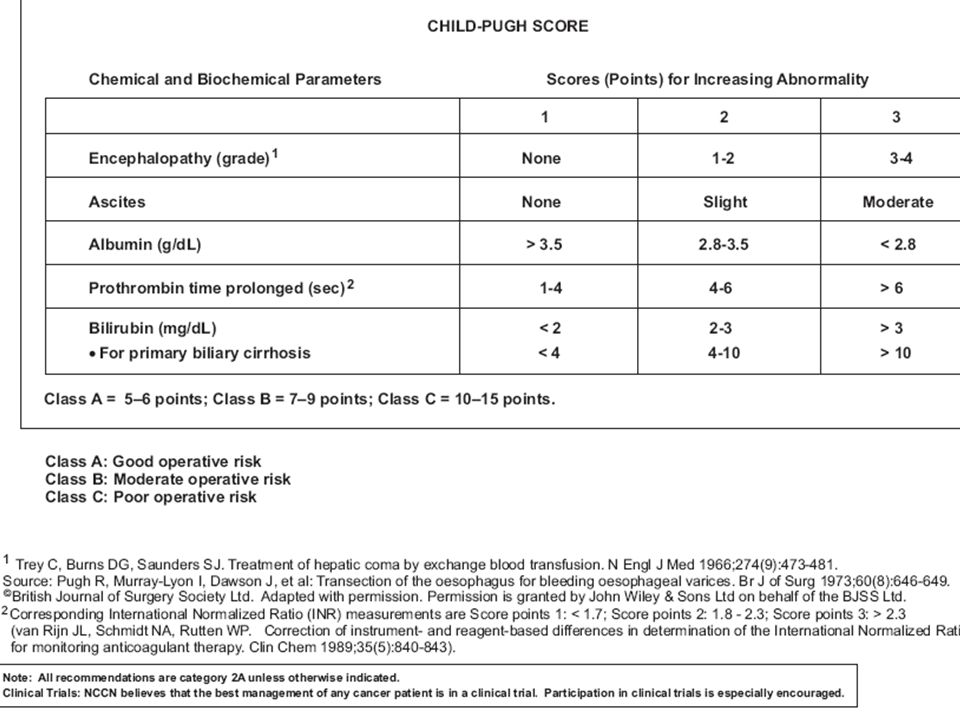
การใช้ยา Sorafenib NCCN 2013 APASL 2009 JSH 2010
For Unresectable HCC (tumor extent or location, liver function reserves), Child A or B APASL 2009 for advanced stage patients who are not suitable for loco-regional therapy and who have Child-Pugh liver function class A. (Grade A) may be used with caution in patients with Child-Pugh liver function class B. (Grade C) JSH 2010 Sorafenib is the first choice of treatment as a standard of care in Extrahepatic spread with Child-Pugh A liver function Sorafenib is also a treatment of choice for TACE refractory patients with Child-Pugh A liver function.
, Child A or B. APASL for advanced stage patients who are not suitable for loco-regional therapy and who have Child-Pugh liver function class A. (Grade A) may be used with caution in patients with Child-Pugh liver function class B. (Grade C) JSH Sorafenib is the first choice of treatment as a standard of care in Extrahepatic spread with Child-Pugh A liver function. Sorafenib is also a treatment of choice for TACE refractory patients with Child-Pugh A liver function.")
8
การศึกษาอ้างอิงที่ใช้ยา Sorafenib รักษามะเร็งตับ
SHARP1 Asia-Pacific2 1.00 1.00 Sorafenib (n=299) Median: 10.7 months Sorafenib (n=150) Median: 6.5 months 0.75 0.75 Placebo (n=303) Median: 7.9 months Placebo (n=76) Median: 4.2 months Survival Probability 0.50 Survival Probability 0.50 0.25 0.25 HR (S/P): 0.69 95% CI: P= HR (S/P): 0.68 95% CI: P=0.014 4 8 12 16 20 4 8 12 16 20 Months from Randomization Months from Randomization 1. Llovet JM, et al. N Engl J Med. 2008;359(4): 2. Cheng AL, et al. Lancet Oncol. 2009;10:25-34.
 Median: 10.7 months. Sorafenib (n=150) Median: 6.5 months Placebo (n=303) Median: 7.9 months. Placebo (n=76) Median: 4.2 months. Survival Probability Survival Probability HR (S/P): % CI: P= HR (S/P): % CI: P= Months from Randomization. Months from Randomization. 1. Llovet JM, et al. N Engl J Med. 2008;359(4): Cheng AL, et al. Lancet Oncol. 2009;10:")
9
การศึกษาอ้างอิงที่ใช้ยา Sorafenib รักษามะเร็งตับ
Sorafenib vs. placebo GIDEON (ASCO 2011) SHARP Asia-Pacific HBV/HCV/others 19/28/53 71/11/19 37/32/39 BCLC stage A/B/ C (%) 0/ 18/82 0/ 5/ 95 7/19/ 54 Child-Pugh A /B (%) 95/5 97/3 61/ 23 ECOG PS 0 / 1 +2 (%) 54/46 25/ 75 40 / 43 OS (months) 10.7 (S) 7.9 (P) 6.5 (S) 4.2 (P) 10.3 (C-P A) 4.8 (C-P B) TTP (months) 5.5 (S) 2,8 (P) 2.8 (S) 1.4 (P) 4.2 (C-P A) 3.6 (C-P B) GIDEON : Global Investigation of Therapeutic Decisions in Hepatocellular Carcinoma and of its Treatment with Sorafenib
 SHARP. Asia-Pacific. HBV/HCV/others. 19/28/53. 71/11/19. 37/32/39. BCLC stage A/B/ C (%) 0/ 18/82. 0/ 5/ 95. 7/19/ 54. Child-Pugh A /B (%) 95/5. 97/3. 61/ 23. ECOG PS 0 / 1 +2 (%) 54/46. 25/ / 43. OS (months) 10.7 (S) 7.9 (P) 6.5 (S) 4.2 (P) 10.3 (C-P A) 4.8 (C-P B) TTP (months) 5.5 (S) 2,8 (P) 2.8 (S) 1.4 (P) 4.2 (C-P A) 3.6 (C-P B) GIDEON : Global Investigation of Therapeutic Decisions in Hepatocellular Carcinoma and of its Treatment with Sorafenib.")
10
GIDEON study: Child-Pugh A vs. B
% of n Child-Pugh A (n=957) Child-Pugh B (n=367) Median treatment duration, weeks 14 9 Median daily dose, mg‡ 680 721 AEs (all Grades) 82 89 SAEs† 29 56 Drug-related SAEs‡ 8 15 Permanent discontinuation of sorafenib due to AE§ 24 38 Global Investigation of Therapeutic Decisions in Hepatocellular Carcinoma and of its Treatment with Sorafenib ASCO 2011
 Child-Pugh B (n=367) Median treatment duration, weeks Median daily dose, mg‡ AEs (all Grades) SAEs† Drug-related SAEs‡ Permanent discontinuation of sorafenib due to AE§ Global Investigation of Therapeutic Decisions in Hepatocellular Carcinoma and of its Treatment with Sorafenib. ASCO")
11
Sorafenib long-term data: Initial presentation of treatment-related AEs (any grade) by cycle
Most Sorafenib-treated patients first experienced HFSR and other common AEs within the first two treatment cycles Patients with AE (%) Cycle HTN, hypertension 1 cycle = 6 weeks Hutson TE, et al. Eur J Cancer 2010;46:2432–40. 11 11
 Cycle. HTN, hypertension. 1 cycle = 6 weeks. Hutson TE, et al. Eur J Cancer 2010;46:2432–")
12
อาการข้างเคียงจากการรักษาของ Sorafenib ในการศึกษาอ้างอิง SHARP & AP trial
Incidence by grade (%) SHARP1 Asia Pacific2 Sorafenib (n=297) Placebo (n=302) Sorafenib (n=149) Placebo (n=75) AE* Any 3-4 3–4 Overall incidence 80 52 81.9 38.7 Diarrhoea 39 8 11 2 25.5 6.0 5.3 Fatigue 22 4 16 3 20.1 3.4 8.0 1.3 HFSR 21 <1 45.0 10.7 2.7 Rash/desquamation 1 0.7 6.7 Alopecia 14 24.8 – Anorexia 12.8 Nausea 11.4 Hypertension 5 18.8 2.0 Nexavar was generally well tolerated with manageable AEs AEs associated with Nexavar were predominantly mild–moderate, and gastrointestinal, constitutional or dermatological in nature Most common drug-related AEs were HFSR, diarrhoea, alopecia, fatigue, rash/desquamation, hypertension, anorexia and nausea AEs (NCI-CTCAE v3.0) that occurred in at least 10% of patients in either study arm are listed. Nexavar® was generally well tolerated with manageable AEs (predominantly grade 1 or 2) the most common drug-related AEs were HFSR, diarrhoea, alopecia, fatigue, rash/desquamation, hypertension, anorexia and nausea this is a similar AE profile to that seen in the SHARP Trial. Grade 3–4 drug-related AEs that were reported more frequently in the Nexavar® group than in the placebo group included HFSR (10.7 vs 0%, respectively) and diarrhoea (6 vs 0%). Cheng A-L, et al. Efficacy and safety of sorafenib in patients in the Asia–Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol 2009;10:25–34. *AEs, as defined by CTCAE version 3.0 that occurred in at least 10% of patients in either study group 1. Llovet JM, et al. N Engl J Med. 2008;359(4): 2. Cheng AL, et al. Lancet Oncol. 2009;10:25-34.
 SHARP1. Asia Pacific2. Sorafenib (n=297) Placebo (n=302) Sorafenib (n=149) Placebo (n=75) AE* Any –4. Overall incidence Diarrhoea Fatigue HFSR. 21. < Rash/desquamation Alopecia – Anorexia Nausea Hypertension Nexavar was generally well tolerated with manageable AEs. AEs associated with Nexavar were predominantly mild–moderate, and gastrointestinal, constitutional or dermatological in nature. Most common drug-related AEs were HFSR, diarrhoea, alopecia, fatigue, rash/desquamation, hypertension, anorexia and nausea. AEs (NCI-CTCAE v3.0) that occurred in at least 10% of patients in either study arm are listed. Nexavar® was generally well tolerated with manageable AEs (predominantly grade 1 or 2) the most common drug-related AEs were HFSR, diarrhoea, alopecia, fatigue, rash/desquamation, hypertension, anorexia and nausea. this is a similar AE profile to that seen in the SHARP Trial. Grade 3–4 drug-related AEs that were reported more frequently in the Nexavar® group than in the placebo group included HFSR (10.7 vs 0%, respectively) and diarrhoea (6 vs 0%). Cheng A-L, et al. Efficacy and safety of sorafenib in patients in the Asia–Pacific. region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol 2009;10:25–34. *AEs, as defined by CTCAE version 3.0 that occurred in at least 10% of patients in either study group. 1. Llovet JM, et al. N Engl J Med. 2008;359(4): Cheng AL, et al. Lancet Oncol. 2009;10:")
13
Supportive measures (control callus, cream, cushion)
Suggested Interventions for skin toxicity (Sorafenib 800 mg/day) Grade 1 Grade 2 Grade 3 Supportive measures (control callus, cream, cushion) Topical therapy Decrease dose to 400mg/d for 7-28 days If symptoms resolve, increase to full dose If symptoms persist, interrupt treatment for 7 days Resume tx at 400mg QD when toxicity < grade 1 13
 Grade 1. Grade 2. Grade 3. Supportive measures (control callus, cream, cushion) Topical therapy. Decrease dose to 400mg/d for 7-28 days. If symptoms resolve, increase to full dose. If symptoms persist, interrupt treatment for 7 days. Resume tx at 400mg QD when toxicity < grade")
14
Supportive measures (control callus, cream, cushion)
Suggested Interventions for skin toxicity Grade 1 Grade 2 Grade 3 Supportive measures (control callus, cream, cushion) Topical therapy Interrupt treatment for 7 days Resume tx at 400mg/d when toxicity < grade 1 Consider further dose reduction if symptoms recur If toxicity < grade 1 for 7-28 days, may increase by one dose level 14
 Topical therapy. Interrupt treatment for 7 days. Resume tx at 400mg/d when toxicity < grade 1. Consider further dose reduction if symptoms recur. If toxicity < grade 1 for 7-28 days, may increase by one dose level. 14.")
15
N = 868 Patients with advanced HCC treated with SOR
Prophylactic effect of urea-based cream on the hand-foot skin reaction associated with sorafenib in advanced HCC N = 868 Patients with advanced HCC treated with SOR Urea-based cream was given twice daily for up to 12 weeks starting on Day 1 (Arm A) vs BSC was at the physician’s discretion and excluded urea-based creams. (Arm B) (1:1) Results All-grade HFSR - lower in Arm A (56.0%) vs Arm B (73.6%); p< Grade ≥2 HFSR tended to be lower in Arm A (21.9%) vs Arm B (29.2%), p= The median time to the first HFSR event was 2.5 fold longer in Arm A (84 days, 95% CI days) vs Arm B; (34 days, 95% CI days) , p<0.001. Ren et al. J Clin Oncol 30, 2012 (suppl; abstr 4008)
 vs BSC was at the physician’s discretion and excluded urea-based creams. (Arm B) (1:1) Results. All-grade HFSR - lower in Arm A (56.0%) vs Arm B (73.6%); p< Grade ≥2 HFSR tended to be lower in Arm A (21.9%) vs Arm B (29.2%), p= The median time to the first HFSR event was 2.5 fold longer in Arm A (84 days, 95% CI days) vs Arm B; (34 days, 95% CI days) , p< Ren et al. J Clin Oncol 30, 2012 (suppl; abstr 4008)")
16
Sorafenib unanswered questions
The mechanism of action of sorafenib in HCC that mediates clinical benefits Benefits/Safety in patients with Child B Optimal dose The mechanism of resistance

17
Phase III trials in advanced HCC
First-line Sorafenib/Doxorubicin vs Sorafenib/Placebo Sorafenib/Erlotinib vs Sorafenib/Placebo Sorafenib vs Sunitinib (failed, ASCO 2011) Sorafenib vs Brivanib Sorafenib vs Linifanib Second-line Brivanib vs BSC (failed, EASL 2012) Everolimus vs BSC Ramucirumab vs BSC ADI-PEG 20 vs BSC
 Sorafenib vs Brivanib. Sorafenib vs Linifanib. Second-line. Brivanib vs BSC (failed, EASL 2012) Everolimus vs BSC. Ramucirumab vs BSC. ADI-PEG 20 vs BSC.")
18
Conclusion : Systemic therapy for HCC
Sorafenib is the only approved systemic agent for the treatment of HCC Many other molecular-targeted agents are at the early stages of development in HCC Rational design clinical trial with combination therapy holds promise to improve outcome and remain to be seen

19
Systemic Therapy for Advanced Cholangiocarcinoma

20
Challenges of systemic therapy in Cholangiocarcinoma
Heterogeneous disease Gall bladder cancer Cholangiocarcinoma Intrahepatic cholangiocarcinoma (Peripheral type, mass forming) Extrahepatic cholangiocarcinoma Different location are truly the same pathology and biology ?
 Extrahepatic cholangiocarcinoma. Different location are truly the same pathology and biology")
21
Challenges to define standard chemotherapy for cholangiocarcinoma ?
Lack of well conducted randomized controlled trial Most studies are small, non randomized phase II Many studies comprise a mix of BTC, GBC and either PC or HCC.

22
Chemo :FELv, FLv (age >60,PS <70)
Overall survival : Chemo VS BSC 6 M VS 2.5 M, P <0.01 6 M VS 2.5 M, P=0.05, N=53 : PCA 6.5 M VS 2.5 M, P=0.1, N=37 : CCA Favorable QOL outcome : Chemo VS BSC – 36%VS10%,P <0.01 both sites Quality adjusted survival : Chemo VS BSC –4 M VS 1M,P <0.01 FELv /FLv Chemo :FELv, FLv (age >60,PS <70)
")
23
Chemotherapy in Cholangiocarcinoma
ยาเดี่ยว Fluoropyrimidine : 5-FU, capecitabine, tegafur, S1 Platinums : Cisplatin, carboplatin, oxaliplatin Antimetabolites : Gemcitabine, MMC Anthracyclines : Doxorubicin, Epirubicin Topoisomerase I inhibitors : Irinotecan Taxanes : Paclitaxel, Docetaxel สูตรยาคู่ FU + Platinums/ Gemcitabine Gemcitabine + Platinums/ FU สูตรผสมที่ใช้ยาตั้งแต่ 3 ตัวร่วมกัน – ECF, FAM, PIAF

24
104 trials (3 randomized, 112 trial arms), N = 2810
From January 1985 to July 2006 15% trials published 1993 – 1999 85% trials published after 2000 No. pt range from 5 – 65/trial (mean 25.1) Pooled RR = 22.6% (95% CI 21.0% %) Pooled TCR (tumor control rate=CR+PR+SD) = 57.3% TTP 4.1 months OS 8.2 months
 Pooled RR = 22.6% (95% CI 21.0% %) Pooled TCR (tumor control rate=CR+PR+SD) = 57.3% TTP 4.1 months. OS 8.2 months.")
25
Comparison of Regimens
2-drug VS 1-drug Higher RR 28.0 vs 15.3%, P=0.000 Higher TCR 61.0 vs 50.4%, P=0.000 Higher TTP 4.4 vs 3.4 months, P=0.015 Higher OS 9.3 vs 7.5 months, P=0.061 3 or more-drug VS 2-drug Lower RR 19.1 vs 28.0%, P=0.000 no difference in OS 9.0 vs 9.3 months 3 or more-drug VS 1-drug Higher TCR 58.9 vs 50.4%, P=0.028 Higher TTP 5.2 vs 3.4 months, P=0.016 Trend OS 9.0 vs 7.5 months, P=0.086

26
Gemcitabine (G) combined with P (cisplatin or oxaliplatin)
the highest increases RR and TCR provide best possible evidence that this combination chemotherapy may improve survival in these diseases Subgroup analysis concerning the three most important drugs demonstrated that G alone is not superior to FU Platinums increase the activity of both G and FU greater with G compared with the addition to FU

27
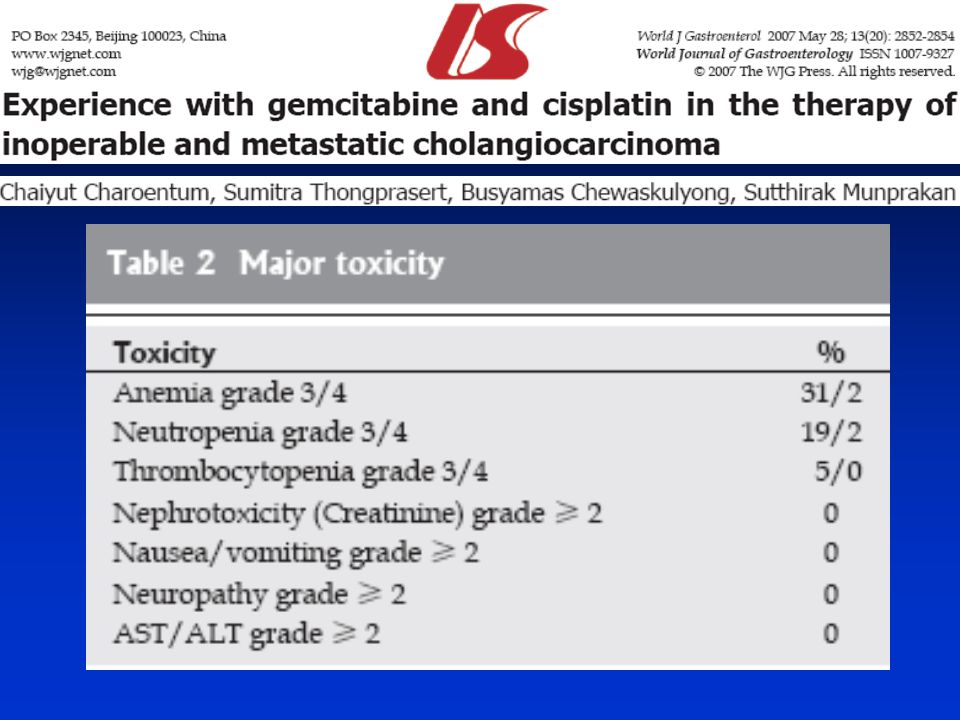
Gemcitabine 1250 mg/m2 in a 30-min infusion on d 1 and 8
Cisplatin mg/m2 on d1, 21-d cycle

29
RR 21%, TCR 52%, TTP 8.5 M, OS 10.5 M

30
Randomized studies of chemotherapy in biliary tract cancer

31
Randomized clinical trials using gemcitabine and cisplatin for advanced biliary tract cancer
gemcitabine 1000 mg/m2+ cisplatin 25 mg/m2 vs. gemcitabine 1000 mg/m2 alone Valle JW, et al. J Clin Oncol 2009;27(15s). Okusaka T,et al. Br J Cancer 2010;103(4):469–74.
. Okusaka T,et al. Br J Cancer 2010;103(4):469–74.")
32
Randomized clinical trials using gemcitabine and cisplatin for advanced biliary tract cancer
gemcitabine 1000 mg/m2+ cisplatin 25 mg/m2 vs. gemcitabine 1000 mg/m2 alone Valle JW, et al. J Clin Oncol 2009;27(15s). Okusaka T,et al. Br J Cancer 2010;103(4):469–74.
. Okusaka T,et al. Br J Cancer 2010;103(4):469–74.")
34
Target agents in development
N RR PFS OS Single target agent Erlotinib 39 BTC 25% Progression free at 6 M Philip et al. JCO HCC 35% Progression free at 6 M Lapatinib 17 BTC 0% M Ramanathan et al.ASCO 2006,abs HCC 12% M Sorafenib 31 BTC/GB 6% 2 M 6 M El-Khoueiry et al. ASCO 2007,abs 4639 Double target agents Erlotinib + Bevacizumab 6 GB 20% (20 evaluable) Holen et al. ASCO 2008, abs CCA Target agent + Chemotherapy Bevacizumab+ GemOX 10 BTC 27% (11 evaluable) Clark et al. ASCO 2007, abs GB Cetuximab + GemOx 22 BTC 58% (19 evaluable) Gruenberger et al. ASCO2008, abs 4586
 Holen et al. ASCO 2008, abs CCA. Target agent + Chemotherapy. Bevacizumab+ GemOX 10 BTC 27% (11 evaluable) Clark et al. ASCO 2007, abs GB. Cetuximab + GemOx 22 BTC 58% (19 evaluable) Gruenberger et al. ASCO2008, abs")
35
Conclusion : Systemic Therapy for CCA
Chemotherapy is the standard for advanced cholangiocarcinoma Level 1 evidence is gemcitabine and cisplatin Other combination regimens also have activity The future in this disease should lie in targeted therapies (which agent ?, combination?)
")
งานนำเสนอที่คล้ายกัน