ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
INTER-HOSPITAL CONFERENCE
21 DEC.2007

2
ผู้ป่วยชายไทยคู่ อายุ 40 ปี อาชีพ ข้าราชการครู ภูมิลำเนา จ. ปทุมธานี
CC: เจ็บที่ลิ้นด้านซ้าย 2 สัปดาห์ ก่อนมา ร.พ. PI : ~ 2 สัปดาห์ ก่อนมา ร.พ. มีแผลที่ลิ้นด้านซ้าย, เจ็บ, ไม่มีเลือดออก, ทำงานหนักพักผ่อนน้อย PHx. : - ปฏิเสธโรคประจำตัว - ปฏิเสธแพ้ยา - ดื่มสุรา, สูบบุหรี่เล็กน้อย หยุดมา 2 สัปดาห์

3
ประวัติเพิ่มเติม ได้รับการรักษาโดยแพทย์ หู คอ จมูก จากต่างจังหวัด โดยการจี้ยา และได้ยาทา ปฏิเสธฟันผุ, การใส่ฟันปลอม ปฏิเสธประวัติโรคมะเร็งในครอบครัว

4
Physical examination Thai male, not pale, no jaundice
v/s T 37˚C PR 80/min BP 120/80 mmHg Heart : normal Lung : clear Abdomen : soft, not tender, no hepatomegaly Neuro sing : WNL

5
ENT Examination AR : normal mucosa, no discharge
PR : no mass, no discharge OC : ulcerative lesion at Lt. lateral tongue size 0.5 x 0.5 cm. IDL : no mass, TVC move bilateral Neck : no palpable lymph node

6
Management?

7
BIOPSY : Negative for malignancy

8
DIFFERENTIAL DIAGNOSIS

9
ENT Examination OC : ulcerative lesion at Lt. lateral tongue size 0.5*0.5 cm., submucosal lesion 2*3cm., no limited tongue movement

11
INVESTIGATION

12
INVESTIGATION A . B . C . D . E .

13
DIAGNOSIS AND MANAGEMENT

14
DIAGNOSIS

15
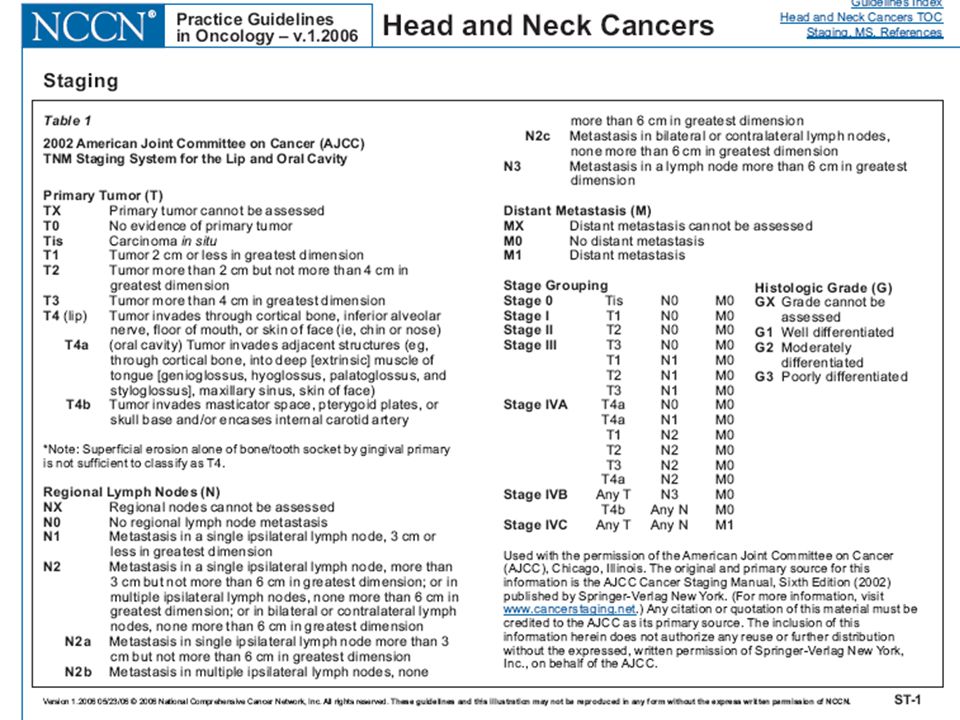
DIAGNOSIS CA Tongue T2N0M0

16
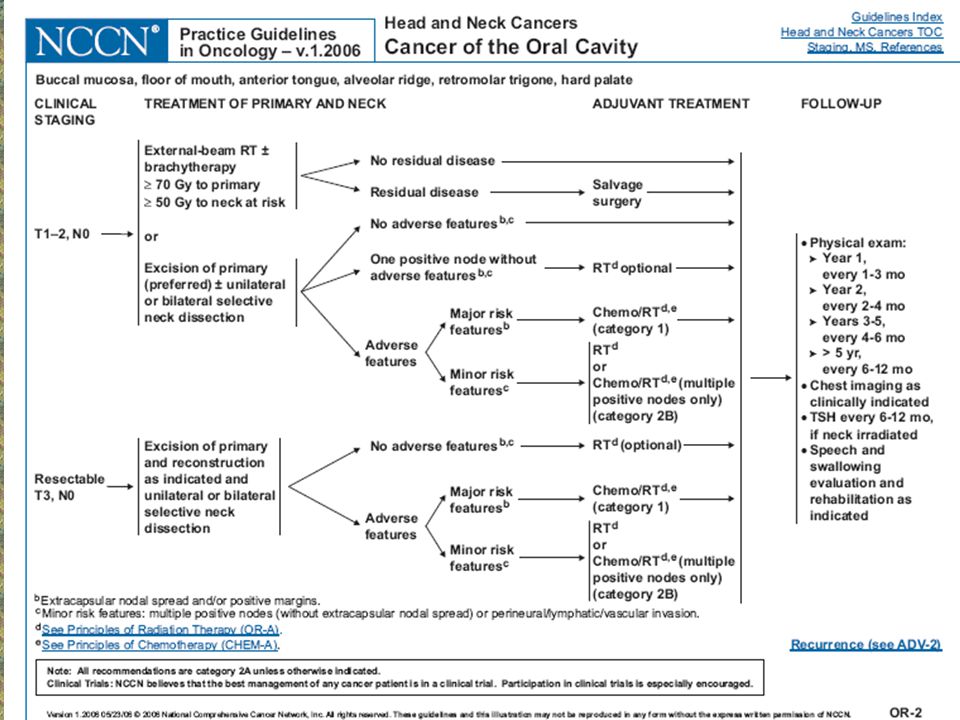
MANAGEMENT Surgery? RT?

17
MANAGEMENT Surgery? RT? Wide excision?

18
DIAGNOSIS AND MANAGEMENT
Dx. CA Tongue T2N0M0 Rx. Lt.Hemiglossectomy with primary closure with Lt. SND I-IV

19
Surgical Pathology Report
Tongue : consists of Lt. half portion of tongue, measuring 5*3*2.5 cm. The outer surface reveals an ulcerated light tan firm mass, measuring 2.7*1.8*0.8cm., occupying the Lt.half of tongue, 0.5 cm.from medial resected margin and 0.5 cm.from deep resected margin Lymph node group I-IV : No evidence of malignancy

20
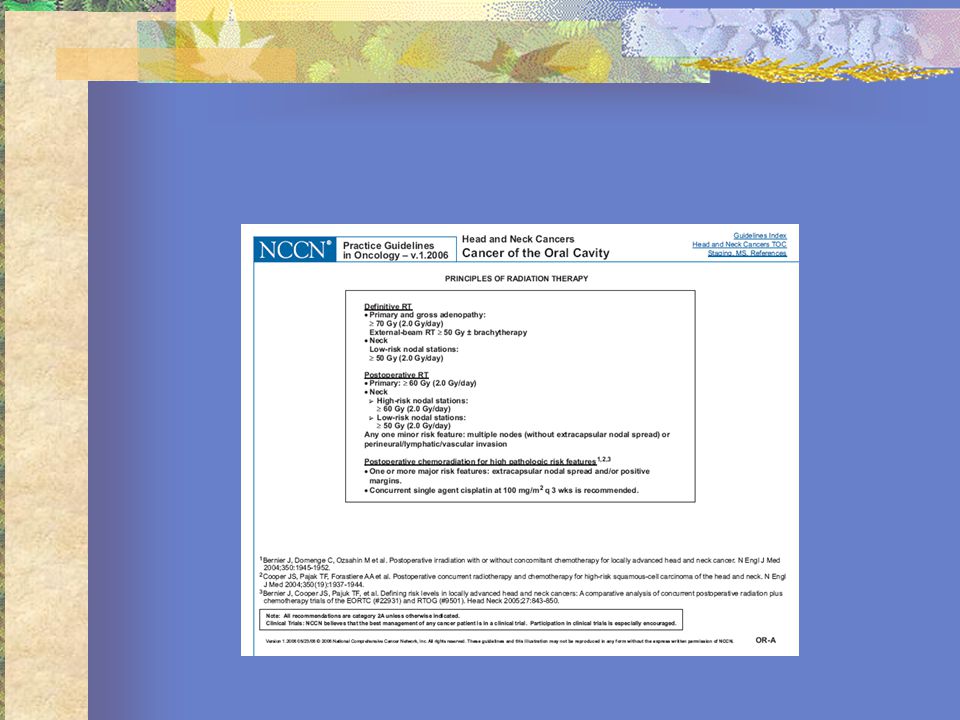
Management Combine Post-Op. RT ? Combine Chemotherapy ?

21
Management of the N0 Neck in CA Oral cavity

22
Evaluation of the N0 Neck
The reported false negative rate in assessing of cervical LN metastasis by palpation is 20%-50% Factor affecting : The experience of the examiner The patient’s body The previous treatment – Sx / RT

23
Evaluation of the N0 Neck
Structure in neck mistake Transverse process of atlas Carotid bifurcation Submandibular gland

24
Evaluation of the N0 Neck
Digital palpation CT / MRI Ultrasound Ultrasound guided FNAB

25
Evaluation of the N0 Neck
Malignancy criteria for CT/MRI LN > 15 mm. in level II LN > 10 mm. in other levels Group of ≥ 3 nodes ( 1-2 mm.) Central necrosis Loss of tissue planes ( fat plane)
 Central necrosis. Loss of tissue planes ( fat plane)")
26
N0 Neck affecting the recurrent/survival rate
Oral cavity CA Type N0 1 node 2 nodes ≥ 3 nodes 5 years survival 75% 49% 30% 15%

27
Therapeutic modalities for the N0 neck
Prophylactic Neck dissection Prophylactic Neck irradiation Observation with therapeutic ND once regional metastasis become appearance

28
The N0 neck in oral cavity CA
Byers et al : the prediction of nodal metas. In primary oral tongue SCCA The depth of muscle invasion N stage The degree of differentiation of the 1˚ tumor T1N0 with muscle invasion < 4 mm., WD 14% chance of nodal involvement

29
The N0 neck in oral cavity CA
SCCA of oral cavity the sites with < 20% occult metastasis : T1/T2 lip T1/T2 oral tongue < 4 mm in thickness T1/T2 FOM < 1.5 mm in thickness

30
Surgical therapy in the N0 neck with oral cavity CA
SOHND Minimal morbidity Reduces the risk of occult disease Avoid the undesirable side effect of RT ( RT is reserved for possible future tx. of second primary tumor )
")
31
RT in the N0 neck with oral cavity CA
An alternative treatment to SOHND PORT of the surgically treated primary tumor site, the neck has not been dissected, and the risk of occult regional dz. is substantial Primary tumor is treated with RT and the risk of occult node > 20%

32
Elective neck dissection VS Elective neck irradiation
ENI reduced neck failure rate in pt with control primary tumor and N0 neck from 18% to 1.9% In T1N0 SCCA oral tongue, ENI provided 95% control rate for neck recurrences compare with 38% without ENI Modality is chosen to Tx primary cancer may also help in formulating a decision as to how to tx the neck

33
Elective neck dissection VS Elective neck irradiation
Prophylactic neck RT provides equal control rate for neck metastasis to prophylactic ND

34
THANK YOU FOR YOUR ATTENTION

35
Combined modality of treatment
perineural spread intravascular spread intralymphatic spread + ve margin 2 histo. Positive LN multiple +ve LN extracapsular spread

36
Management of contralateral N0
14% incidence of involvement of contralateral neck node regardless of tumor stage If primary oral cavity cancer is midline location, bilaterally, along the tip of tongue or approaches or cross the midline

38
BASIC LAB . CBC : Hct. 36% WBC 11,200 ( N 72.2% L21% E 2.1% M 3.9%)
BUN 5 Cr 0.5 Na 137 K 4.3 Cl 106 CO2 25 FBS : 107 LFT : Alk.59 SGPT 12 SGOT 17 TB 0.63 TP Alb 4.6 EKG : Normal CXR : No active pulmonaly lesion

39
BIOPSY. Lt. Lateral tongue : Squamous cell carcinoma, moderate differentiated

40
@

42
N0 in early SCCA oral cavity
Most important prognostic factor in Mx of oral SCCA is status of cervical LN. Present of metastasis to cervical LN can reduce curative rate by 50% 3 Tx options are available. Observation with therapeutic ND once regional metastasis become appearance Elective neck RT Elective neck dissection

43
Morbidities of associated ENI
Xerostomia Dsyphagia Increased oral passage time Mucositis Pain Increased complication if salvage sx. Long duration of tx.

งานนำเสนอที่คล้ายกัน