ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
การเฝ้าระวังการติดเชื้อในโรงพยาบาล
สุจินดา ธิติเสรี 15 มิถุนายน 2558

2
Goal of infection control
Protect the patients Protect Healthcare worker/ visitors Cost effective manner

3
การติดเชื้อในโรงพยาบาล New Terminology
Nosocomial infection Hospital acquired infection Healthcare associated infections : HAI

4
ขณะแรกรับยังไม่ปรากฏอาการและไม่อยู่ในระยะ
Healthcare associated infection (HAI) การติดเชื้อที่สัมพันธ์กับบริการสุขภาพ ผู้ป่วยได้รับเชื้อขณะรับการตรวจ /รักษา ใน สถานพยาบาล ปรากฏอาการหลังเข้ารับการรักษาใน รพ. > 2 วัน (วัน admit = day1) เชื้อโรคอาจมาจากตัวผู้ป่วยเอง (endogenous) หรือรับเชื้อจากภายนอก (exogenous) : บุคลากร เครื่องมือ ขณะแรกรับยังไม่ปรากฏอาการและไม่อยู่ในระยะ ฟักตัวของโรค
 การติดเชื้อที่สัมพันธ์กับบริการสุขภาพ. ผู้ป่วยได้รับเชื้อขณะรับการตรวจ /รักษา ใน. สถานพยาบาล. ปรากฏอาการหลังเข้ารับการรักษาใน รพ. > 2 วัน. (วัน admit = day1) เชื้อโรคอาจมาจากตัวผู้ป่วยเอง (endogenous) หรือรับเชื้อจากภายนอก (exogenous) : บุคลากร เครื่องมือ. ขณะแรกรับยังไม่ปรากฏอาการและไม่อยู่ในระยะ. ฟักตัวของโรค.")
5
Key Responsibility of Infection Control
SURVEILLANCE Collect and analyze data Identify problems & Interventions (CQI) Monitor process compliance, outcome and feedback
 Monitor process compliance, outcome and feedback")
6
is an effective infection Prevention and control program
SURVEILLANCE is an effective infection Prevention and control program 6

7
Study on Efficacy of Nosocomial Infection Control : SENIC study (Haley et al ,1985)
4 point recommendation Surveillance Control measures Infection control nurse Hospital epidemiologist Best infection control program reduce rate of HAI by 32% No infection control program rate increased by 18%

8
Definition of surveillance
A comprehensive method of measuring outcomes and related processes of care, analyzing the data, and providing information to members of the healthcare team to assist in improving those outcomes and processes 8

10
จุดมุ่งหมายของการเฝ้าระวังการติดเชื้อ ในโรงพยาบาล
1. ทราบอัตราการติดเชื้อที่เป็นข้อมูลพื้นฐาน (endemic หรือ background rate) 2. ทราบว่ามีการเพิ่มขึ้นของอัตราการติดเชื้อสูงกว่าปกติ หรือไม่ (epidemic level หรือมี outbreak) 3. ทราบถึงปัจจัยเสี่ยง (leading process)ต่อการติดเชื้อ ในโรงพยาบาล 4. เพื่อประเมินผลการปฏิบัติตามแนวทางที่กำหนดว่ามี การปฏิบัติตามมากน้อยเพียงใด และมีผลในการลด การติดเชื้อหรือไม่ (compliance monitoring) 10
 2. ทราบว่ามีการเพิ่มขึ้นของอัตราการติดเชื้อสูงกว่าปกติ หรือไม่ (epidemic level หรือมี outbreak) 3. ทราบถึงปัจจัยเสี่ยง (leading process)ต่อการติดเชื้อ. ในโรงพยาบาล. 4. เพื่อประเมินผลการปฏิบัติตามแนวทางที่กำหนดว่ามี การปฏิบัติตามมากน้อยเพียงใด และมีผลในการลด. การติดเชื้อหรือไม่ (compliance monitoring) 10.")
12
Endpoint of HAI Surveillance
Data that demonstrate progress in HAI Prevention โครงการ Fighting VAP to Zero VAP /1000 vent days

13
Set goals to reset endemic rate of NI Nosocomial infections
Surveillance Set goals to reset endemic rate of NI Outbreak Nosocomial infections Endemic Rate New Infection Rate Identify outbreak Bring about changes in the risk of infections Intervention Time What we learn 13

14
Surveillance not only to obtain RATE but to do INTERVENTION

15
Surveillance of NI in Patients
- Hospital-wide Admit - Targeted Patient Post discharge SSI,PP-NB ER, OPD

16
Hospital-wide Surveillance
All patients All site of infections All wards, departments

17
Hospital-wide Surveillance
Advantage: Provide data on all units/ organisms/infection sites Cluster detection Establish baseline rates Recognizes outbreak early Cooperation Ward alert Easily implement control measures Disadvantages: Expensive, Labor-intensive, Large amounts of data collected and little time to analyze Difficult to develop interventions Not all infections are preventable

18
TARGETED SURVEILLANCE
Focus (target) on high-risk, high volume, problem-prone data relevant to the type of healthcare facilities Ventilator- associated pneumonia Catheter- associated UTI Surgical site infection Primary Bloodstream infection 18 18
 on high-risk, high volume, problem-prone. data relevant to the type of. healthcare facilities. Ventilator- associated pneumonia. Catheter- associated UTI. Surgical site infection. Primary Bloodstream infection")
19
Targeted Surveillance
Advantages Concentrates limited resources on high-risk areas Focuses on infections with known control measures to r educe infection risk Can determine valid denominator Flexible, can be mixed with other strategies Increases efficiency of surveillance Liberates ICP to perform other activities

20
Targeted Surveillance
Disadvantages Collects data only for targeted patients or risks Denominator data may be inadequate May miss clusters or outbreaks in nonsurveyed areas or populations

21
Post discharge Surveillance
Directly assessing the patients Reviewing records from visits to clinics or ER Contacting physicians or patients by mail or telephone

22
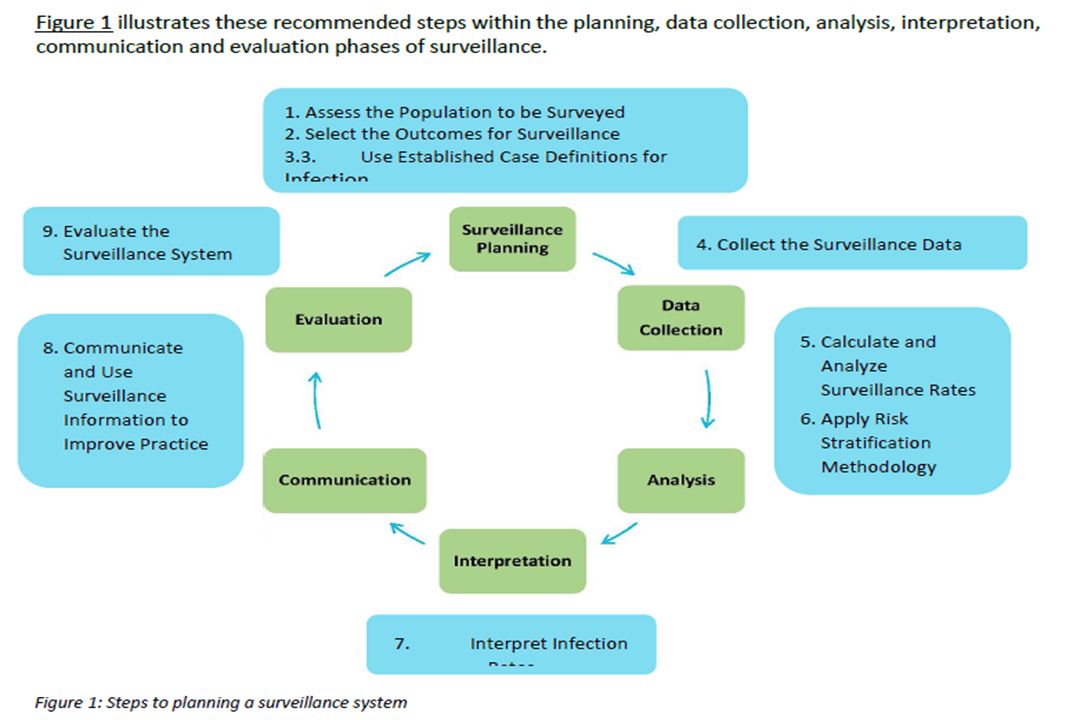
Recommended Practices for Surveillance
1. Assess the population 2. Select the outcome or process for surveillance 3. Use surveillance definitions 4. Collect surveillance data 5. Calculate and analyze infection rate 6. Apply risk stratification methodology 7. Report and use surveillance information AJIC Am J Infect Control 2007; 35 :

23
Patient Population “at-risk” for infection
1. Assess the population Patient Population “at-risk” for infection การเฝ้าระวังการติดเชื้อใน รพ. ระดับ Tertially Care Device-associated infections -Ventilator-associated pneumonia (VAP) -Central line associated BSI (CLABSI) -Cath. Assoc. UTI (CAUTI) Surgical Site Infection (SSI) Antibiotic-resistant organisms: CRE, PDR-GNB MDR-GNB, MRSA, VISA, VRE
 -Central line associated BSI (CLABSI) -Cath. Assoc. UTI (CAUTI) Surgical Site Infection (SSI) Antibiotic-resistant organisms: CRE, PDR-GNB. MDR-GNB, MRSA, VISA, VRE.")
24
Device Associated Risk
Infection risk increase with use of invasive devices High risk with longer duration More device Increased risk Increase infection

25
Patient Population “at-risk” for infection
What infections occur most commonly? What infections are likely to occur? Where are greatest opportunities to prevent infections? What are our most frequently performed procedures? What type of patients increase liability and/or costs for our hospital?

26
2. Select the outcome or process for surveillance
Outcome : the result of care or performance Infection Length of stay Patient satisfaction Examples CAUTI / 1000 Catheter days CLABSI / central line days Episiotomy infection / 100 ผู้คลอด

27
2. Select the outcome or process or surveillance
Process - กระบวนการที่ทำให้เกิด outcome Hand hygiene VAP , CLABSI , CAUTI bundle practices Timing of ATB prophylaxis Examples CAUTI bundle : % foley cath with appropriate indication VAP bundle : % compliance to VAP bundle MDRO bundle : environmental cleaning

28
Steps to achieve the outcome
Surveillance Collecting Tabulating Analyzing Reporting Processes Steps to achieve the outcome Outcome Result of Care Hand Hygiene Infection rate

29
3. Use Standard Surveillance Definitions
Must use written definitions to ensure accuracy of applying case definitions Use standardized, publish validated definition where available For accurate and valid comparisons, use the same definition

30
4. Collect surveillance data
Case finding ICN/ ICWN ผู้ที่ได้รับมอบหมายเฉพาะ หัวหน้าหอผู้ป่วย /sub head Maintain consistent surveillance intensity over time and across data collectors

31
Collection of Surveillance Data Who should collect infection data?
Active surveillance Trained epidemiology staff Discuss with ward More accurate infection data Sensitivity = 85 – 100 % (Pert, 1998) Passive surveillance Doctors or nurses report infections to ICN Generally results in under reporting of infections. Sensitivity : 14-34% (Pert, 1998)
 Passive surveillance. Doctors or nurses. report infections. to ICN. Generally results in. under reporting of. infections. Sensitivity : 14-34% (Pert, 1998)")
32
Prospective vs. Retrospective
Prospective surveillance initiated when patient is still under the care ข้อดี เห็นข้อมูลจริง (ตัวผู้ป่วย) / real time สอบถามข้อมูลจากพยาบาล /ผู้ป่วย เห็นอาการ /อาการแสดง ของผู้ป่วยที่อาจไม่ได้บันทึก ใน chart
 / real time. สอบถามข้อมูลจากพยาบาล /ผู้ป่วย. เห็นอาการ /อาการแสดง ของผู้ป่วยที่อาจไม่ได้บันทึก. ใน chart.")
33
Prospective vs. Retrospective
Retrospective surveillance Closed record review after patient has been discharge ข้อดี สำรวจข้อมูล หรือทบทวนเหตุการณ์ /เวชระเบียน ข้อด้อย ไม่สามารถแก้ปัญหา/Intervention ได้ทันที Not reliable or valid for HAI surveillance

34
Numerator Data Collection
Numerator = the “ Event” being measured case HAI จากการเฝ้าระวังแบบ Active surveillance - CAUTI, VAP, CLABSI ,SSI , Omphalitis Laboratory finding - MDR-GNB : A.baum, CRE - MRSA Care practice, Process, observation - Hand hygiene, IC bundle compliance

35
Data Collection form เก็บเฉพาะข้อมูลที่จำเป็น /ตามวัตถุประสงค์ สอดคล้องกับฐานข้อมูลเดิม

36
: population at risk or total possible
Denominator Data : population at risk or total possible ตัวอย่าง Number of surgical procedure or total # HH observation Denominator data collection may involve data necessary for risk adjustment - birth weight , ASA score - population at risk or total possible

37
การเก็บข้อมูล device day ต้องเหมือนกัน/เวลาเดียวกัน

38
device day, patient day : การติดเชื้อใน newborn แยกตามน้ำหนักแรกเกิด

39
5. Calculate and analyze infection rate 6
5. Calculate and analyze infection rate 6. Apply risk stratification methodology

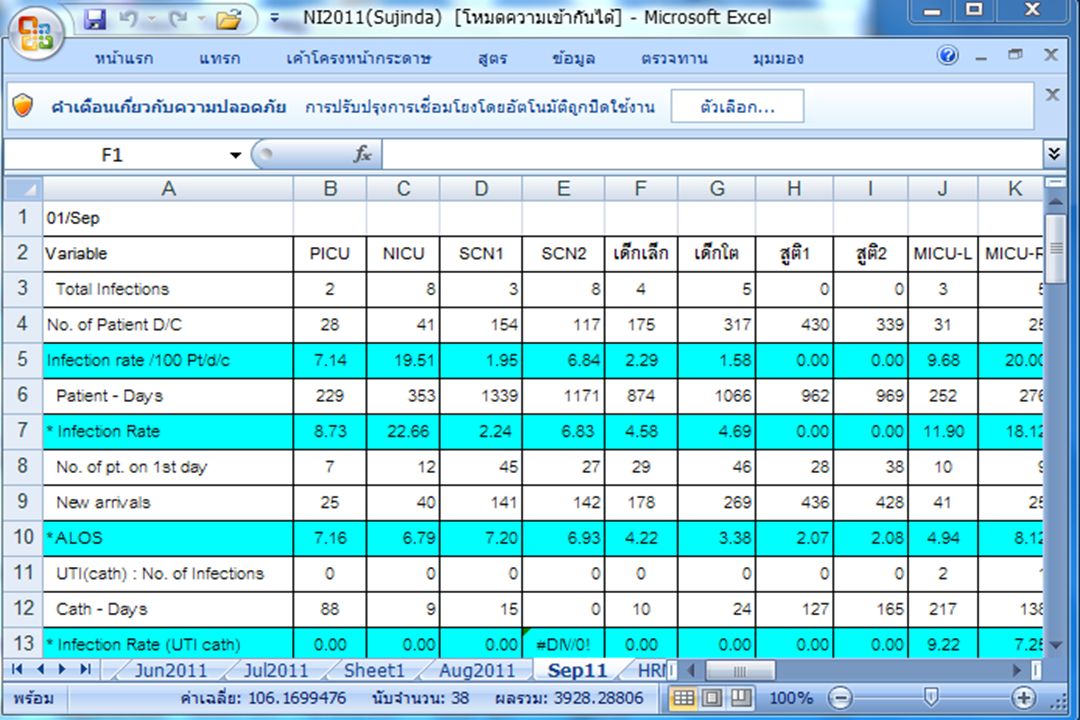
40
Calculating by denominator type
Infection Rate จำนวนครั้งของการติดเชื้อในเวลาที่กำหนด จำนวนวันนอนผู้ป่วยในช่วงเวลาเดียวกัน = X1000 Device associated infection จำนวนครั้งของการติดเชื้อตามชนิดdevice device day ในช่วงเวลาเดียวกัน = X1000 หน่วย : ต่อ วันนอน(Patient days) หรือ ต่อ device days 40
 หรือ ต่อ 1000 device days. 40.")
41
Calculating by Denominator type
จำนวนครั้งผู้ป่วยติดเชื้อ VAP X 1000 # Ventilator day ในช่วงเวลาเดียวกัน VAP rate = จำนวนครั้งผู้ป่วยติดเชื้อ CAUTI X 1000 # Catheter day ในช่วงเวลาเดียวกัน CAUTI rate = จำนวนครั้งผู้ป่วยติดเชื้อ CLABSI X 1000 # Central line day ในช่วงเวลาเดียวกัน CLABSI rate = 41

42
Calculating by Denominator type
surgical & procedures จำนวนครั้งผู้ป่วยติดเชื้อ SSI (Appendec) X 100 # APPY ช่วงเวลาเดียวกัน SSI rate = (Appendec) จำนวนครั้งผู้ป่วยติดเชื้อ Episio X 100 # ผู้ป่วยคลอด normal labour/episio ช่วงเวลาเดียวกัน Episiotomy = infection Rate 42
 X 100. # APPY ช่วงเวลาเดียวกัน. SSI rate = (Appendec) จำนวนครั้งผู้ป่วยติดเชื้อ Episio X 100. # ผู้ป่วยคลอด normal labour/episio. ช่วงเวลาเดียวกัน. Episiotomy = infection Rate. 42.")
44
Measure : Device Utilization (DU) Rate
# ventilator days X 100 # patient days Vent Utilization = rate # central line days X 100 # patient days Central line = Utilization rate

45
Device Utilization Rate
Measurement of wards invasive practices - extrinsic risk factor Indicator of severity of illness - intrinsic risk factor

46
Percentage of Maharat HAI (สัดส่วนของการติดเชื้อในรพ
Percentage of Maharat HAI (สัดส่วนของการติดเชื้อในรพ.) (Device + Non-device) Oct 13- Sep 14 จำนวนครั้งการติดเชื้อทั้งหมด ปี = ครั้ง
 (Device + Non-device) Oct 13- Sep 14. จำนวนครั้งการติดเชื้อทั้งหมด ปี 2557 = 1266 ครั้ง.")
47
3 Major Device-Associated Infection Rate (No
3 Major Device-Associated Infection Rate (No.Infections/1000 device days) Oct 13- Sep 14 SSI = 0.41 /100 procedures 47
 Oct 13- Sep 14. SSI = 0.41 /100 procedures. 47.")
48
VAP in 4 Major Departments (2551–2557)
VAP /1000 Vent days

49
VAP and Ventilator Utilization (2551 – 2557)
VAP / 1000 Vent days

50
Adjusting Rates Adjusting rates for exposure to devices
Adjusting rates for length of stay Adjusting rates for exposure to devices Adjusting rates for severity of illness

51
อัตราการติดเชื้อ CLABSI แยกตามน้ำหนักแรกเกิด
SSI : Abd. hysterectomy เทียบกับ NHSN อัตราการติดเชื้อ CLABSI แยกตามน้ำหนักแรกเกิด SSI by Risk index

52
อัตราการทำความสะอาดมือ (%) ตุลาคม 56 – กันยายน 57
อัตราการทำความสะอาดมือ (%) ตุลาคม 56 – กันยายน 57 ร้อยละ
 ตุลาคม 56 – กันยายน 57. ร้อยละ.")
53
Healthcare-associated Infections
Is not expected to be ZERO Is not entirely preventable Rates should be monitored and compared to benchmark level

54
กำหนด BENCHMARK รายงานข้อมูลแบบมี Benchmak :
internal (self-compare, compare with overall hospital rates) external (NHSN , UHOSNET) เปรียบเทียบข้อมูลรายเดือน, รายไตรมาส, รายปี Best practice = 25th percentile ward รู้ status จาก : trend over time (graph), benchmark
 external (NHSN , UHOSNET) เปรียบเทียบข้อมูลรายเดือน, รายไตรมาส, รายปี Best practice = 25th percentile. ward รู้ status จาก : trend over time (graph), benchmark.")
55
Infection Rates vs. UHOSNET
2553 2554 2555 2556 2557 UHOSNET VAP 6.09 5.54 6.92 6.98 6.15 < 8 CLABSI 3.13 2.54 2.20 1.72 0.92 < 3.25 CAUTI 2.18 1.88 1.90 1.52 1.31 < 2 หน่วย = / 1,000 device days 55

56
แ P25 =4.95 VAP 2014 (Mean = / 1,000 Vent. days Trend Over Time

57
high-outliers (>P90) กำหนดเป็น high-risk units (ผู้ป่วยไม่ปลอดภัย)
ทำอย่างไรต่อไป ?

58
โครงการ Fighting VAP to Zero
อัตราการติดเชื้อ 2552 2553 2554 UHOSNET VAP/1000 vent days 8.06 6.09 5.54 <8 VAP champion VAP /1000 vent days

59
CQI ลดการติดเชื้อ CLABSI : หน่วยทารกแรกเกิด
CLABSI bundle compliance CLABSI Rate CLABSI bundle 1 ปรับนิยาม ร้อยละ CLABSI bundle 2 CLABSI / 1000 Line days

60
Surveillance without action
should be abandoned

งานนำเสนอที่คล้ายกัน












 within the product or service. An item is classified as a.>")





 6 กรกฎาคม 2559>")
 พฤษภาคม 2561.>")