ดาวน์โหลดงานนำเสนอ
งานนำเสนอกำลังจะดาวน์โหลด โปรดรอ

1
ระบบคัดกรองผู้ป่วย (Triage)
ผศ.พญ.รพีพร โรจน์แสงเรือง ภาควิชาเวชศาสตร์ฉุกเฉิน คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี

2
One stop service-admission
ลงทะเบียนประวัติ ตรวจสอบสิทธิผู้ป่วย Admission center

3
“triage” มาจากภาษาฝรั่งเศสที่ว่า“trier”แปลว่า to “sort” or “choose”.
ถูกใช้ครั้งแรกในกองทัพในสงคราม

4
ระบบในการจำแนกผู้ป่วยตามลำดับความรุนแรงของโรค ซึ่งได้มีการริเริ่มมาตั้งแต่สมัยสงครามโลกครั้งที่ 1โดยนายแพทย์ชาวฝรั่งเศสชื่อ Dominique Jean Larrey

5
ในสมัยนั้นการจำแนกได้กระทำโดยการ “เดา” เป็นหลัก และเน้นคัดกรองเพื่อให้ได้รับการรักษาอย่างรวดเร็วมากกว่าความแม่นยำ

6
ระบบการคัดกรอง Simple Triage Advanced triage
Continuous Integrated Triage Reverse Triage

7
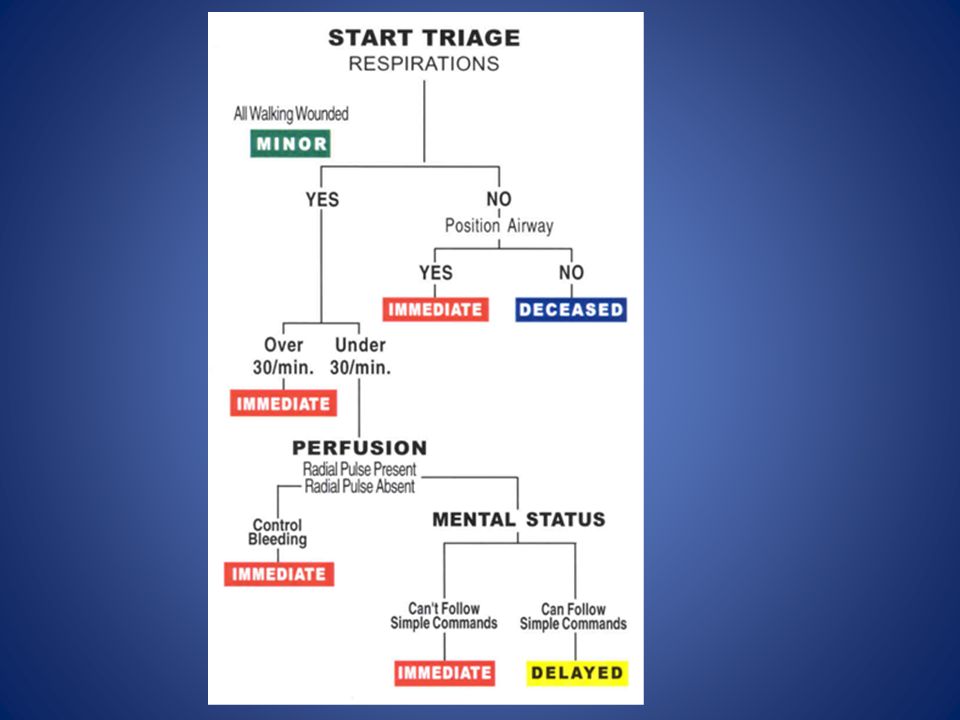
Simple Triage ใช้ในกรณีที่มี อุบัติภัยหมู่ (Mass Casualty Incident) เพื่อที่จะจำแนกผู้ป่วยที่ต้องได้รับการดูแลอย่างเร่งด่วนและนำส่งโรงพยาบาลก่อนออกมาเป็นลำดับแรก S.T.A.R.T. (Simple Triage and Rapid Treatment) เป็นระบบการจำแนกผู้ป่วยแบบที่สามารถใช้ได้ง่ายโดยผ่านการฝึกฝนเพียงเล็กน้อยก็ทำได้ ในอุบัติภัยหมู่หลายเหตุการณ์
 เพื่อที่จะจำแนกผู้ป่วยที่ต้องได้รับการดูแลอย่างเร่งด่วนและนำส่งโรงพยาบาลก่อนออกมาเป็นลำดับแรก. S.T.A.R.T. (Simple Triage and Rapid Treatment) เป็นระบบการจำแนกผู้ป่วยแบบที่สามารถใช้ได้ง่ายโดยผ่านการฝึกฝนเพียงเล็กน้อยก็ทำได้ ในอุบัติภัยหมู่หลายเหตุการณ์")
8
ระบบ S.T.A.R.T จะแบ่งผู้บาดเจ็บออกเป็น 4 กลุ่มดังนี้
0 deceased เกินความสามารถในการช่วยเหลือ 1 immediate transport ผู้บาดเจ็บต้องได้รับการนำส่งทันที 2 delayed transport การนำส่งสามารถรอได้ 3 minor injuries บาดเจ็บเล็กน้อยสามารถรอการช่วยเหลือเป็นลำดับท้ายได้

10
Advanced triage เลือกได้ว่าผู้บาดเจ็บรุนแรงรายใดที่ไม่ควรได้รับการช่วยเหลือเนื่องจากมีอัตรารอดชีวิตต่ำ คำนึงถึงการให้ความช่วยเหลือแก่ผู้ที่มีโอกาสรอดชีวิตได้มาก แทนการทุ่มกำลังไปเพื่อช่วยเหลือผู้ป่วยที่มีอาการรุนแรงและมีโอกาสเสียชีวิตในที่สุด การจำแนกระบบนี้มีปัญหาทางจริยธรรม Triage Revised Trauma Score (TRTS) Injury Severity Score (ISS)
 Injury Severity Score (ISS)")
11
Continuous Integrated Triage
ระบบที่ใช้ในสถานการณ์ที่มีอุบัติภัยหมู่ มีความจำเพาะสูง , สามารถจำแนกผู้บาดเจ็บที่ต้องการความช่วยเหลือก่อนได้ดี และ มีการบริหารทรัพยากรอย่างคุ้มค่า

12
Continuous Integrated Triage มีได้หลายระดับดังนี้
Group (Global) Triage (i.e., M.A.S.S. triage) Physiologic (Individual) Triage (i.e., S.T.A.R.T.) Hospital Triage (i.e., E.S.I. or Emergency Severity Index)
 Triage (i.e., M.A.S.S. triage) Physiologic (Individual) Triage (i.e., S.T.A.R.T.) Hospital Triage (i.e., E.S.I. or Emergency Severity Index)")
13
Reverse Triage ในบางสถานการณ์ซึ่งผู้ที่ได้รับบาดเจ็บเล็กน้อยอาจจำเป็นต้องได้รับการช่วยเหลือก่อนผู้ที่เจ็บหนัก ดังเช่น ในภาวะสงคราม ทั้งนี้เพื่อให้ผู้บาดเจ็บเล็กน้อยเหล่านั้นฟื้นสภาพร่างกายได้เร็วพอจนสามารถคืนกลับไปสู่กองทัพได้อีกครั้ง กรณีที่เป็นเหตุการณ์อุบัติภัยหมู่และมีบุคลากรทางการแพทย์ได้รับบาดเจ็บเป็นจำนวนมาก การช่วยบุคลากรทางการแพทย์เหล่านี้ก่อนก็เพื่อที่จะให้สามารถกลับไปปฏิบัติหน้าที่

14
Labelling of patients triage tag

15
Undertriage and overtriage

16
Undertriage การประเมินความรุนแรงการบาดเจ็บที่ต่ำกว่าความเป็นจริง เช่นผู้บาดเจ็บระดับ 1 ซึ่งอาการหนักและต้องได้รับการดูแลรักษาอย่างรีบด่วนแต่ถูกประเมินเป็นระดับ 2 หรือ 3 ใน Triage System ใดๆนั้น สามารถยอมรับอัตราของ undertriage ได้ไม่เกินร้อยละ 5 ทั้งนี้เพราะ undertriageเป็นการประเมินผู้ป่วยต่ำกว่าอาการรุนแรงแท้จริงของผู้ป่วย นั่นย่อมทำให้เกิดอันตรายต่อชีวิตของผู้ป่วยได้มากกว่า

17
Overtraige การประเมินความรุนแรงการบาดเจ็บที่มากเกินความเป็นจริง กล่าวคือ ประเมินผู้บาดเจ็บระดับ 3 เป็น ระดับที่ 2 หรือ 1 เป็นต้น ยอมรับการ overtriage ได้ไม่เกินร้อยละ 50 ของการประเมินทั้งหมด

18
Emergency Severity Index (ESI)
")
19
5 ระดับ ระดับ 1 (most urgent) - ระดับ 5 (least urgent)
แบ่งตาม acuity และ resource needs ESI concept in 1998

20
ประโยชน์ improvements in ED operations
support for research and surveillance for benchmarking

21
The purpose of ED triage
to prioritize incoming patients and to identify those patients who cannot wait to be seen to cope with overcrowding there is a critical need for a valid, reliable triage acuity rating system in order to sort these incoming patients more rapidly and accurately

22
The 3-level acuity-rating scale
emergent, urgent, and nonurgent unclear, not uniform and are often hospital dependent and nurse dependent

23
One option for the overcrowded ED is to try to control the “front end”

24
ESI (USA) Canadian Triage and Acuity Scale (CTAS) Australasian Triage Scale (ATS) Manchester Triage Scale (U.K.)
 Canadian Triage and Acuity Scale (CTAS) Australasian Triage Scale (ATS) Manchester Triage Scale (U.K.)")
25
สัมพันธ์กับ resource needed
outcome data( such as admission rates, ED length of stay and mortality rates) interrater reliability
 interrater reliability.")
26
Getting the right patient to the right resources at the right place and at the right time.

27
5 level triage system

28
ESI (v.4)
")
30
Major difference between ESI and CTAS and the ATS
the triage scales from Australia, Canada and the U.K. is that the purpose of triage is to determine how long the patient can wait for care in the ED.

31
ESI ESI does not define expected time intervals to physician evaluation. expected resource needs (e.g.,diagnostic tests and procedures), in addition to acuity
, in addition to acuity.")
32
สัมพันธ์กับ resources used in the ED
outcomes such as hospitalization, ED length of stay, and mortality Higher acuity patients (ESI levels 1 and 2) consumed more resources and were more likely to be admitted to the hospital
 consumed more resources and were more likely to be admitted to the hospital.")
33
Many believe that a complete assessment need not be done at the initial triage station, but rather can occur in the main treatment area or secondary triage area.

34
Only the assessment is required at triage in order to facilitate the initial sorting of patients.
Complete clinical assessments (at triage) can delay care and reduce satisfaction for patients with more minor emergencies.
 can delay care and reduce satisfaction for patients with more minor emergencies.")
35
“I need a bed for a level 2 patient,” and through this common language, the charge nurse understands what is needed without a detailed explanation of the patient by the triage nurse.

36
The Emergency Severity Index(ESI)
")
37
meet high acuity level criteria (ESI level 1 or 2)
expected resource needs(ESI level 3, 4, or 5) by the stability of vital functions and potential for life, limb, or organ threat based on previous experience
 by the stability of vital functions and potential for life, limb, or. organ threat. based on previous experience.")
38
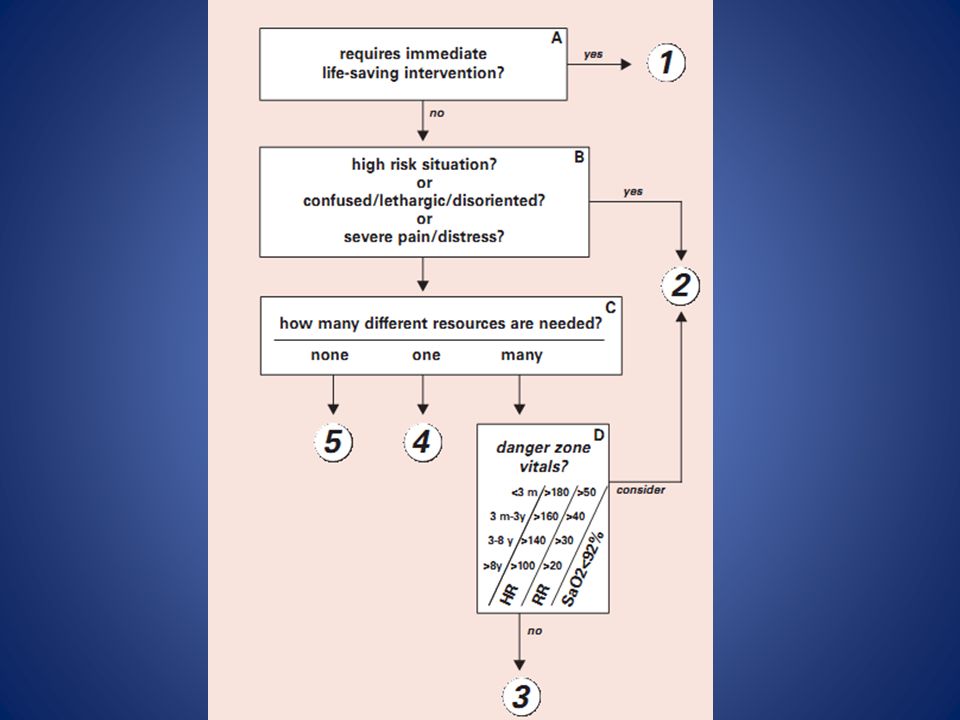
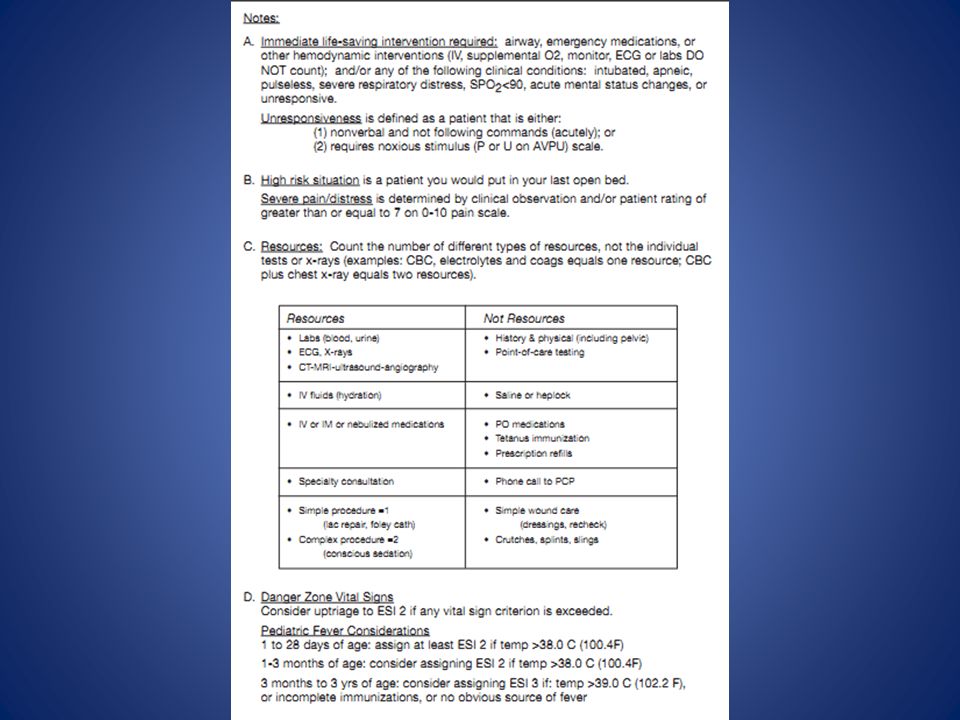
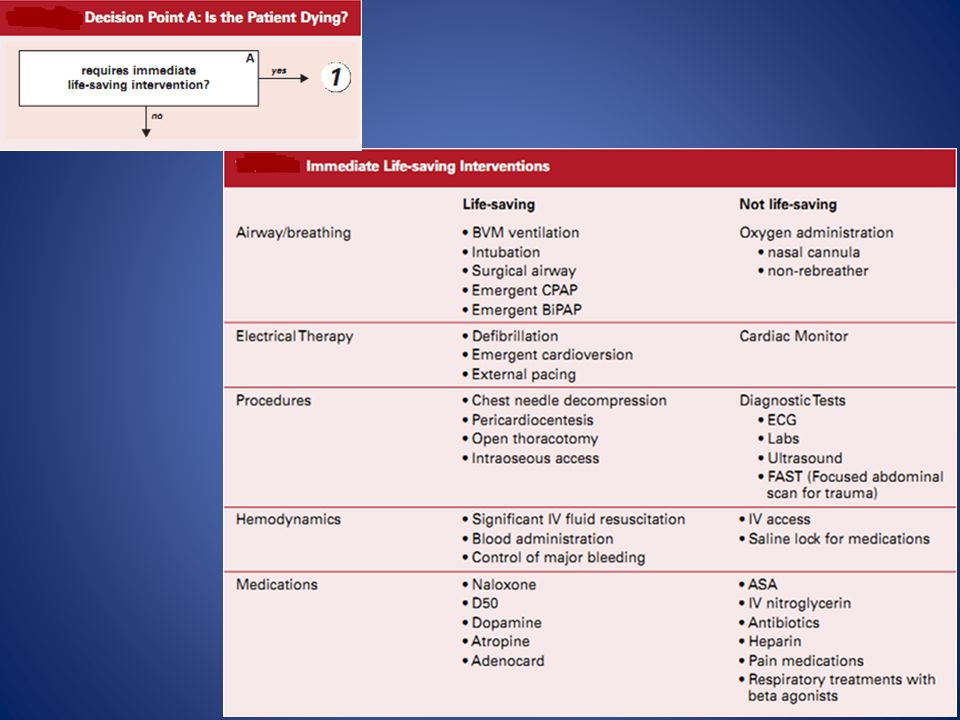
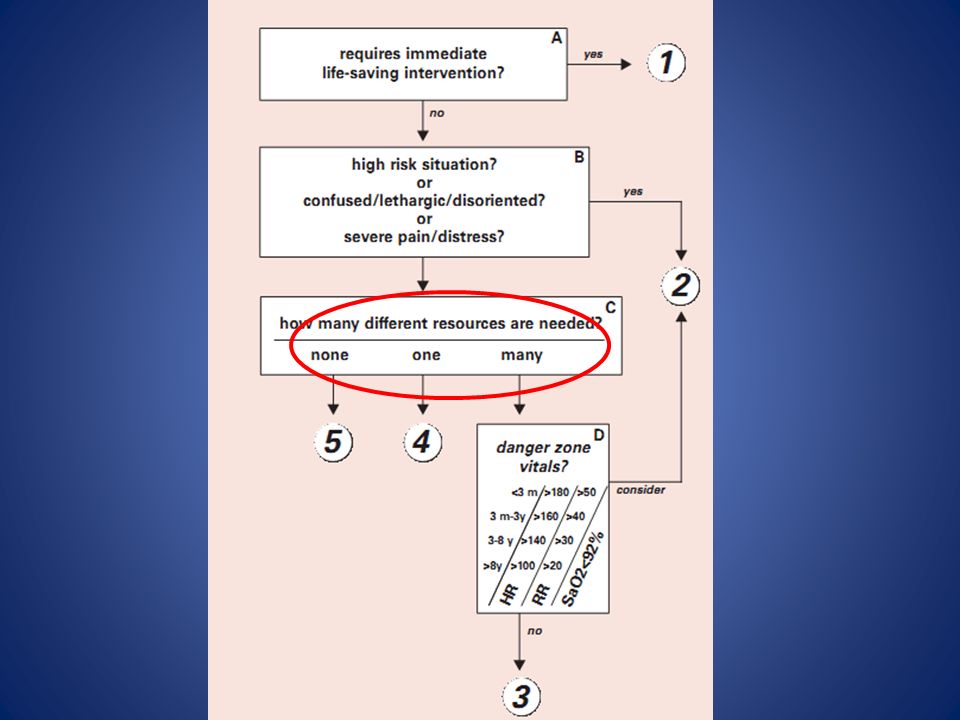
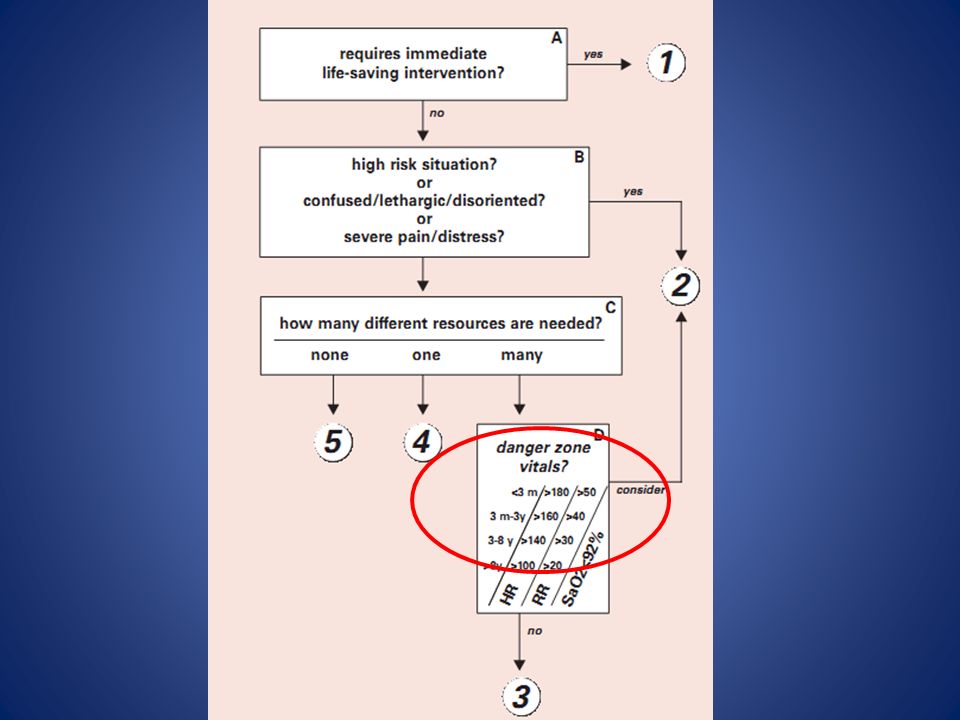
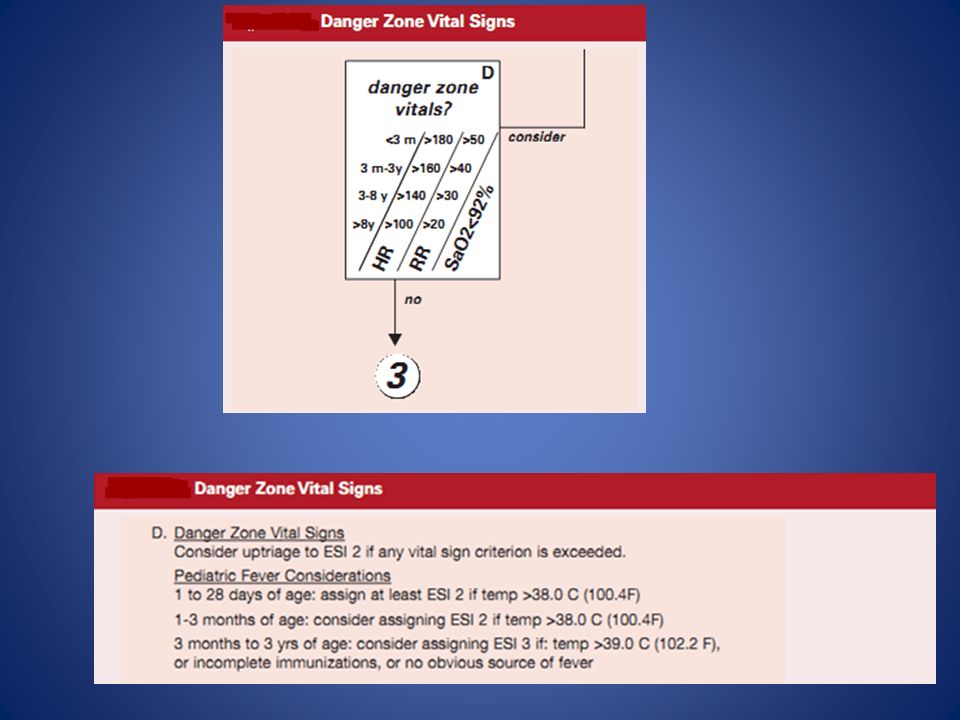
4 key questions A. dying? B. shouldn't wait? C. many resources?
D. vital signs?

44
Life-saving interventions are aimed at
securing an airway maintaining breathing supporting circulation.

45
Patient requires a life-saving intervention
• Does this patient have a patent airway? • Is the patient breathing? • Does the patient have a pulse? • Is the pulse rate, rhythm, and quality? • Was this patient intubated pre-hospital? • Is this patient's ability to deliver adequate oxygen to the tissues?

46
A key difference between ESI level-1 and 2
Immediate physician involvement in the care level-2 patients :the emergency nurse can initiate care through protocols without a physician at the bedside.

47
level-1 criteria patients who are pale, diaphoretic, in acute respiratory distress or hemodynamically unstable will require immediate life-saving interventions back

48
The emergency nurse can
initiate intravenous access, administer supplemental oxygen obtain an ECG on a cardiac monitor All before a physician presence is needed.

49
Patients with chest pain
must also be evaluated using the same criteria. Some patients presenting with chest pain are very stable. Although they may require a diagnostic ECG, these patients do not meet level-1 criteria.

50
ESI-level 1 Requires immediate life-saving intervention
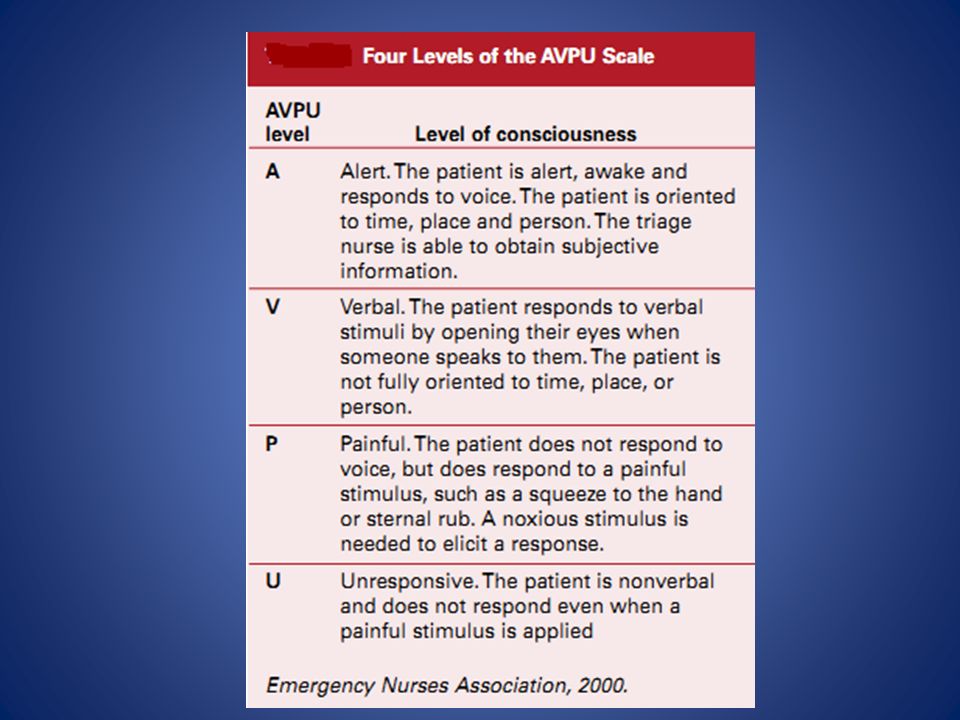
Assess an acute change in level of consciousness AVPU (alert, verbal, pain unresponsive) scale
 scale.")
52
Examples of ESI level 1 • Cardiac arrest. • Respiratory arrest.
• Severe respiratory distress. • SpO2 < 90. Baby that is flaccid. • Critically injured trauma patient who presents unresponsive. • Overdose with a respiratory rate of 6. • Chest pain, pale, diaphoretic, blood pressure 70/palp. • Weak and dizzy, heart rate = 30. • Severe bradycardia or tachycardia with signs of hypoperfusion. • Hypotension with signs of hypoperfusion. • Trauma patient who requires immediate crystalloid and colloid resuscitation. Hypoglycemia with a change in mental status

53
Examples of ESI level 2 • Active chest pain, suspicious for coronary syndrome, but does not require an immediate life-saving intervention, stable. • A needle stick in a health care worker. • Signs of a stroke, but does not meet level-1 criteria. • A rule-out ectopic pregnancy, hemodynamically stable. • immunocompromised+fever. • A suicidal or homicidal patient.

58
A 6-month-old baby with a cold +RR48
(ESI-2) BT is only included with children <3 yrs Significant fever may exclude children from ESI- 4 and 5
 BT is only included with children <3 yrs. Significant fever may exclude children from ESI- 4 and 5.")
59
ESI does not mandate specific time standards in which patients must be evaluated by a physician.
However, patients for ESI level 2 should be seen as soon as possible; up to the individual institution

60
care of ESI level-2 patients should be rapidly facilitated and patients should ideally wait
< 10 minutes to be placed in the treatment area.

61
Components of ESI level-2 criteria
1. Is this a high-risk situation? 2. Is the patient experiencing new onset confusion, lethargy, or disorientation? 3. Is the patient experiencing severe pain or distress?

63
based on the experienced triage nurse
sixth sense

65
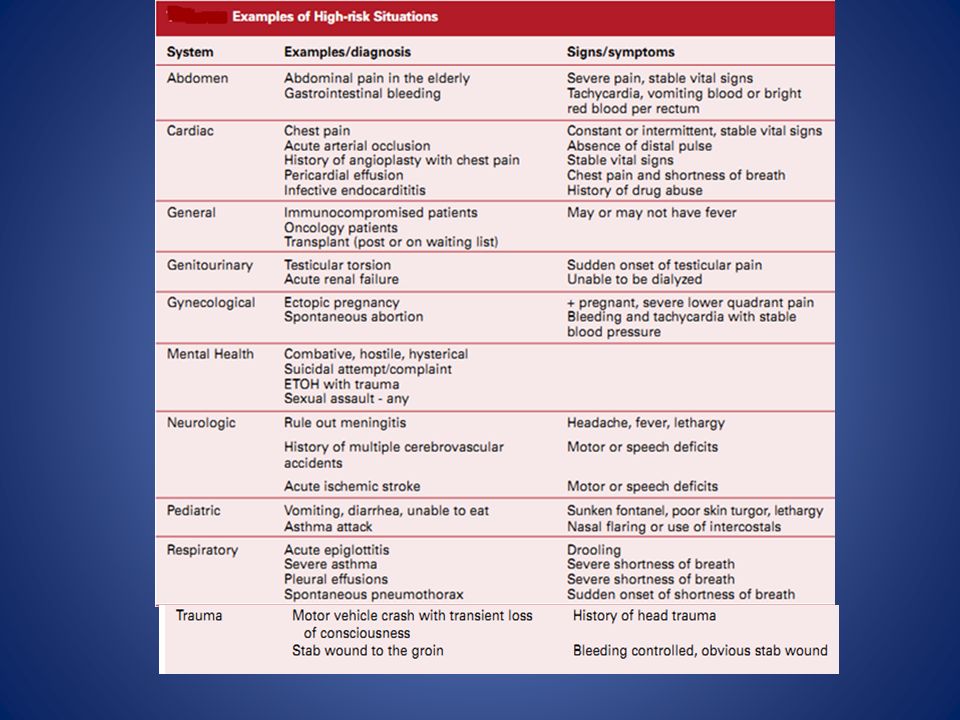
Examples of high-risk situations for children
• Seizures. • Sepsis, severe dehydration. • Diabetic ketoacidosis. • Child abuse, burns. • Head trauma. • Vitamins/iron or other overdoses/ingestions. • Infant less than 28 days of age with BT >38° C.

66
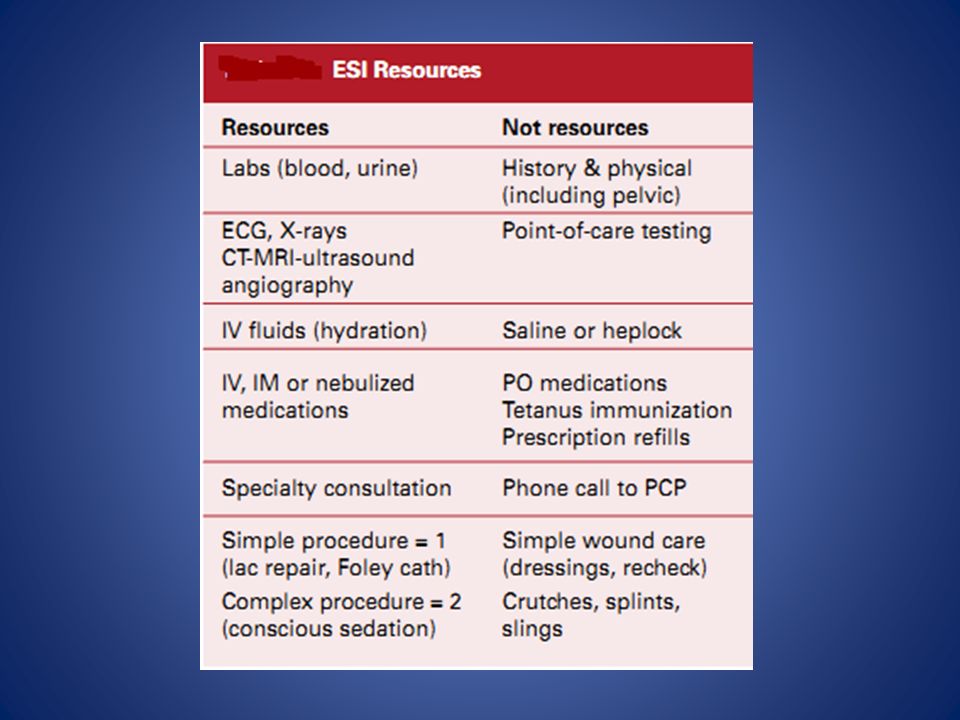
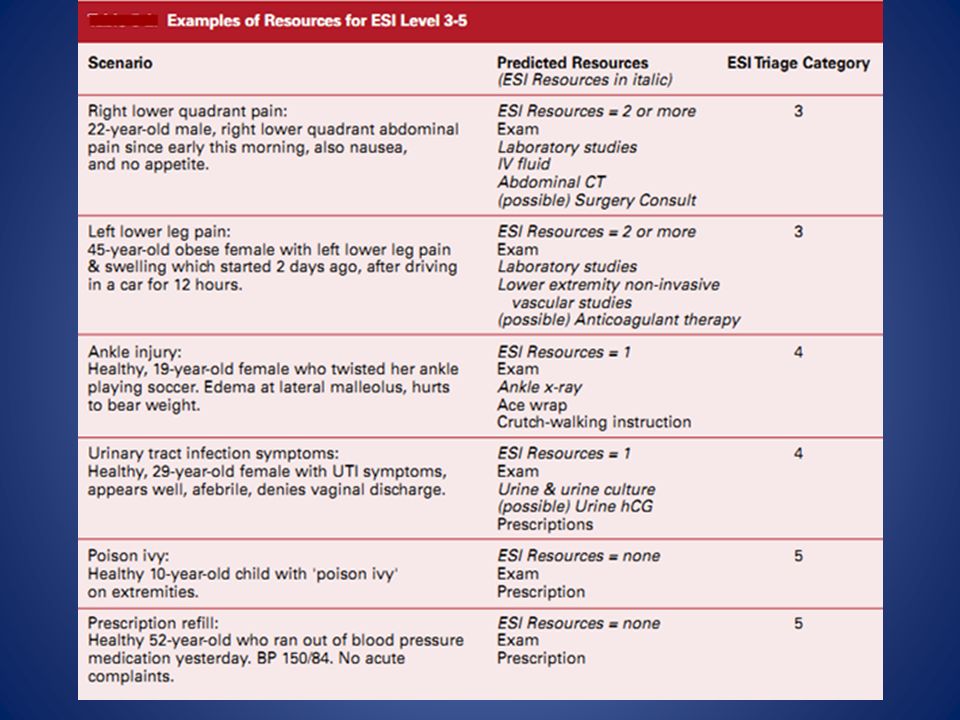
Resources needed • CBC and electrolyte comprise 1 resource (lab test). • CBC and chest x-ray are 2 resources (lab test, x-ray). • CBC and urinalysis are both lab tests and together count as only 1 resource. • chest x-ray and plain skull films are 1 resource (x-ray). • cervical-spine films and a CT scan of the head are 2 resources (x-ray and CT scan).
. • CBC and chest x-ray are 2 resources (lab test, x-ray). • CBC and urinalysis are both lab tests and together count as only 1 resource. • chest x-ray and plain skull films are 1 resource (x-ray). • cervical-spine films and a CT scan of the head are 2 resources (x-ray and CT scan).")
67
a splint eye irrigation (Patients with a chemical splash usually meet ESI level-2 criteria )
")
68
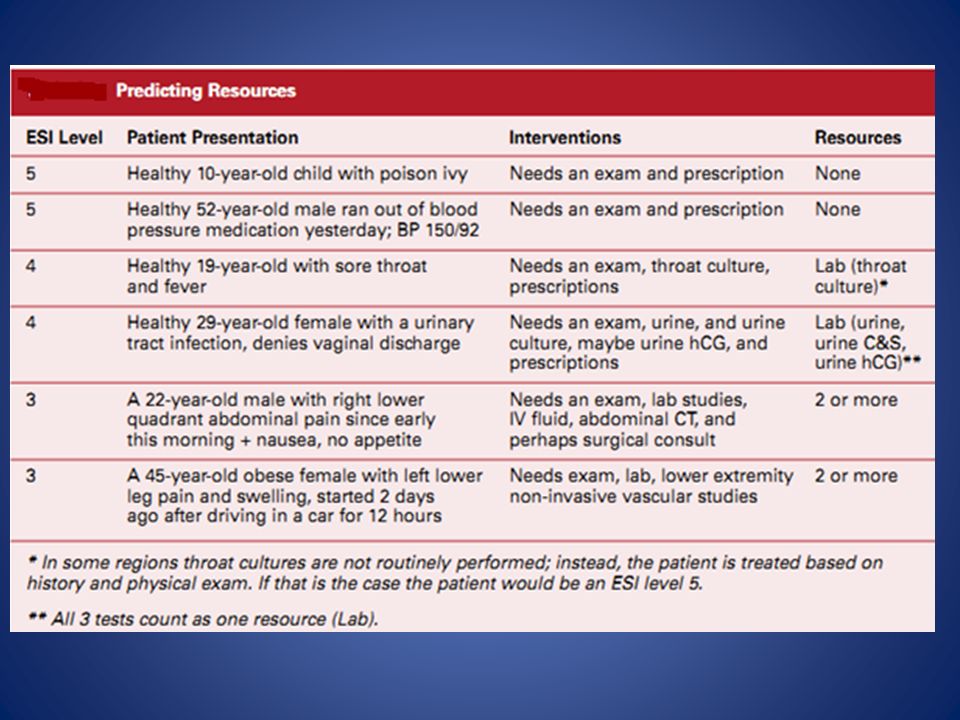
One ED practice variation that may result in different ESI levels for different sites is the evaluation of patients with an isolated complaint of sore throat. At some hospitals it is common practice to obtain throat cultures (one resource, ESI level 4), while at others it is not (no resources, ESI level 5).
, while at others it is not (no resources, ESI level 5).")
69
Summary ESI is a 5-level triage system that is simple to use and divides patients by acuity and resource needs. The ESI triage algorithm is based on 4 key decision points. The experienced nurse :rapidly and accurately triage patients using this system.

70
resources is included in the triage level assignment for ESI level-3, 4, and 5 patients.
ESI level-1 and 2 decisions are based only on patient acuity.

73
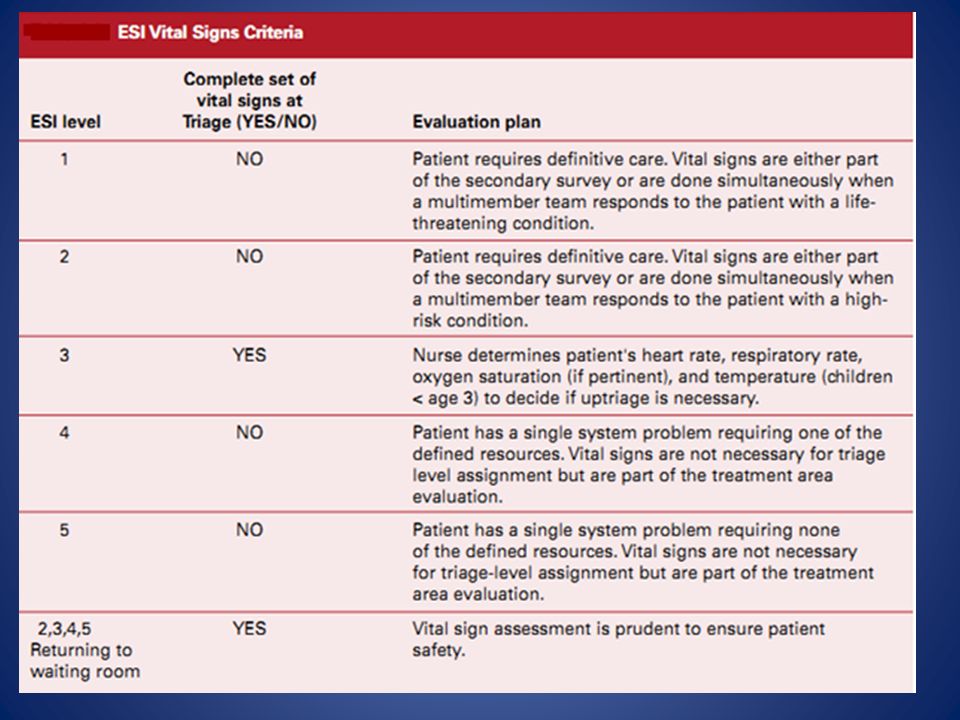
Vital signs can play a more important role in the evaluation of ESI level 3.
Temperature is specifically used in ESI triage for children < 3 yrs blood pressure is not included in the ESI The infant <28 days old with a fever should be considered high risk and assigned to at least ESI level 2.

74
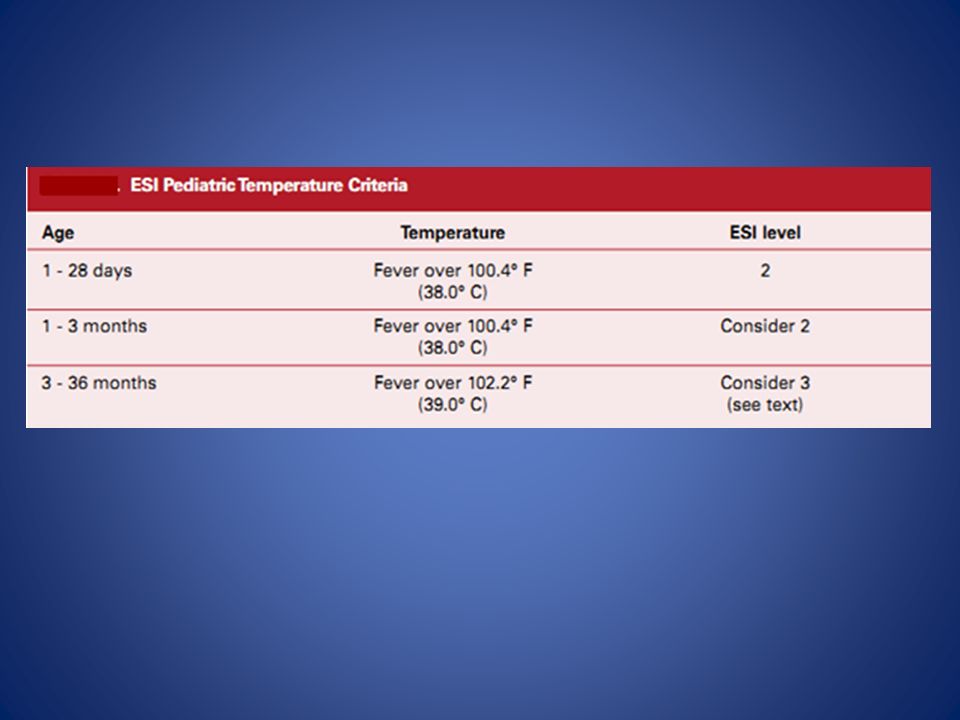
Pediatric fever <3 m- 3years old BT >39° C
assess immunization status +source of fever incomplete immunizations +/-no identifiable source of fever : ESI level 3. immunizations +/-identifiable source of fever : ESI level 4, 5

77
Evaluation and Quality Improvement
• Reduction in variation of assigned triage categories. • Decreased risk of negative outcomes due to mis- triage, particularly while patients are waiting. • The ability to obtain more accurate data to use for administrative purposes. The need to move from a 3-category to a 5-category triage system to better “sort” the increasing number of ED patients. • A more accurate description of patient triage level

78
Goal of ESI accurately capture patient acuity
to optimize the safety of patients in the waiting room by ensuring that only patients stable to wait are selected to wait.

79
ESI triage alone cannot decrease the ED length of stay nor improve customer satisfaction with the ED visit. The continued success of ESI triage is including the evaluation of triage in the overall quality improvement (QI) plan for the ED.
 plan for the ED.")
80
ESI quality indicators
• Accuracy of ESI triage category rating by the triage nurse. • Rates of under and over-triage. • Review of all negative outcomes which occurred due to a mis-triage. • Measurement of time from patient arrival to being seen by a physician for each ESI triage category. • Measurement of length of stay for each ESI triage category. • Measurement of admission rates for each ESI triage category. • Review of patients rated ESI level 4 and 5 who are admitted to the hospital.

81
+ the under-triage rate at 20 % of the mis-triages.
Should the triage category be correct 90%? The triage accuracy threshold might be 80 % + the under-triage rate at 20 % of the mis-triages. To determine how many triage indicators should be monitored on

82
It is also possible to focus on monitoring one aspect of triage for a period of time, and then switch to another indicator when improvement occurs in the previously monitored indicator.

83
Accuracy of triage acuity level should probably be monitored on a continuous basis to evaluate new triage nurses as well as monitor for trends which may identify the need for re-education on a particular aspect of triage.

84
when monitoring QI indicators, it is important to determine how many charts must be reviewed for each indicator and how frequently the indicator should be reviewed (monthly, quarterly, etc.). The selection of the appropriate number of charts for each indicator will again depend on the particular indicator.

85
Cases from different nurses and each shift and day of the week should be reviewed.
10% of all cases are often selected as an “appropriate” number of cases to review. In a busy ED, this is an unrealistic number.

86
Case1 “I just turned my back for a minute,” cried the mother of a 4-year-old. The child was pulled out of the family pool by a neighbor who immediately administered mouth-to-mouth resuscitation. The child is now breathing spontaneously but continues to be unresponsive. On arrival in the ED vital signs (VS) were: HR 126, RR 28, BP 80/64, SpO2 96% on a non- rebreather.
 were: HR 126, RR 28, BP 80/64, SpO2 96% on a non- rebreather.")
87
ESI level 1: unresponsive.
This 4-year-old continues to be unresponsive. The patient will require immediate life-saving interventions to address airway, breathing, and circulation.

88
Case 2 A 28-year-old male presents to the ED requesting to be checked.
He has a severe shellfish allergy and mistakenly ate a dip that contained shrimp. He immediately felt his throat start to close so he used his EpiPen®. He tells you he feels okay. No wheezes or rash noted. VS: BP 136/84, HR 108, RR 20, SpO2 97%, temperature (T) 97° F.
 97° F.")
89
ESI level 2: high-risk situation for allergic reaction.
The patient has used his EpiPen but still requires additional medications and close monitoring.

90
Case 3 “He was running after his brother, fell and cut his lip on the corner of the coffee table. There was blood everywhere,” recalls the mother of a healthy 19-month-old. “He'll never stay still for the doctor.” You notice that the baby has a 2- cm lip laceration that extends through the vermillion border. Vital signs are within normal limits for age.

91
ESI level 3: two or more resources.
A laceration through the vermillion border requires the physician to line up the edges exactly. Misalignment can be noticeable. A healthy 19-month-old will probably not cooperate. In most settings he will require conscious sedation, which counts as 2 resources. The toddler's vital signs are within normal limits for age, so there is no reason to up-triage to ESI level 2.

92
The End

งานนำเสนอที่คล้ายกัน







>")













